
Abstract
Aim: The purpose of this study was to use measurements from cone beam computed tomography scans to quantify the cortical bone thickness of mandibular buccal shelf region and preferable site for buccal shelf implant placement in 10 hyperdivergent and 10 hypodivergent patients.
Method: 20 cone beam computed tomographies were equally divided based on divergence. 6 sites were examined: mesial of first molar (6M), middle of first molar (6Mi), interdental between the first and second molar (Id), mesial of second molar (7M), middle of second molar (7Mi), and distal of second molar (7D). The study quantified the mandibular buccal shelf relative to its angle of slope, the cortical bone thickness measured perpendicular to the bone surface, the amount of cortical bone 30° angle to the bone surface. The cortical bone thickness was measured perpendicular and at a 30° angle at 3, 5, and 7 mm from the alveolar crest.
Result: Significant change is seen at the buccal shelf slope at 6M (P = .001) and further increase in this angle till 7D (P = .003). Mean amount of cortical bone for hyperdivergent group at 7D is 4.77 ± 0.68 mm and for hypodivergent group is 3.86 ± 0.70 mm. Statistically significant differences were noted at insertion site at 90° and 30° for both groups at 3, 5, and 7 mm from the alveolar crest.
Conclusion: Preferable site for buccal shelf implant placement is distal to the mandibular second molar. The maximum amount of cortical bone is found distal to the second molar 7 mm vertically from alveolar crest when the buccal shelf implant is placed at 30° angulation for hyperdivergent group.
Introduction
The extra-alveolar sites for the placement of mini-implant are selected depending on the biomechanics to be used and the quality of bone present at the site of placement. At present, the mandibular buccal shelf (MBS) area is used for mini-screw insertion mainly for the correction of class III problems and correction of severe skeletal and dental malocclusions without extractions or extensive surgical procedures. 1 There are a gamut of variations when it comes to selecting the site of implant placement in the buccal shelf area because of varying mandibular anatomy. Thus, with the assumption that mandibular anatomy varies in patients with different facial divergence, the site and angulation of buccal shelf implant placement also differs as per the anatomy. Henceforth, it is important to determine the cortical bone thickness of the buccal shelf area and the site of buccal shelf implant placement in individuals with different facial divergence. Moreover, authors suggest that placing the mini-implant at an angle to the bone surface increases the bone contact. Studies also suggest that to distalize the entire mandibular arch, the mini-screw should be placed at an angle perpendicular to the occlusal plane.2, 3
The purpose of this study was to record measurements from cone beam computed tomography scans to quantify the cortical bone thickness of MBS region and find out the preferable site for buccal shelf implant placement in 10 hyperdivergent and 10 hypodivergent patients. The study gauges MBS relative to:
The angle of slope, which is measured between the outer cortical outline of the buccal shelf area and the long axis of the respective molar The cortical bone thickness which is measured at 90° to the outer buccal cortex The amount of cortical bone engagement when the screw is placed lateral to the molar roots, approximately perpendicular to the occlusal plane, ie, 30° angle to the outer buccal cortex.
Material and Methods
Sampling
Purposive sampling was done retrospectively by collecting 20 pretreatment cone beam computed tomography scans of adult patients with the age range of 19 to 25 years (10 hypodivergent and 10 hyperdivergent) from the preexisting college records.
Inclusion criteria: All the included subjects were of Indian origin. Subjects who have not undergone orthodontic or orthopedic intervention were included. Groups were classified based on the Frankfort mandibular plane angle (FMA < 22° were included in hypodivergent group whereas FMA > 27° were included in hyperdivergent group), ascending ramus, mandibular base length, Jarabak ratio and Downs Y-axis, and subjects with healthy periodontium and adequate alveolar bone support were included in the study (alveolar crest 1.5–2 mm apical to cementoenamel junction).
Exclusion criteria
Measurements Recorded
6 sites were examined on the right side of mandible (as there is bilateral symmetry): mesial of first molar (6M), middle of first molar (6Mi), interdental between the first and second molar (Id), mesial of the second molar (7M), middle of the second molar (7Mi), and distal of the second molar (7D; Figure 1). The subsequent bone measurements were carried out on coronal section and curved slicing in cone beam computed tomography scans at the above mentioned 6 sites. The alveolar crest was the horizontal baseline.
The angle of slope was measured between the cortical outline of the buccal shelf area and the long axis of the respective molar (Figure 2a).
The cortical bone thickness was measured at 90° and 30° angle as shown at 3, 5, and 7 mm from the alveolar bone crest (Figure 2a,b,c).
Bone engagement depth of an 8-mm mini-implant is 3 mm, of a 10-mm bone screw is 5 mm, and of a 12-mm bone screw is 7 mm; and therefore, 3, 5, and 7 mm measurements were selected from the alveolar crest.
All the collected data were analyzed on the Carestream dental (CS 3D [Carestream dental, Rochester, NY, USA]) imaging software.
Sites Examined Are Marked with Purple Lines
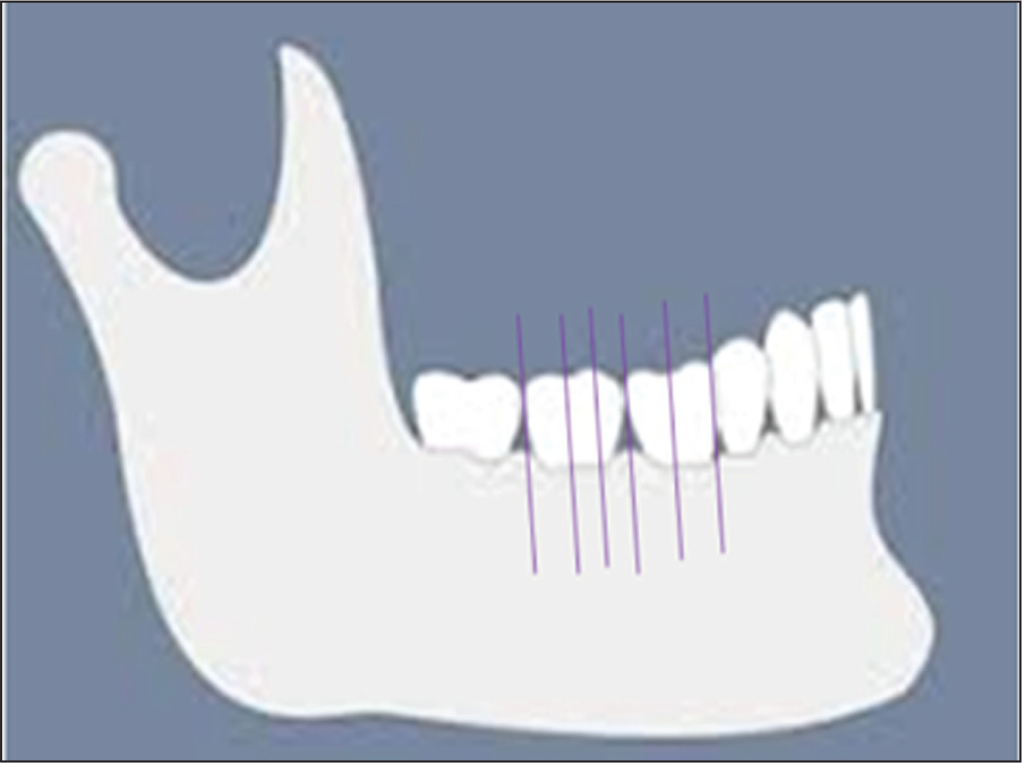
Figure 2. (a) 3, 5, and 7 mm Vertically Down From the Alveolar Crest and Angle of the Slope of the Mandibular Buccal Shelf (b) Measurement of Cortical Bone Thickness at 90° to the Outer Buccal Cortex and 7 mm Vertically Down From the Alveolar Crest (c ) Measurement of Cortical Bone Thickness at 30° Angulation and 7 mm Vertically Down From the Alveolar Crest

Results
Data were analyzed using SPSS version 23. Descriptives, one-way analysis of variance for intragroup comparison, independent t-test for intergroup comparison, paired t-test for interangle (30° and 90°) comparison, and P ≤ .05 was considered significant.
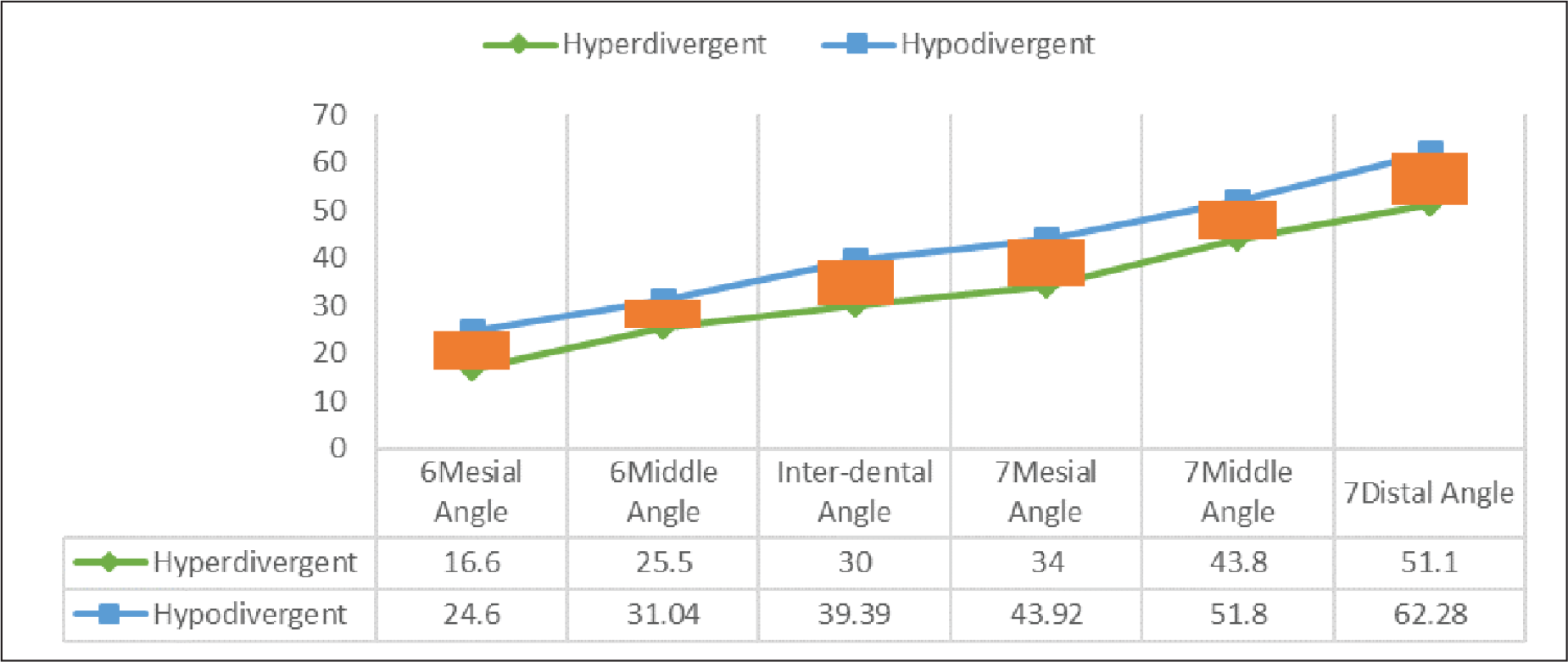
A significant change in anatomy was seen at the angle of buccal shelf slope at the mesial of first molar (P = .001), mesial of second molar (P = .008), distal of second molar (P = .003; Figure 3).
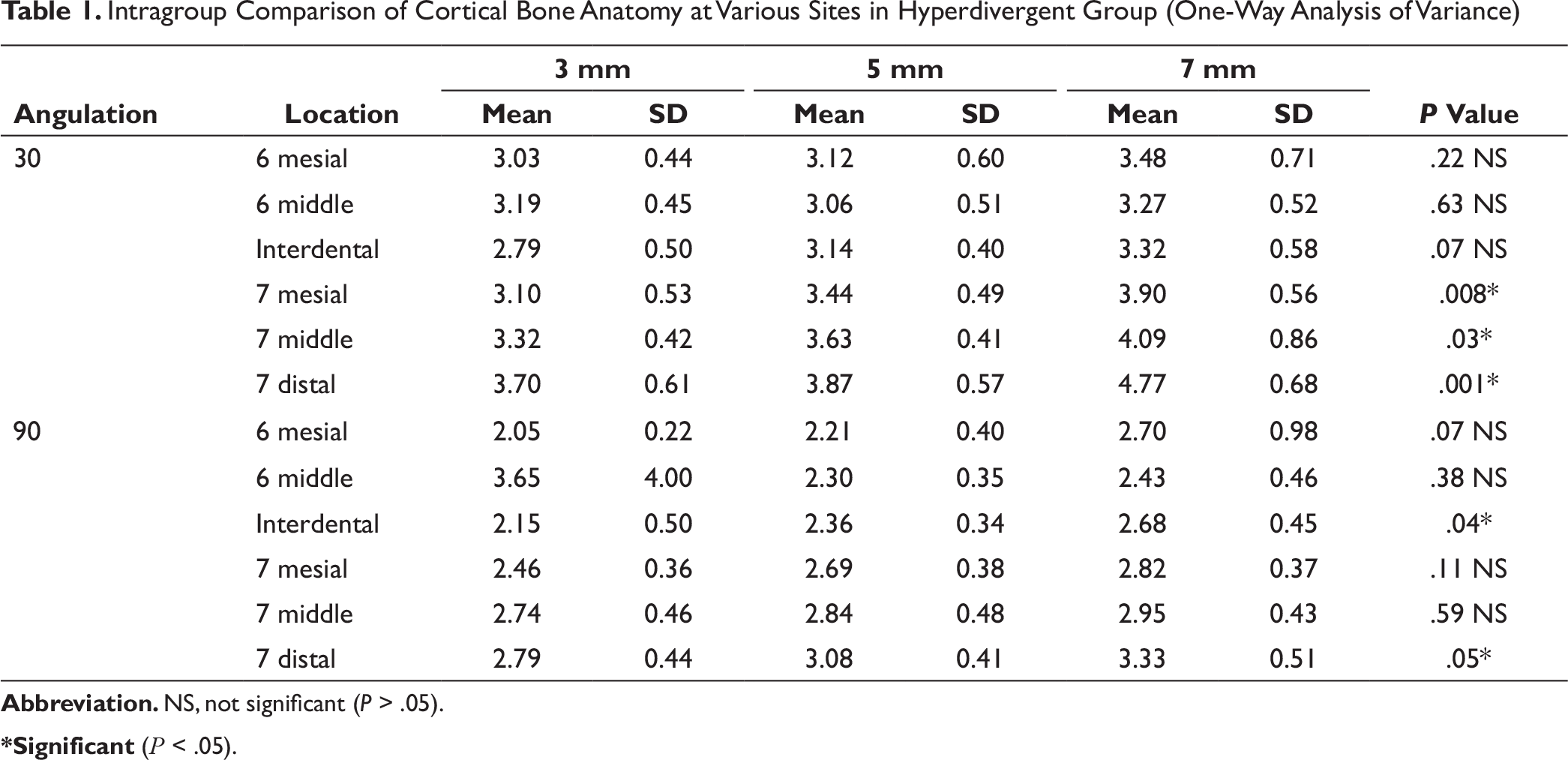
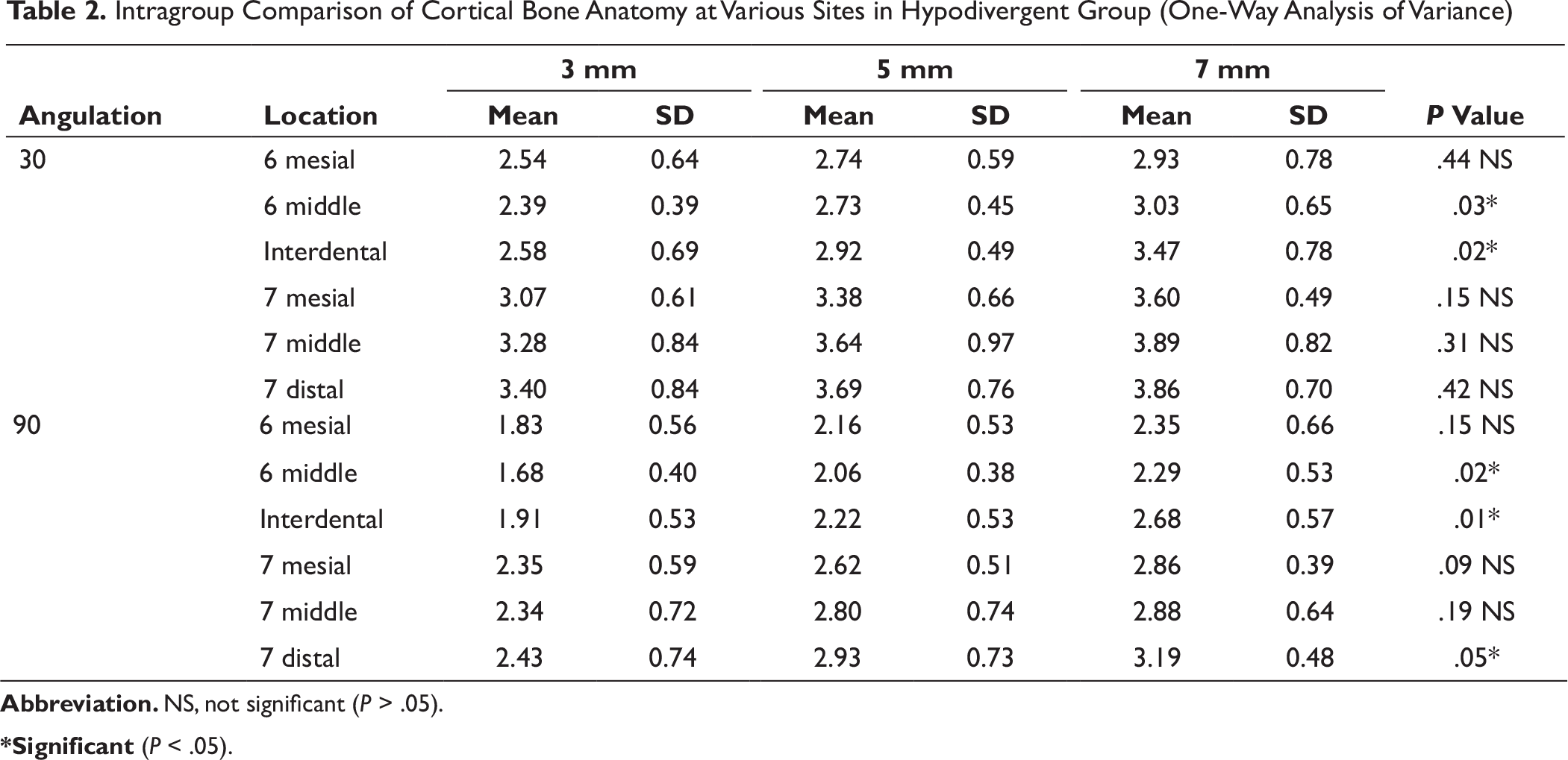
Intragroup comparison of cortical bone anatomy of MBS for hyperdivergent group showed statistically significant differences at 3, 5, and 7 mm from the alveolar crest. At 30° angulation, significant differences were noted at the mesial (P = .008), middle (P = .03), and distal (P = .001) of the mandibular second molar. At 90° angulation, a significant difference was present at the interdental (P = .04) between the first and the second molar and distal to the second molar (P = .05; Table 1). Intra-group comparison of cortical bone anatomy of MBS for hyperdivergent group showed statistically significant differences at various sites at 3, 5, and 7 mm from the alveolar crest (Table 2). The maximum mean amount of cortical bone for hypodivergent group distal to the second molar is 4.77 ± 0.68 mm at 30° angulation and for hypodivergent group is 3.86 ± 0.70 mm at 30° angulation, and at the middle of the second molar for hyperdivergent group this value is 4.09 ± 0.86 mm and for hypodivergent group it is 3.89 ± 0.82 mm at 30° angulations (Table 5).
Intragroup Comparison of Cortical Bone Anatomy at Various Sites in Hyperdivergent Group (One-Way Analysis of Variance)
Intragroup Comparison of Cortical Bone Anatomy at Various Sites in Hypodivergent Group (One-Way Analysis of Variance)
Interangle Comparison at 3 mm
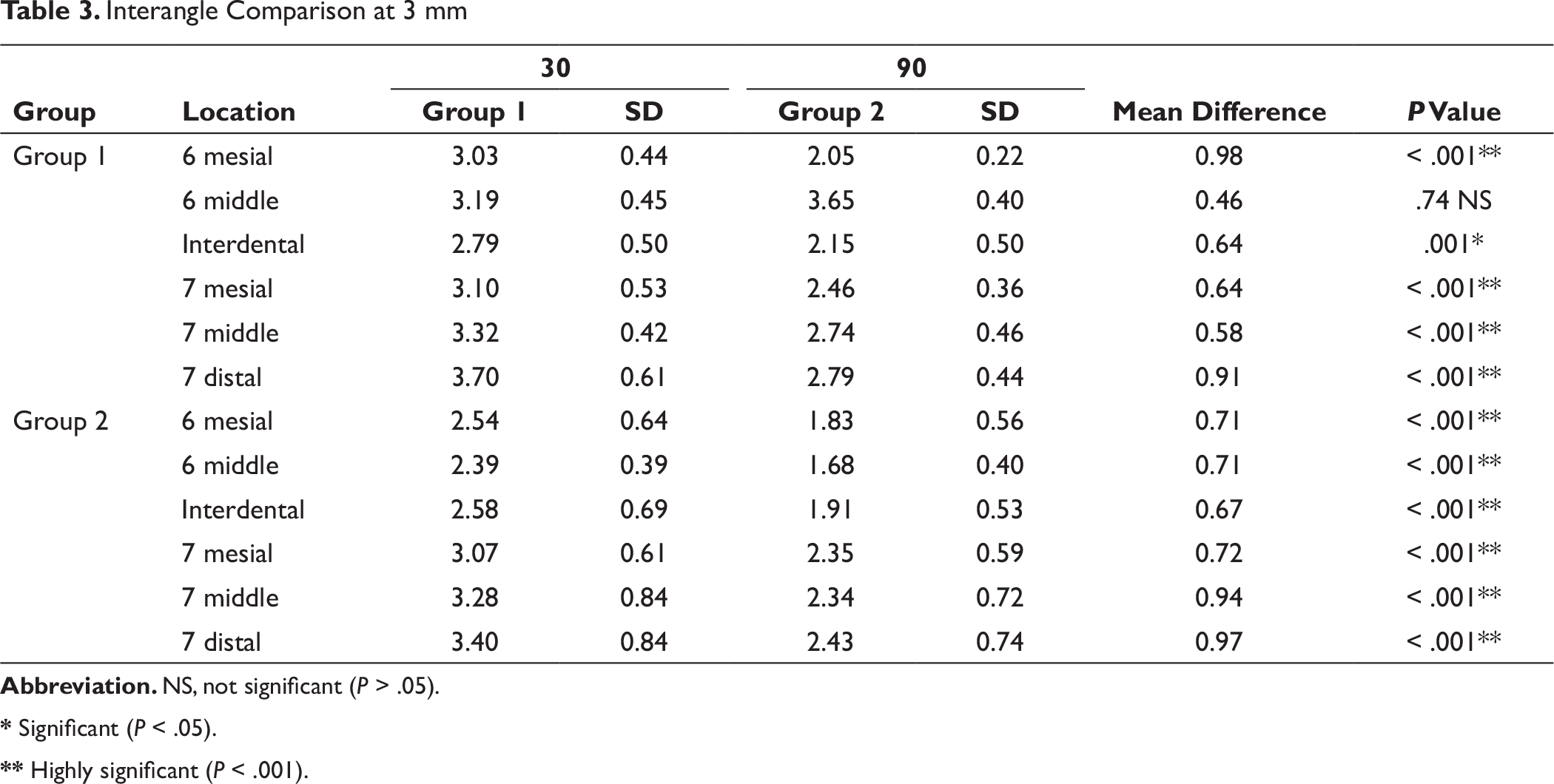
* Significant (P < .05).
** Highly significant (P < .001).
Interangle Comparison at 5 mm
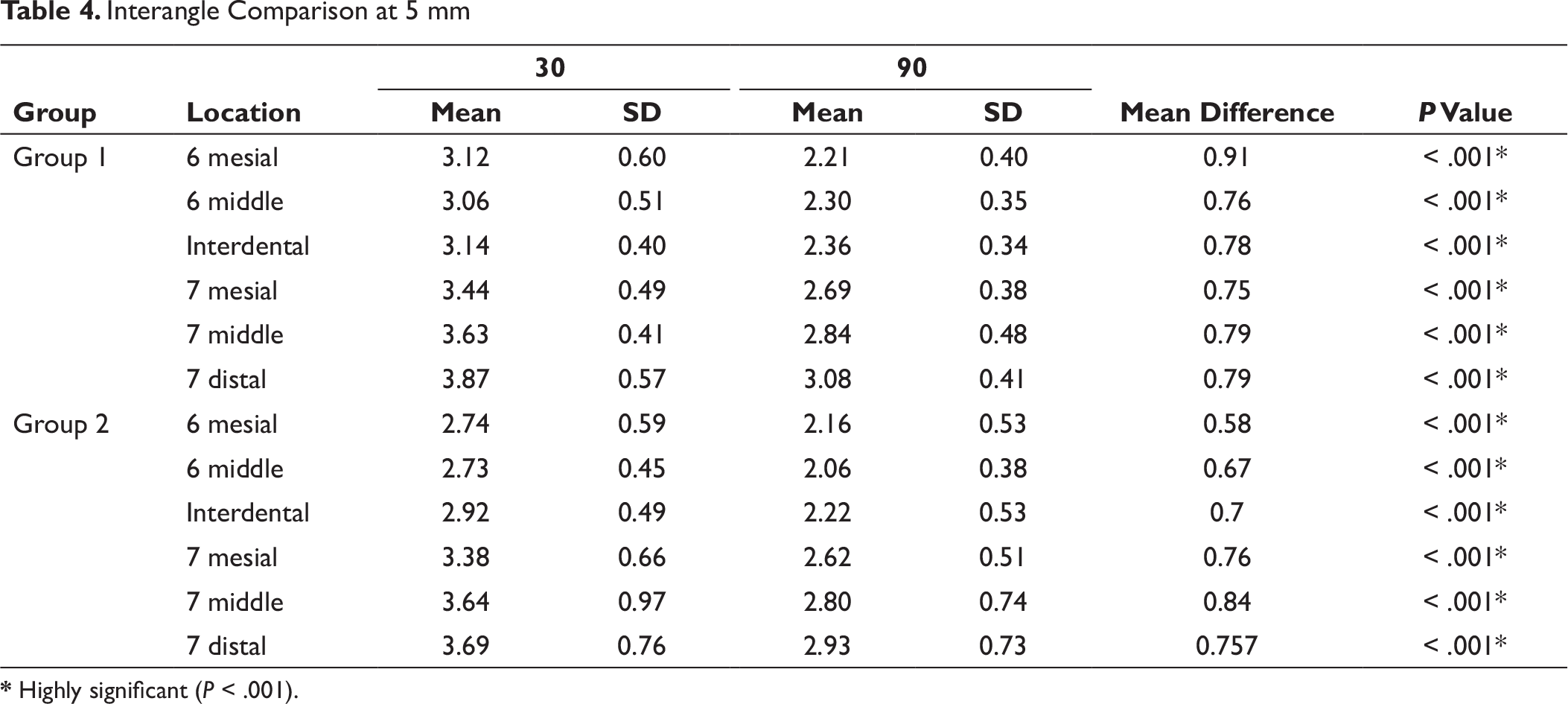
* Highly significant (P < .001).
Interangle Comparison at 7 mm
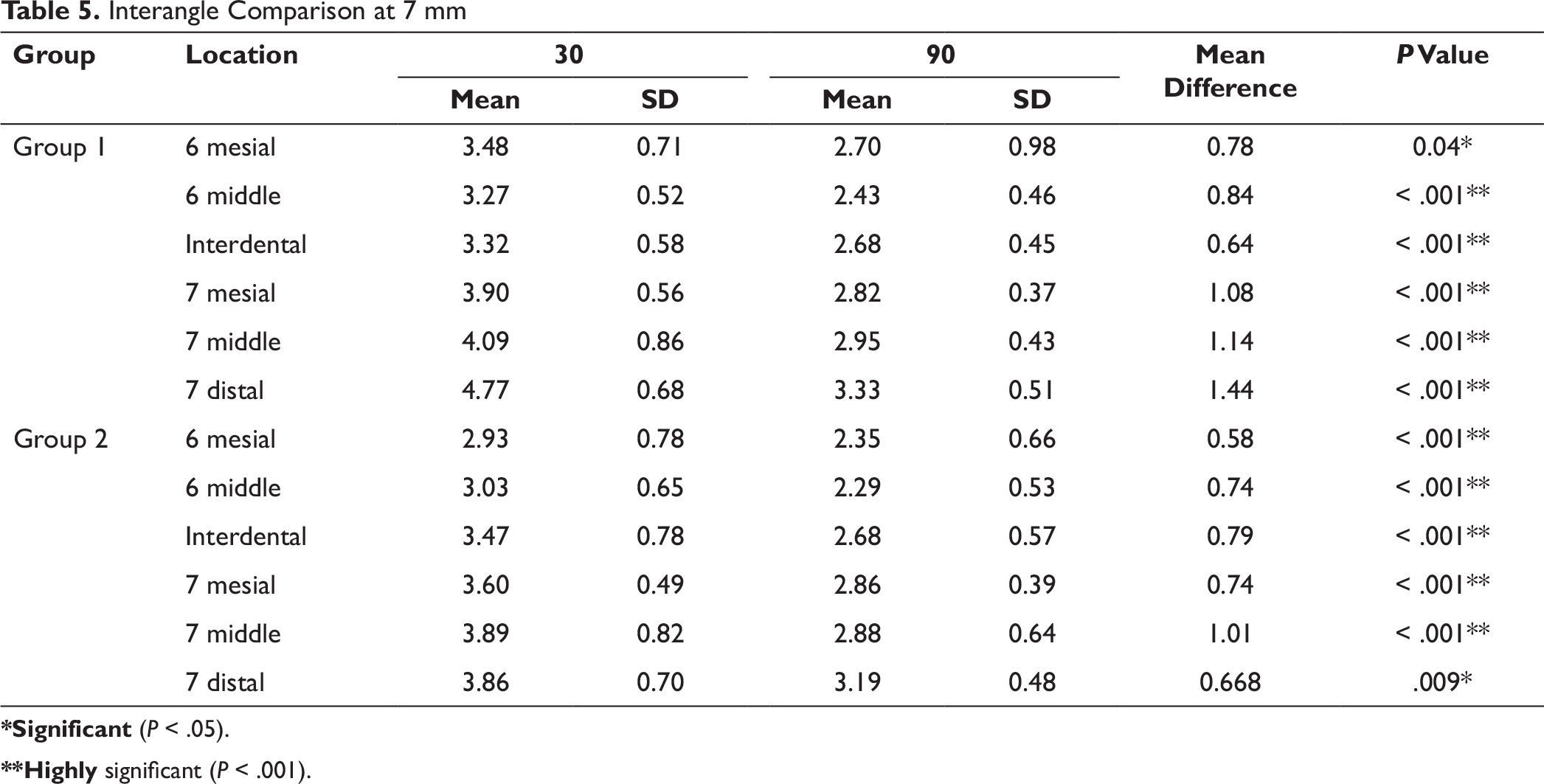
*Significant (P < .05).
**Highly significant (P < .001).
Comparative Evaluation of Angular Measurements in Hyperdivergent and Hypodivergent Groups
Discussion
Newton’s third law of motion states: “For every action, there is an equal and opposite reaction.” 4 This law is also applicable in orthodontics: for every desired tooth movement, there is a potential to create an undesired tooth movement. This was the problem when teeth were used as anchor units. Inspired by the stability of prosthodontic implants, orthodontists modified the use of these implants for absolute anchorage purpose. 5
These mini-screws provide absolute anchorage by absorbing the reactive forces and transmitting it to skeletal structures, thus the undesirable side effects can be prevented entirely. As they are anchored directly on the skeletal structures, no root to mini-implant contact occurs and hence no damage to the root happens. 6 Also, a long range of action can be achieved. Owing to all these advantages, we can easily distalize the entire dentition and borderline surgical cases were converted into nonsurgical cases. Moreover, we can achieve a three-dimensional control on the applied orthodontic or orthopedic forces along with maintaining the integrity of both maxillary and mandibular arches.7, 8
Facial divergence of an individual has an important role in determining the type of biomechanics to be used in orthodontics. There is always more anchorage requirement in individuals with hyperdivergent growth pattern as compared to hypodivergent growth pattern. The anatomy of the mandible, and thus the buccal shelf area, is different in hyperdivergent and hypodivergent growth patterns. It becomes mandatory to have adequate knowledge of anatomy as well as the amount of cortical bone available at the site of insertion of the bone screw.
Two popular sites of extra-alveolar placement of mini-screw are infra-zygomatic crest and buccal shelf area. Bone screws are manufactured of pure stainless steel.9, 10 Bone screws are generally placed in areas of D1 ( > 1250 HU) quality bone 11 and therefore require greater fracture resistance. Stainless steel provides greater fracture resistance than titanium alloy and, therefore, it is the material of choice.
This study focuses on the facial divergence pattern of an individual, as the anatomy of the mandible is different in patients of different facial divergence because of the muscle forces. It was interesting for us to find out the difference in the anatomy of the buccal shelf area, the site of implant placement, and the buccal cortical bone thickness for these 2 groups.
Power analysis was performed with the GPower 3.1 software for the sample size selection. (Effect size = 0.282, α = 0.05), (1-β) = 0.80, and (N2/N1 = 1)
In the present study, 6 sites were examined: mesial of the first molar, middle of the first molar, interdental between the first and second molar, mesial of the second molar, middle of the second molar, and distal of the second molar.
Angular measurements of the slope of buccal shelf area to the respective molar show broader buccal shelf area in hypodivergent group (increased angular measurements) as compared to hyperdivergent group. A significant change in anatomy was seen at the angle of buccal shelf slope at mesial of first molar (P = .001), second molar mesial (P = .008), second molar distal (P = .003; Figure 3). Thus, an interesting finding is that in hypodivergent individuals, because of broader buccal shelf area, the screw can be placed farther from the dentition compared to the hyperdivergent individuals.
The results obtained suggest that the favorable site of buccal shelf implant placement is distal to the second molar which correlates with the study of Baumgaertel. 12 Similar study carried out by Liu et al at Guangzhou Medical University concluded that the ideal site for buccal shelf implant placement is between distobuccal of first molar and mesiobuccal of the second molar. The growth pattern of an individual was not considered in this study. 13 The present study accounts for the facial divergence, and the site for buccal shelf implant placement between distobuccal of the first molar and mesiobuccal of the second molar is suitable when the screw is placed at an obtuse degree angulation. A significant finding of our study is that the amount of cortical bone available is more when the buccal screw is inserted at 30° to the occlusal plane which is in accordance with the study of Chang et al. We found high statistically significant differences in the angulation of bone placement distal to the second molar for both the hyperdivergent and hypodivergent groups.
The anatomy of the mandible, and thus the buccal shelf area, is different in hyperdivergent and hypodivergent growth patterns. The hyperdivergent group has flat mandibular anatomy and hence a narrow buccal shelf area when compared to the hypodivergent group. Mean amount of cortical bone when the screw is placed at 30° for hyperdivergent group distal to the second molar is 4.77 ± 0.68 mm and for hypodivergent group is 3.86 ± 0.70 mm. 14 Another statistically significant site for implant placement is middle of mandibular second molar at 30° where the mean amount of cortical bone for hyperdivergent group is 4.09 ± 0.86 mm and for hypodivergent group is 3.89 ± 0.82 mm.
Thus, a good amount of cortical bone is available at both 90° and 30° angulations for both the groups, when the screw is placed distal to the mandibular molar. However, comparatively more bone is available at 30° angulated placements. The difference in the mean cortical bone at 90° and 30° is more in hyperdivergent group than in hypodivergent group. Whereas, for the middle of the second molar only 30° angulated placements are favorable for both groups.
When a mini-implant is placed distal to mandibular second molar, the proximity of nerve should be examined. According to the study of Elshebiny et al, the distance between the nerve and mini-implant placed distal to mandibular second molar is safe enough for the placement without damaging the nerve. 15
The thickness of the soft tissue affects the stability of mini-screw. This study was focused on the bony architecture of the buccal shelf area and soft tissue parameters were not taken into consideration.
Conclusion
The optimal site for buccal shelf implant placement is distal to the mandibular second molar. Another suitable site is middle of mandibular second molar at an obtuse angulation of placement.
Hyperdivergent individuals have narrow buccal shelf area compared to the hypodivergent individuals.
The maximum amount of cortical bone was found distal to the second molar at 7 mm vertically from alveolar crest when the implant was placed at 30° angulation for both the groups. The difference in the cortical bone thickness at 90° and 30° is more in hyperdivergent group than hypodivergent group.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.