
Abstract
Patients with a skeletal class II malocclusion are usually associated with a prognathic maxilla with orthognathic mandible or a retrognathic mandible with orthognathic maxilla or a combination of both. Patients with severe prognathic maxilla are usually associated with increased overjet which results in a lower lip trap. The lip trap should be managed the earliest as it will lead to further proclination of the upper anterior teeth and also hinder the normal growth of the mandible. To overcome the limitations of a conventional lip bumper, we arrived at an idea of fixed lip bumper supported using mini-implants.
Introduction
Management of habitual lip trap or lip sucking will be the first line of treatment in the patients with severe skeletal class II with lower lip trap, as it will hinder the treatment and also will aggravate the malocclusion. The most common method of managing lip trap is by using habit breaking appliance such as a lip bumper. Lip bumpers are usually contraindicated in patients in whom the first molars are not fully developed, or when there is less than 50% root formation in the permanent second mandibular molars, when the permanent molars are ankylosed or periodontally compromised or in cases where the permanent first molars are already upright in the transverse and the sagittal plane.
Limitations for fabricating a lip bumper are primarily when the first molars are not fully developed. Another drawback with the conventional lip bumpers taking anchorage from the first molars is the increased probability of impaction of permanent second molars. 1 In such clinical situations, a novel design of a mini-implant-supported lip bumper would be beneficial.
Appliance Design
The appliance consisted of a lip bumper made of acrylic which is held in position by obtaining anchorage from bone in the mandibular anterior region using mini-implants. Under local anesthesia, 2 mini-implants of size 1.5 mm × 8 mm dimension were inserted with the help of drivers in the lower anterior region by self-drilling method.
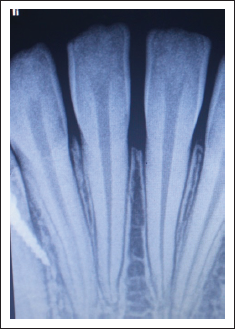
The mini-implants were inserted distal to the mandibular lateral incisor on both sides (Figure 1). The site of insertion of mini-implants was decided based on the biomechanical advantage that can be obtained from the appliance after insertion and was cross-checked using intraoral periapical radiographs taken prior to the insertion of the mini-implants for any other interference such as root. After insertion of mini-implants, radiographs were taken to confirm any damage to the adjacent roots (Figures 2 and 3).
Mini-implants 1.5 mm × 8 mm in Dimension Were Inserted Distal to the Mandibular Lateral Incisor.

Anterior IOPA Radiograph Showing Site of Insertion of Mini-Implant 1.

Anterior IOPA Radiograph Showing Site of Insertion of Mini-Implant 2.
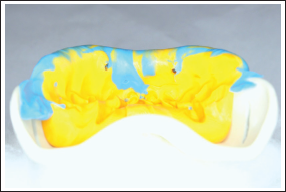
A lower anterior sectional elastomeric impression was taken with the mini-implants in position (Figure 4). Before pouring the impression, mini-implants of the same size were placed on their sites on the impression to provide us a custom model for fabrication of the appliance.
Lower Anterior Sectional Elastomeric Impression Was Taken With the Mini-implants in Position.
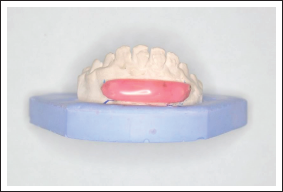
The laboratory procedure involved fabrication of a wire component which acted as a framework to support the acrylic component of the lip bumper. The lip bumper is attached to the mini-implants using precision attachments where the mini-implant acts as the key. The keyhole of the precision attachment is present in the inner aspect of the acrylic component which consists of a standard retention cap with steel housing from Rhein’83(Italy) and a rubber ring (Figure 5). This rubber ring helps in snugly holding the lip bumper to the mini-implants. By this method, the anchorage for the lip bumper is obtained from the bone (Figures 6 and 7) rather than the permanent mandibular first molar which is usually seen in a conventional lip bumper. The pre- and post-treatment pictures after usage of lip bumper are given in the Figures 8 and 9, respectively.
Lip Bumper Attached to Mini-implants Using Precision Attachment.

Mini-implant-Supported Lip Bumper Attached to the Model.
Mini-implant-Supported Lip Bumper in Patients.

Pre-treatment Extraoral Profile Picture.

Post-treatment Extraoral Profile Picture.

Conclusion
Habits creating malocclusions should be intervened at the earliest. This novel method of fabricating a mini-implant-supported lip bumper was found to be stable and effective in correcting a lip trap.
Footnotes
Statement of Informed Consent
Written informed consent was obtained from the subject for the use of photographs for publication
Acknowledgment
We would like to acknowledge Dr Faizur Rahman for helping us in the fabrication of the appliance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.