
Abstract
Class II malocclusion is one of the most commonly seen malocclusions in the orthodontic practice, with a variety of treatment modalities found in the literature. Maxillary molar distalization is a one of treatment options of dental Class II patients with excessive overjet, anterior crowding, or both. However, a commonly seen side effect in the conventional distalization devices is anchor loss. Here, in this case report, we have shown the successful treatment of a Class II malocclusion patient with a new concept of modified placement of the hybrid hyrax appliance, which was used effectively for en-masse, bodily distalization of maxillary teeth, with no anchorage loss. Also, the same appliance could be used for retention after the active distalization period till the treatment completion.
Introduction
Class II type of malocclusion is one of the most commonly encountered type of malocclusion in the practice of orthodontics. Treatment of Class II malocclusion in adults usually involves extractions of either two maxillary premolars or premolars in both arches, or it may involve distalization of maxillary teeth into a Class I relationship.1–3 Conventionally, extraoral appliance, such as headgear, is used for distalization of the upper dentition. However, the main disadvantage with extraoral appliances is the need for patient compliance, and also, it is unesthetic in appearance. 4
Intraoral devices such as highly elastic NiTi coil springs, repelling magnets, Jones-jigs, pendulum appliance, distal-jets, and others have been available since the 1980s, to distalize molars with a minimal amount of patient cooperation.5, 6 All of these methods adequately distalize both the first and second molars, but they may also lead to anchor loss, which is characterized by the protrusion of the maxillary incisors, and an increase in overjet “and overbite”. The average tooth movement achieved by commonly used intraoral distalizing appliances was 71% molar distalization, and 29% loss of reciprocal anchorage. 7
Recently, intraoral molar distalization devices supported by implants have been developed to offer adequate anchorage and lessen these side effects.8, 9 To minimize the surgical invasiveness in pure bone borne appliances, Wilmes and colleagues introduced the Hybrid Hyrax Distalizer, a new appliance for Class III malocclusion treatment that helps facilitate both palatal expansion and molar distalization. To provide sagittal anchorage and prevent the mesial migration of the maxillary teeth, it consists of two mini-implants in the anterior part of the palate. 10
This case report demonstrates the effective management of a Class II malocclusion in a female patient, with distalization of the maxillary teeth, that was successfully achieved with a modified hybrid-hyrax appliance.
Diagnosis and Treatment Planning
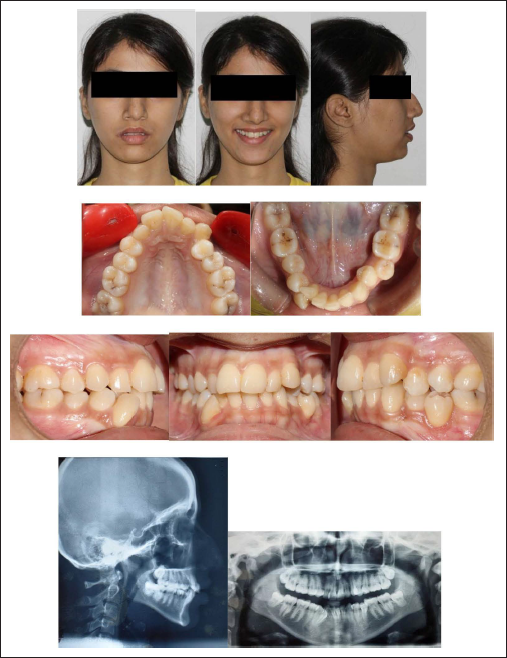
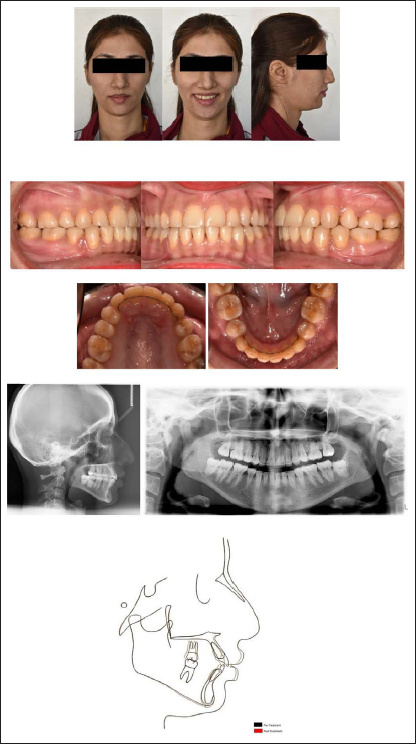
A 17-year-old female reported with the chief complaint that her upper and lower front teeth were irregularly placed. She gave a history of extraction of her permanent right maxillary canine (13). Extraoral clinical analysis showed a convex profile, mesoprosopic facial type, and incompetent lips. She had an end-on molar relationship bilaterally, and an end-on canine relationship on the left side; the maxillary and mandibular midline was shifted 2 mm to the right with respect to the facial midline. The lower right canine (43) was buccally placed and a unilateral crossbite was present with respect to the lower left second premolar (35). She exhibited severe maxillary crowding (12 mm) and mandibular crowding (13 mm), with 3 mm of overjet and 2.5 mm of overbite. Occlusal caries was observed concerning the maxillary and mandibular permanent first molars (16, 26, 36, 37, 46, 47) (Figures 1 and 2).
A 17-year-old Female Patient with End on Molar Relationship Before Treatment.
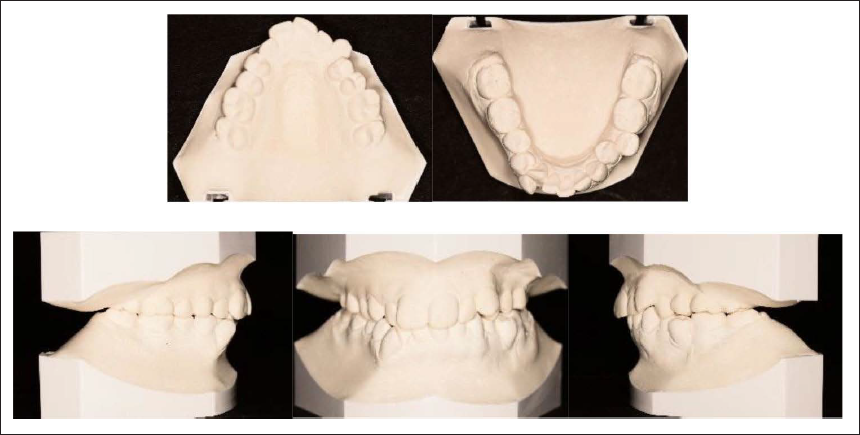
Pre-treatment Models.
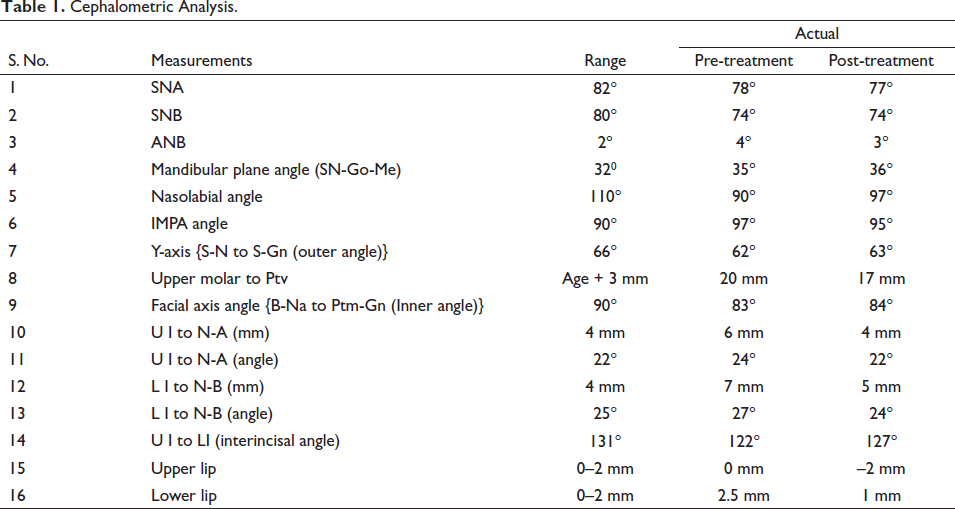
Radiographic examination revealed the presence of all four third molars. Lateral cephalometric evaluation confirmed a skeletal Class II jaw–base relationship (ANB, 4°), with hyperdivergent growth pattern (SN-Go-Me, 35°), and proclined mandibular incisors (IMPA, 97°), with decreased interincisal angle (122°) (Figure 1; Table 1).
Cephalometric Analysis.
Treatment Objectives
The treatment objectives are listed as follows:
To achieve well-aligned maxillary and mandibular arches. To establish a Class I molar relationship and canine relationship bilaterally. To establish ideal overjet and overbite. To correct the dental midline discrepancy. To obtain a harmonious soft-tissue profile.
Treatment Plan
The treatment plan considered was the extraction of upper left first premolar and the mandibular first premolars to resolve anterior crowding, with upper right first premolar substitution in the place of the missing canine, finishing in a Class I molar relationship bilaterally.
With the patient’s agreement, we decided to proceed with this treatment plan. Also, we observed that the color, shape, and size of the upper right first premolar was favorable for substitution in place of the missing canine.
Treatment Progress
Treatment was initiated with the extraction of all first premolars except maxillary right first premolar, which was planned for substitution as canine. After two weeks, banding and bonding were done in the upper arch with a pre adjusted edgewise appliance (0.22" × 0.028" slot MBT prescription, 3M Unitek). All bracket positioning was done according to the MBT prescription, except for the upper right first premolar bracket. The position of the bracket for the upper right first premolar was kept distally for mesio-palatal rotation, which will help in reducing the visibility of the palatal cusp while smiling. Leveling and alignment was initiated, with 0.014" Nickel Titanium archwire (3M Unitek nitinol super elastic, USA), progressing to 0.016" × 0.022" Nickel Titanium archwire (3M Unitek nitinol super elastic, USA).
Six months later, the lower arch was bonded, except for the lingually placed right lateral incisor. Leveling and alignment was then initiated with 0.012" Nickel Titanium (3M Unitek nitinol super elastic, USA), and continued with 0.016" × 0.022" Nickel Titanium archwire (3M Unitek nitinol super elastic, USA). After four months, an open coil spring was inserted on 0.016" × 0.022" Stainless Steel arch wire (SS American Orthodontics), between the lower right central incisor and canine, for creating space for the blocked out right lateral incisor. Three months later, the right lateral incisor was bonded, and leveling and alignment were then continued with 0.014" Nickel Titanium archwire (3M Unitek nitinol super elastic, USA), and progressed to 0.016 × 0.022" Nickel Titanium archwire (3M Unitek nitinol super elastic, USA).
Three months later, as leveling and alignment were achieved in both the arches, majority of the extraction space in the mandibular arch had been utilized in resolving the anterior crowding. Considering the situation, the original treatment plan had to be modified, and maxillary arch distalization was planned to achieve a Class I molar relationship bilaterally.
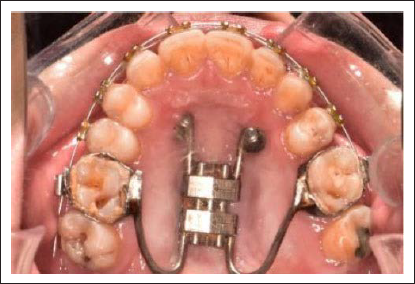
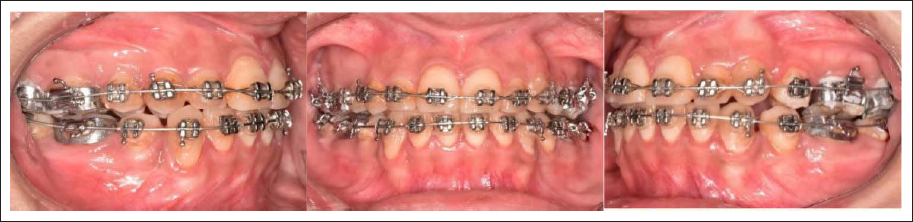
A Modified hybrid hyrax appliance (Leone, Italy) was used for the en-masse distalization of the upper dentition. The placement of the hyrax expander was modified. It was placed at the mid palatine rugae, with the expansion vector set anteroposterior instead of transverse, as this positioning will aid in distalizing the maxillary molar. The anteriorly directed arms of the hybrid hyrax were bent into an eyelet form for the insertion of two mini-implants in the anterior part of the palate, while the posterior arms were soldered to the first permanent maxillary molar bands (16, 26). After placement of the appliance, two mini-implants (SK Surgicals, India) (2 mm diameter and 10 mm length) were inserted 3 mm away from the mid-palatal suture at the level of the third palatal rugae under local anesthesia. Before active distalization started, the upper third molars were extracted (Figure 3).
A Modified Hybrid Hyrax Appliance Placed for Distalization.
The patient was instructed to activate the distalization screws weekly (0.2 mm per week), and this was continued for four months. During the monthly check-ups, the stability of the appliance, the mini-screws, and the patient’s dental hygiene were assessed. After four months, a Class I molar relationship was obtained bilaterally (Figure 4). The modified hybrid hyrax appliance was left in place for retention, with no further activation. Additional negative crown torque was added on 0.019 × 0.025" Stainless Steel archwire (SS American Orthodontics), lateral to the upper right first premolar, to simulate the inclination of a canine. Settling of the upper and lower arches was done on 0.014” Nickel Titanium archwire (3M Unitek nitinol super elastic, USA) for two months. The modified hybrid hyrax appliance was also removed. Debonding was done, and a fixed lingual retainer was bonded on the upper arch (3-4) and the lower arch (4-4). Also, the patient was provided Essix retainer for nighttime wear.
Distalization of the Upper Arch with Modified Hybrid Hyrax.
Treatment Result
A good occlusion with coincident midline and good intercuspation was achieved after 24 months of treatment. Replacement of the missing upper right canine with first premolar resulted in an esthetic smile. Class I molar relationship and canine relationship was established bilaterally. The cephalometric superimposition demonstrated the distalization of the maxillary permanent first molar (Figures 5 and 6; Table 1).
Intra-oral and Extra-oral Photos of a Patient After 24 Months of Treatment; Post-treatment Radiographs Superimposition of Pre- and Post-treatment Cephalometric Tracings.
Post-treatment Models.

Although the patient had a skeletal Class II base with retrusive maxilla and mandible, she exhibited a good soft tissue compensation. Additionally, advancement genioplasty would have further improved her facial esthetics. However, the patient decided not to undergo it, as she was already satisfied with her treatment results.
Discussion
Class II malocclusion is a commonly seen malocclusion in orthodontic practice, and a variety of treatment modalities have been noted in the literature. The original treatment plan considered in our case was the extraction of first three premolars to achieve Class I molar relationship bilaterally, with the missing upper right canine substituted by the first premolar. However, during the course of treatment, the plan had to be modified, as majority of the extraction space in the mandibular arch had been utilized in relieving the anterior crowding present, before a Class I molar relationship could be achieved. Although the patient had a skeletal Class II base with retrusive maxilla and mandible, she exhibited a good soft tissue balance, and distalization could be considered as an option for treatment. During distalization, the presence of third molars may impede the distal movement of the first and second molars, so it has been recommended to extract them when possible. 11 Hence, distalization of the upper arch, with the third molars extracted, was planned.
Distalization of the maxillary molars is a commonly used treatment method in dental Class II patients, with a significant amount of overjet, crowding in the anterior, or both. As headgears are not usually preferred by patients,12, 13 intraoral appliances, with a minimal need for patient cooperation, are often the appliance of choice. Unfortunately, majority of the conventional non-compliance devices produce undesirable side effects. Since these conventional appliances are connected to first or second premolars during distalization, the presence of counteracting moments is frequently inevitable leading to forward movement of premolars and anterior teeth and finally increased overjet.
In recent years, temporary anchorage devices have been combined with distalization appliances to prevent anchorage loss.3, 14 It has been reported that the range of molar distalization possible with use of skeletal anchorage is 1.4–5 mm for maxillary molars, and 1.6–7 mm in mandibular molars.15–18 Various insertion sites for temporary anchorage devices for distalization mechanics have been recommended. The anterior palate is considered as a safe site because of the good bone quality present, thin attached mucosa, and less risk of dental injury from close proximity of roots. 19 A study by Yu et al. reported that distalization with the mini-implants in the anterior palatal region provided bodily molar movement without tipping or extrusion as compared to mini-implants on the buccal side. 20 Also, a very high success rate of 98% has been reported with mini-implant placement in the anterior palate region. 21 Hence, in this case, a modified hybrid hyrax, with anchorage from two mini-implants in the anterior palate, was used successfully for the distalization of the maxillary molars.
Conventionally, the hyrax appliance is used for transverse maxillary expansion. Wilmes et al. introduced the hybrid hyrax distalizer, with mini-implants placed in the anterior palate that can be utilized for both orthopedic protraction of the maxilla with simultaneous distalization of the maxillary molars. 10 Here, we chose to modify the placement of the conventional hyrax appliance by setting the expansion vector anteroposteriorly, instead of transverse, with the anteriorly directed arms bent into an eyelet form for inserting two mini-implants in the anterior palatal region and the posterior arms soldered to the first permanent maxillary molar bands, hence named the modified hybrid hyrax appliance. This pattern of placement facilitates maxillary molar distalization. The activation schedule followed was quarter turn per week (0.2 mm/week). In this case, a successful distalization of 3 mm was achieved with bodily movement of molars, as the application of force was from the appliance placed high in the palatal vault, near to the center of resistance of the molars. The patient did not express any major pain or discomfort during hyrax activation. One main advantage of this appliance is that, after active distalization, the appliance can be converted to a passive anchorage device, eliminating the need for any additional retention method till the treatment is completed. Other advantages are cost-efficiency with minimal surgical invasiveness, no need for extra laboratory procedures, and easy fabrication.
Canines are considered extremely important in establishing a functional occlusion by guiding lateral occlusion of the mandible. Also, the prominence of the canine acts as a support for the upper lip, while their high gingival contour helps determine the smile line. Furthermore, canines have a unique shape and color, which makes them challenging to replace with premolars. Special consideration must be given to orthodontic mechanics when replacing upper canines with first premolars. 22 In this case, the color, shape, and size of the right first premolar was favorable for substitution in place of the missing canine. The position of the bracket for the upper right first premolar was kept distally for mesio-palatal rotation, which will help in reducing the visibility of the palatal cusp while smiling. The labial root torque was accentuated for the upper right first premolar to simulate canine prominence. The palatal cusp of the substituted premolar was abraded to avoid interference during disocclusion. Lateral disclusion was established in group function. The gingival margins of the upper canines showed a slight discrepancy, which could have been rectified with periodontal surgery; however, the patient refused, as she was already satisfied with the treatment results. All our treatment objectives were achieved with no compromise to the patient’s functional and occlusal stability (Figure 7).
One-year Post-retention Phototographs.

Conclusion
This new concept of modified placement of the hybrid hyrax appliance, introduced in this case report, could be used effectively in the treatment of Class II malocclusion for en-masse, bodily distalization of the upper dentition, with no anchor loss. Additionally, the same appliance could be used for retention after the active distalization period till treatment completion.
This approach can effectively shorten the length of treatment time and increase the orthodontist’s ability to gain space and provide anchorage.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and /or publication of this article.
Ethical Approval
No Institutional Ethical Committee approval was needed for this case study.
Informed Consent
Informed consent was obtained from the patient and guardian.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.