
Abstract
Anchorage is one of the most important consideration in the field of orthodontics to achieve a desired tooth movement. In order to eliminate the undesirable side effects such as anchorage loss, skeletal anchorage systems such as mini-implants have been introduced in orthodontics.
Aim:
To evaluate the bone thickness of the infrazygomatic crest in different cervical vertebrae maturation index (CVMI) and to compare it between male and female subjects, by using cone beam computerized tomography (CBCT) imaging.
Materials and Methods:
A retrospective study was conducted using CBCT images of 60 patients in the age group of 8–25 years. Cervical vertebra maturation was analyzed using Hassel–Farmann index and divided into 6 groups (n = 10/group). The infrazygomatic crest was divided into horizontal and vertical planes. The horizontal plane passed through the most inferior border of the zygomatic process of maxilla and the vertical plane passed through the most anterior point of the infratemporal fossa parallel to midsagittal plane. Five parallel lines were drawn at 2 mm interval in both horizontal and vertical planes (HB+2, HB+4, HB+6, HB+8, and HB+10) (V-2, V-4, V-6, V-8, and V-10). The bone thickness was measured at the point of intersection of these lines.
Results:
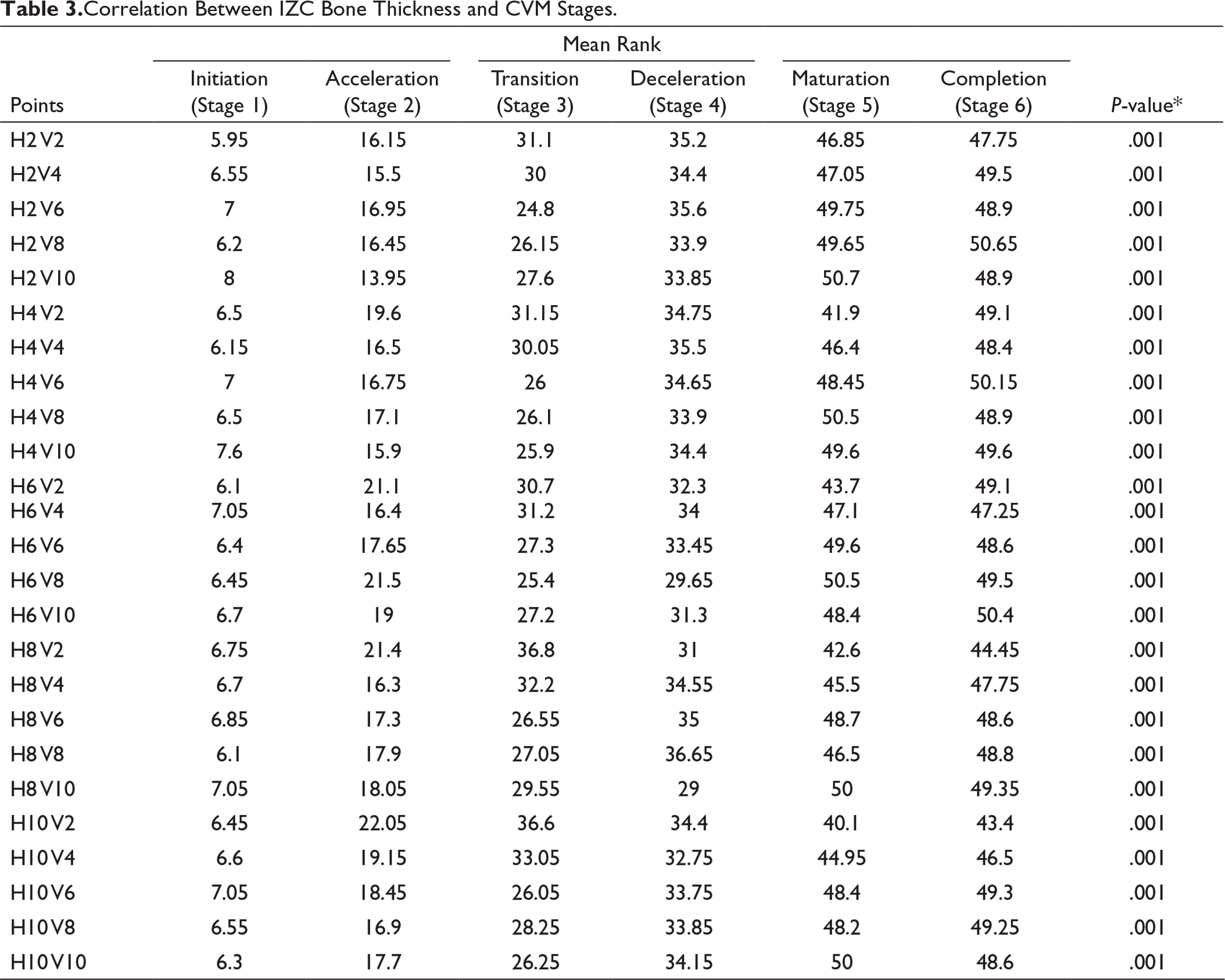
According to Kruskal–Wallis analysis, statistically significant difference in infrazygomatic crest (IZC) bone thickness was seen in various CVMI stages (P = .001). Maximum bone thickness was 11 mm and minimum bone thickness was 1 mm. No significant difference was observed between male and female populations.
Conclusion:
Thus, the superolateral area in infrazygomatic crest is the most appropriate site for miniscrew insertion in all age groups.
Introduction
Anchorage in orthodontics has been an important consideration since the start of the millennium. Conventional anchorage uses intraoral and extra oral methods like headgear and intermaxillary elastics to reinforce anchorage. Nowadays, cortical anchorage has replaced conventional techniques since it provides increased anchorage control with least patient compliance. Temporary anchorage devices such as miniscrews, mini-implants, miniplates are used extensively because of the smaller size, cost effectiveness, and ease of application.1, 2 Many factors such as implant design, torque, patient age, bone thickness, adequate mechanical properties of the screws, material used, and type and length of active loading3-6 have determined the primary stability of the miniscrews. Safe zones for placement of miniscrews are being extensively studied7-10 in order to prevent the risk of injuring the roots of the teeth and to decrease mucosal irritation. Many methods such as use of insertion guides and11, 12 assessment of bone thickness with computed tomography (CT) and cone beam computerized tomography (CBCT) are followed to decrease the risk factors associated with miniscrews. Mavropoulos et al 13 has stated that >1 mm of cortical bone thickness is required for the stability of the implants. However, a higher failure rate due to peri implantitis, decreased stability when loaded, and increased risk of root injury have decreased the application of interradicular implants in severe malocclusions. 14
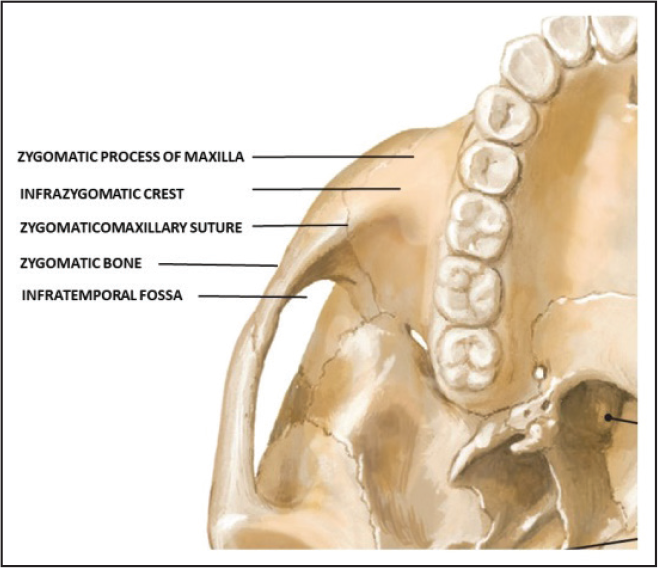
Extraalveolar sites such as infrazygomatic crest and buccal shelf area can be used to overcome these disadvantages. Infrazygomatic crest is a bony ridge between the zygomatic process and the alveolar process of maxilla (Figure 1). It has bicortical plates which provide precise control of anchorage for effective tooth movement such as space closure in class II patients, 15 molar intrusion in anterior open bite cases, 16 uprighting the impacted molars, deep bite correction, 17 molar distalization,18, 19 and maxillary protraction in skeletal class III cases. 20
Anatomy of Infrazygomatic Crest.
Temporary anchorage device (TAD) placed in infrazygomatic crest region has an overall success rate of 93.7%, of which only 6.3% of stainless steel and 5.7% of titanium alloy implants failed 21 . Mini-implants placed in infrazygomatic crest do not interfere with the orthodontic tooth movement as they are placed at a higher position from the root region. However due to the close proximity with the maxillary sinus 22 and the mesiobuccal root of the maxillary first molar in young patients, accurate determination of bone thickness is necessary for selection of ideal implants. Many studies have been conducted to evaluate the intraradicular bone thickness.23, 24 However only a few studies have been conducted to evaluate the infrazygomatic bone thickness. Fransworth 3 stated that average infrazygomatic bone thickness is only 1.44 to 1.58 mm. Many studies were conducted using computed tomography (CT), but the main disadvantage of CT is its high cost and higher radiation exposure. The aim of the study was to measure the bone thickness of infrazygomatic crest region and to correlate the bone thickness with cervical vertebrae maturation index (CVMI) using cone beam computed tomography (CBCT).
Materials and Methods
A retrospective study with CBCT scans of 60 patients (30 male, 30 female) was conducted. In order to evaluate the sample power, G*Power software (3.0.10) was used and a power of 80% was found based on a large effect size. The identity of the patients was not revealed, and each patient images was given a unique identity code. CBCT equipment used in this study was Kodak 9500. The settings were as follows: 90 kVp, 10 mA, exposure time 15 s, field of view 18 × 21 cm with a spatial resolution of 10 line pairs per centimeter, and an isotropic of 0.2 mm voxel size was used. The institutional review board reviewed and approved the study. The age of the patients ranged from 8 years to 25 years.
Inclusion criteria include presence of permanent first molar with no bony lesion. Exclusion criteria include presence of any tumors, atrophic bone, cleft lip and palate, syndromes associated with bone metabolism, impacted teeth in the infrazygomatic region, and partially edentulous patients.
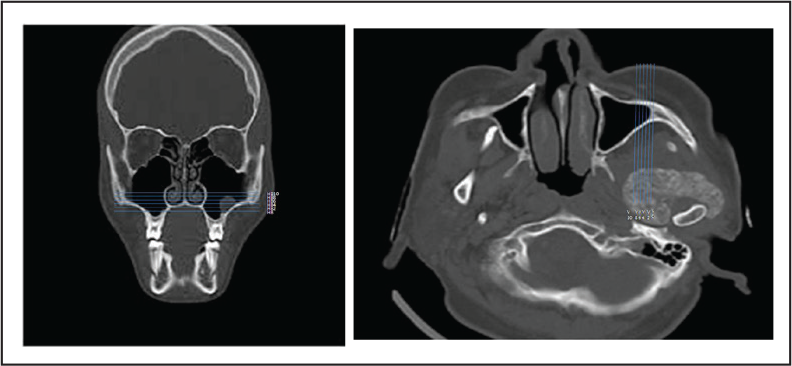
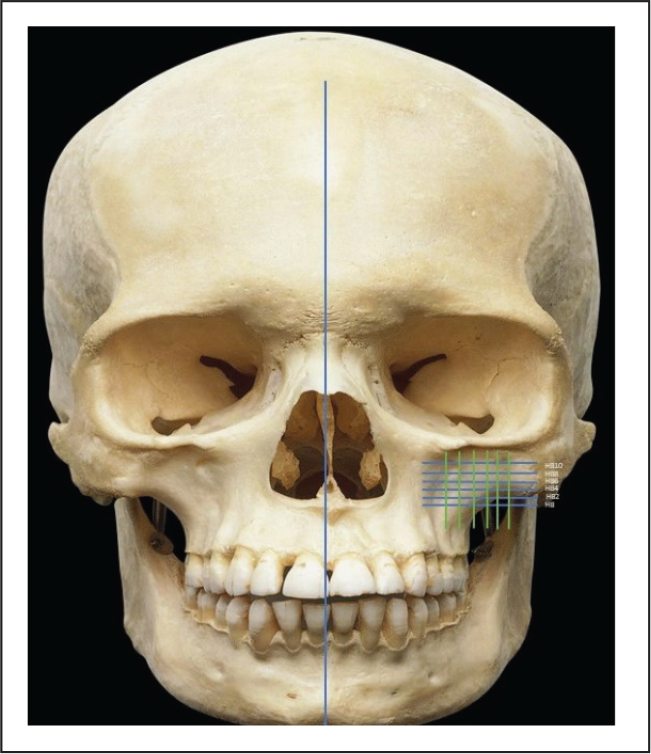
The infrazygomatic crest was divided into horizontal and vertical planes. The horizontal plane passed through the most inferior border of the zygomatic process of maxilla and the vertical plane passed through the most anterior point of the infratemporal fossa parallel to midsagittal plane (Figure 2A and B). Five parallel lines were drawn at 2 mm interval in both horizontal and vertical planes (HB+2, HB+4, HB+6, HB+8, and HB+10) (V-2, V-4, V-6, V-8, and V-10). The bone thickness was measured at the point of intersection of these lines (Figure 3).
Construction of Horizontal Reference Plane (HB) and Anteroposterior Plane (V). (A) HB Plane Passes Through the Most Inferior Border of the Zygomatic Process of Maxilla. (B) V Plane Passes Through the Anterior Most Point of the Infratemporal Fossa.
Construction of Reference Planes in Skull.
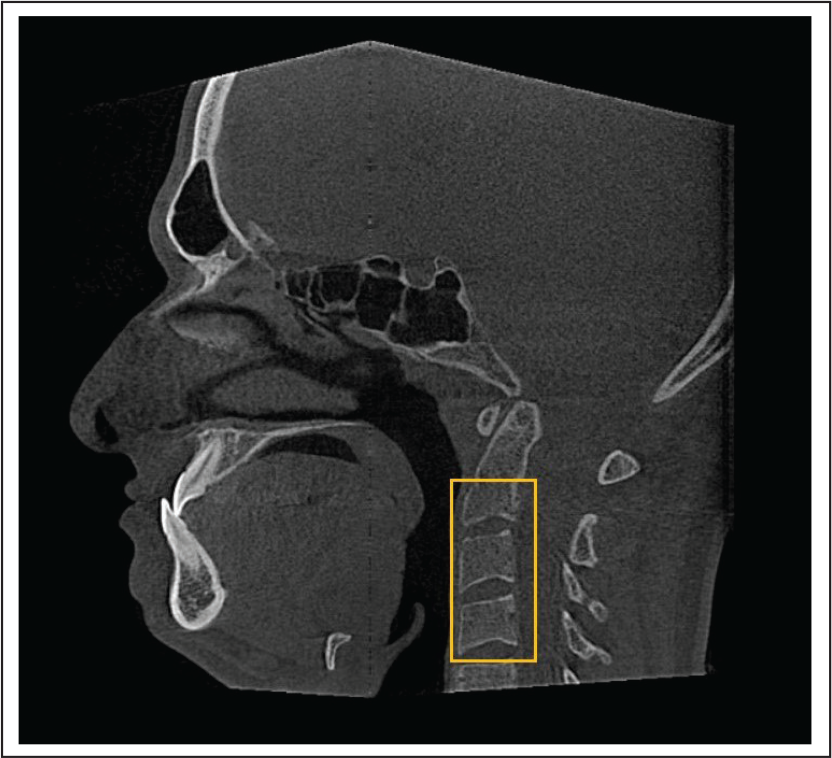
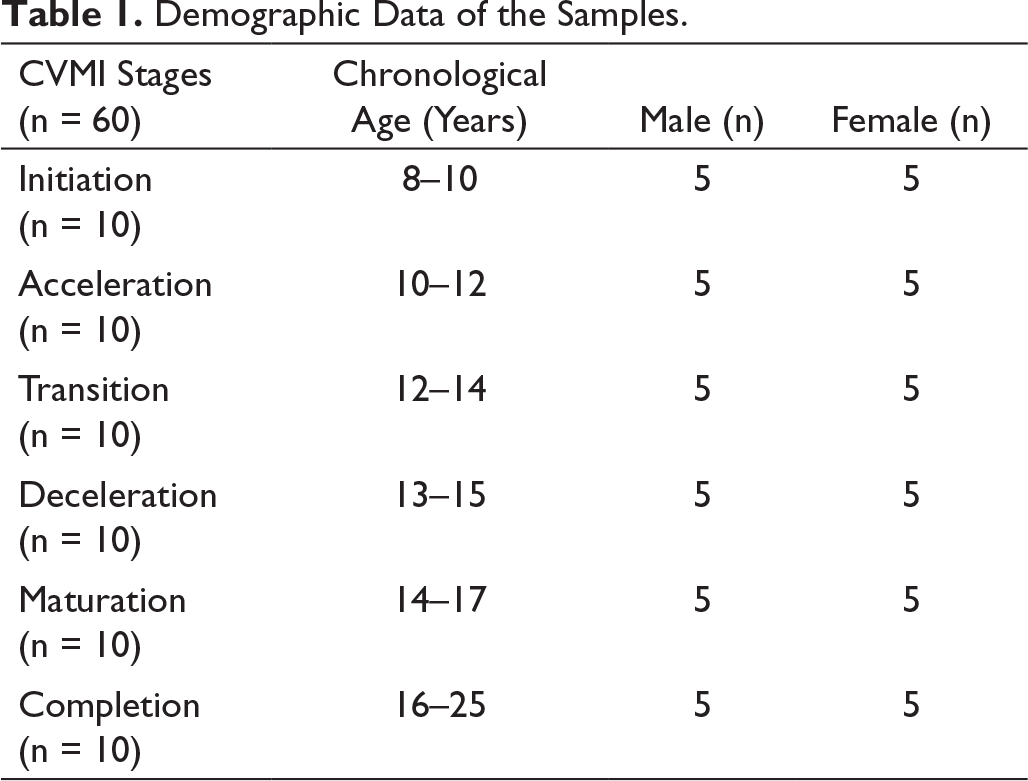
Cervical vertebra maturation was constructed in CBCT and was analyzed using Hassel–Farmann index (Figure 4; Table 1). All the measurements were performed by a single investigator.
Assessment of CVM in CBCT.
Demographic Data of the Samples.
Statistical Analysis
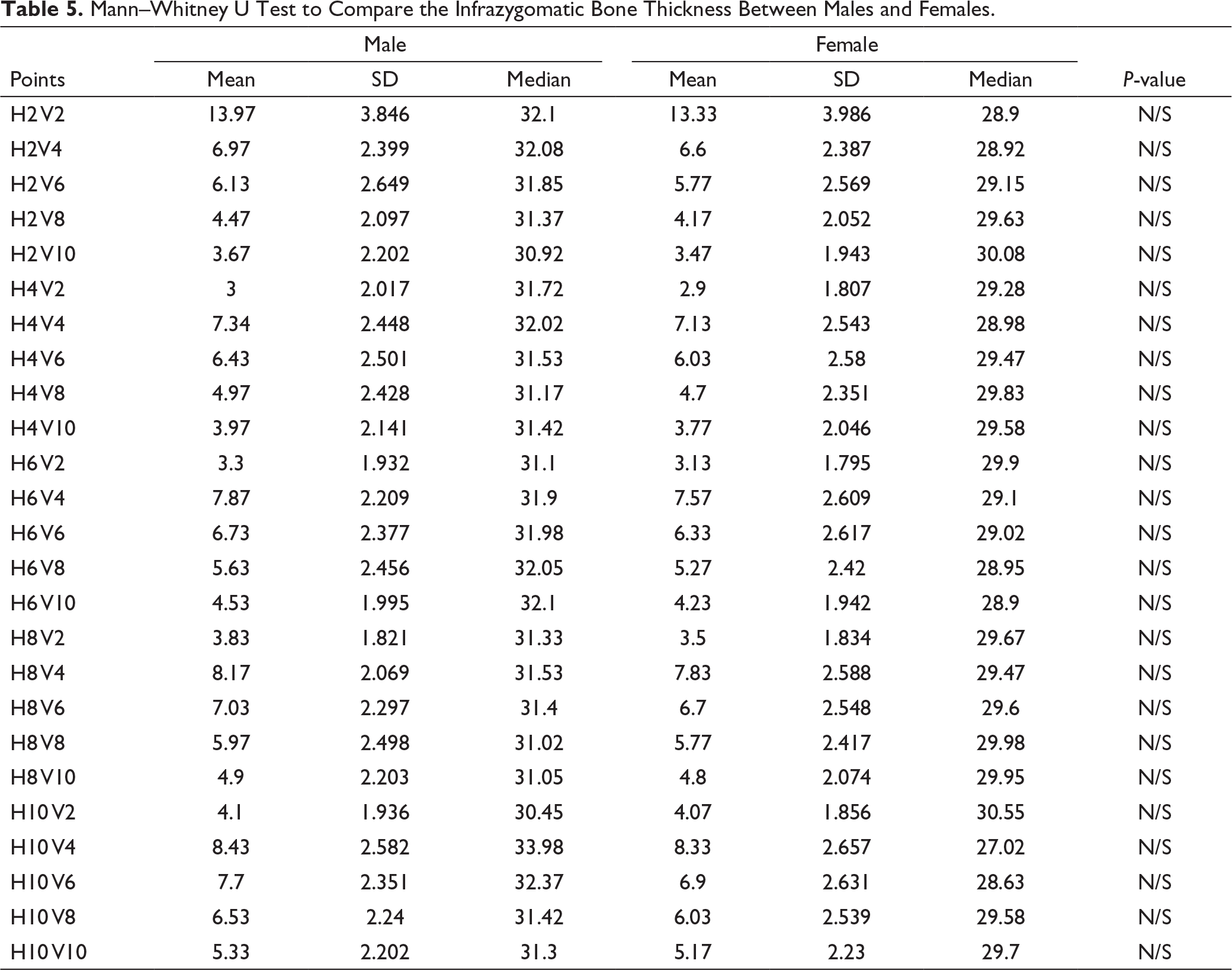
The Kruskal–Wallis analysis of variance (ANOVA) test was used to analyze the correlation between the infrazygomatic bone thickness and the cervical vertebrae maturation stages. Mann–Whitney U test was used to compare the infrazygomatic bone thickness between males and females.
Results
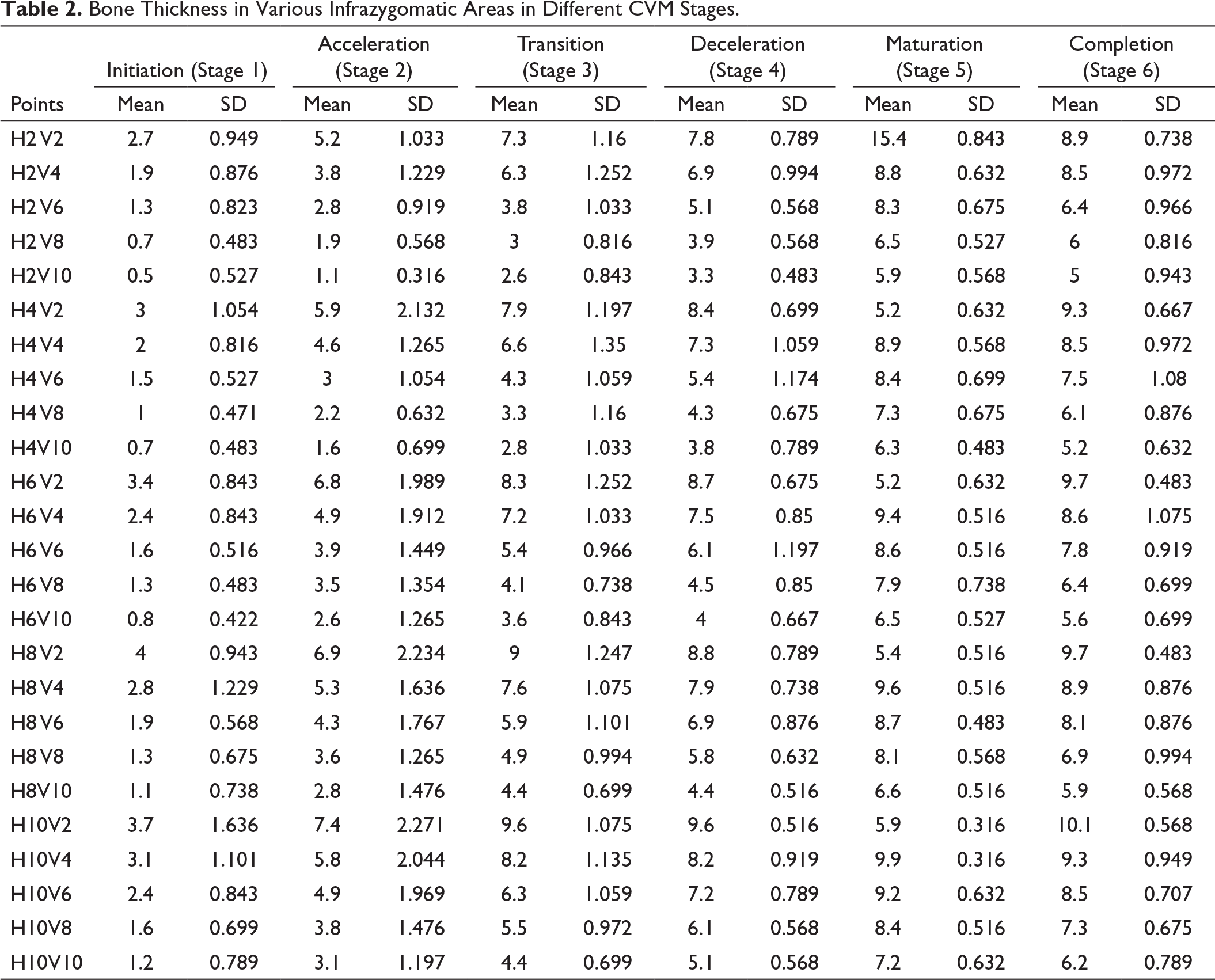
Bone Thickness in Various Infrazygomatic Areas in Different CVM Stages.
Correlation Between IZC Bone Thickness and CVM Stages.
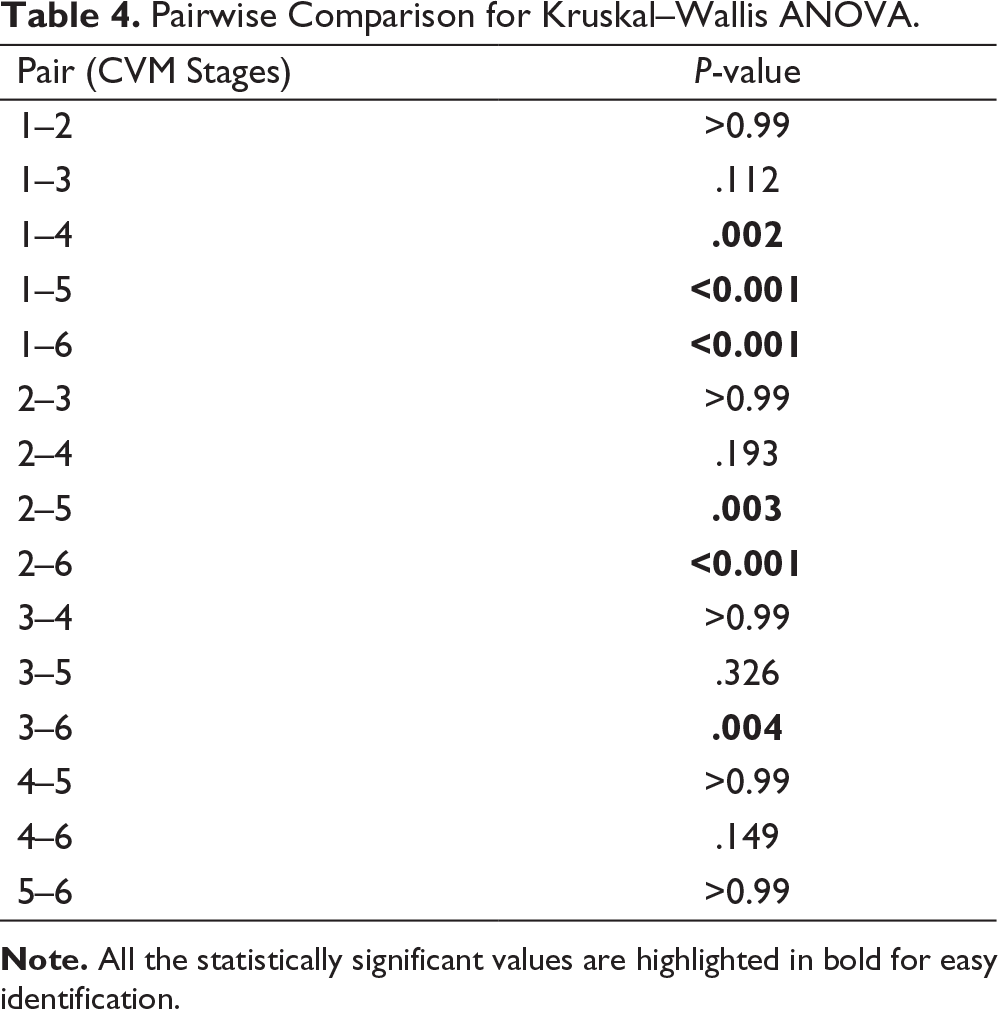
Pairwise Comparison for Kruskal–Wallis ANOVA.
Mann–Whitney U Test to Compare the Infrazygomatic Bone Thickness Between Males and Females.
Discussion
Cone beam computed tomography allows precise 3D imaging with less radiation exposure providing a more detailed evaluation of the patient compared to CT. 25 According to Lee et al, the anterior most point of the infratemporal fossa which is close to the zygomaticomaxillary suture can be easily identified in CT images. Thus, the study was conducted using infratemporal fossa as the horizontal reference line. 26 In our study, the thickest amount of bone was observed in superolateral region of infrazygomatic bone which corresponds to the zygomatic process of maxilla with the maximum mean bone thickness of 10 mm, and the least bone thickness was observed in the anterior wall of maxillary sinus with the maximum mean bone thickness of 5 mm in the completion stage of CVMI. Statistically significant difference in bone thickness was observed between initiation and maturation, completion stages and also in acceleration and completion stages. This can be attributed to the increase in bone density with increasing age and also to the development of the maxillary sinus into reverse pyramidal shape causing expansion laterally at the superior region.27, 28 The infrazygomatic bone thickness showed a marked variation of about 0.5 mm in the initiation stage to 10 mm in the completion stage. Studies conducted by Ko et al 29 and Alrbata et al 30 suggest that infrazygomatic bone thickness of 1 to 2 mm will be adequate for placement of 4- to 5-mm miniscrews for a 2-mm miniplate. However, if a 5- to 7mm-long miniscrew is used in the initial stages of bone development, it might lead to perforation of Schneiderian membrane of the maxillary sinus. Thus, proper assessment of bone thickness becomes necessary for selection of ideal miniscrews for orthodontic purpose.
The bone thickness was highest at v2 and v4 regions in all horizontal areas than at medial points with the range of about 2.7 mm to 10.1 mm. This correlated with the study of Lee et al, 26 in which the bone thickness increased laterally than the medial regions, with the thickness of bone ranging from 1.8 mm to 5 mm. He also stated that the miniscrews of about 4 to 7 mm can be used in these areas if miniplates are used, while longer implants would be appropriate if the implants are placed in the oblique direction. The bone thickness also increased in caudocranial direction in our study, which was similar to the results of Prager et al 31 where the thinnest bone was observed at 2.7 mm in the apical region while near the zygomatic bone, it was 9.8mm. Miniscrews placed at the level of zygomatic process have the advantage of less mobile mucosa as well as decreased interference with the tooth movement. He concluded that miniscrews of 5 mm in length can be placed near the alveolar process while 7-mm miniscrews can be placed closer to zygomatic process. Baumgaertel and Hans 32 also showed similar results where the greatest bone depth was observed at 11.48 mm apical to cemento enamel junction (CEJ) of the maxillary molar. Liou et al 33 has stated that the mean bone thickness was 5.2 mm with 40 degree insertion angle and 8.8 mm at 75 degree insertion angle. Murugesan et al 34 and Amri et al 35 also showed similar results and recommended use of 9 to 11 mm implants at an angle of 65 to 70 degree at a height of 12 to 17 mm above the occlusal plane.
Our study also showed no statistical difference between the male and female groups which was in concordance with the previous studies of Prager et al and Santos et al who showed no significant gender difference. 36 However, in the study conducted by Chen et al, the average infrazygomatic (IZ) bone thickness was 5.8 mm, with the male group showing bone thickness of more than 6 mm. These differences might be due to the individual variation in the development of maxillary sinus. 37
The study included the patients of age 8 to 25 years. Determination of appropriate age for miniplate insertion is based on the orthodontic treatment plan. Jager et al have stated that maximum skeletal effects can be achieved if the treatment is started before 8 years of age. 38 Bacetti has also succeeded in placing mini-implants in 9-year-olds for correction of skeletal class III problem. Miniplates are contra indicated below 8 years because the presence of the low bone density in children will result in increased failure rate for miniplate anchorage, 17 whereas in older patients, because of the increased bone volume in zygomatic process, adequate anchorage can be achieved even by using single cortical anchorage systems for distalization, molar intrusion, etc. Hence, assessing the skeletal age of the patient is necessary to determine the bone volume and density before placing the miniscrews for orthodontic purpose.
Even though Vargas et al 39 have stated that there is no correlation between the facial pattern and infrazygomatic crest (IZC) bone thickness, Murugesan et al 40 have stated that bone thickness decreased in high angle cases compared to low angle cases. Thus, further longitudinal studies are required to investigate the infrazygomatic bone thickness in various skeletal patterns.
Conclusion
The study results can be summarized as follows: the superior and the lateral regions of the zygomatic process of maxilla have the maximum bone thickness and are the most appropriate site for placement of miniscrews or miniplates. There was no statistically significant difference between the male and female groups. Bone thickness increased with cervical vertebrae maturation age. Thus, the findings of the study can be used as a benchmark for the selection of ideal implants by clinicians.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.