
Abstract
Aim and Objective:
The aim of the study was to compare the full-depth bone thickness and the cortical bone thickness in the infrazygomatic crest (IZC) region above the mesiobuccal (MB) root of maxillary first molar and second molar and thus find the ideal site for the placement of IZC screw.
Materials and Methods:
Pretreatment cone-beam computed tomography images of 30 orthodontic patients were collected and IZC bone thickness and cortical bone thickness were measured above the MB root of maxillary first and second molar at an angle of 70° to the molar occlusal plane. Measurements were done on both right and left sides. Independent sample t test was done to compare the bone thickness between the right and left sides and also to compare the bone thickness above the first and the second molar.
Results:
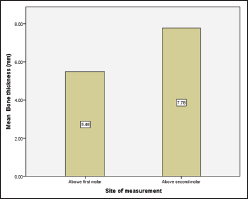
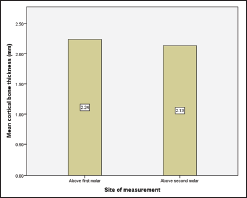
Mean bone thickness at the IZC region of 5.48 ± 2.2 mm and 7.78 ± 2.35 mm and a cortical bone thickness of 2.24 ± 0.46 mm and 2.13 ± 0.46 mm was obtained above the MB root of maxillary first molar and second molar, respectively. IZC bone thickness was significantly higher above the second molar than above the first molar (P < .001), whereas there was no significant difference in the cortical bone thickness measured on both the sites (P = .22).
Conclusion:
Significantly higher IZC bone thickness was noted above the MB root of the maxillary second molar, which may ensure better stability and safety of the miniscrew.
Introduction
Anchorage control is one of the inevitable considerations during orthodontic treatment. Temporary anchorage devices (TADs) are now tremendously being used to deliver absolute anchorage during tooth movements. Miniplates, interradicular implants, and extraradicular screws are the different types of TADs used for clinical application. Out of these, interradicular and extraradicular implants are the most commonly used ones. Interradicular implants are positioned interdentally, whereas, extraradicular implants are placed at sites away from the tooth roots. Minute size, simple insertion technique, various insertion sites, immediate loading, and minimal patient cooperation are the advantages of the mini-implants that have led to their popularity.1, 2
Infrazygomatic crest (IZC) is a hard tissue elevation in the middle of the maxillary zygomatic process and the alveolar process.3, 4 This is one of the most common extraradicular sites in the maxilla for miniscrew placement. Here, the bone screws will be placed buccal to the molars at the level of the mucogingival junction or alveolar mucosa. Unlike interradicular mini-implants, IZC screws ensure unhindered movement of the teeth. IZC screws are effective in providing anchorage for anterior intrusion and retraction, molar intrusion, and en-masse distalization of maxillary teeth.3–9
The location of the IZC varies with age. In young individuals, it is located between the upper second bicuspid and first molar, whereas in adults, it extends superior to the first molar. 3 The use of mini-implants and miniscrews are more frequent in adults than in young patients because of the fear of injury to the developing roots and tooth buds in the latter.
Clinically, the ideal site for IZC screw placement in adults is controversial. Liou et al recommend that IZC screws be placed above the mesiobuccal (MB) root of the maxillary first molar, while Lin et al recommend it to be positioned above the MB root second (M2) molar.3, 10, 11 Therefore, the aim of the study was to assess and compare the full bone thickness and cortical bone thickness in the IZC region above the MB root of M1 and M2 in South Indian subjects and thus identify the ideal location for the placement of IZC screw.
Materials and Methods
The study was carried out at the Department of Orthodontics, Saveetha Dental College and Hospitals, Chennai. This was a retrospective study done using cone beam computed tomography (CBCT) images. The study design was analyzed and accepted by the Scientific Review Board of the institution.
The sample size was calculated for a power of 95% using G power analysis based on the results obtained by Liou et al.
3
30 CBCTs, which were previously taken to diagnose impacted teeth, were selected from the database of the orthodontic patients who met the following selection criteria:
South Indian nativity. Adults subjects in the age group 18 to 25 years. Patients with no gross facial asymmetries and craniofacial anomalies. Patients with no posterior dental arch constriction and other dental anomalies that can hinder the measurements. Systemically healthy patients.
Measurements
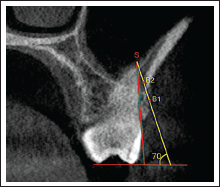
Galileos Viewer Software (Sirona, Vensheim, Germany) was used to measure the IZC bone thickness on a CBCT. The image was aligned such that the MB root tip of the M1/M2 molar was seen in all the views and the bony dimensions were evaluated cross-sectionally. The first step was to draw 2 reference lines. The first line connected the buccal and palatal cusp tip of the molar representing the occlusal plane (OP). The second line was a tangent to the buccal surface of the root of the molar that varied depending on the angulation of the teeth (Figure 1). The point where the tangent intersected the sinus floor was the S point. Next, a third line was drawn such that it formed a 70° angle with the OP line and it extended through the point S. The place where the third line intersected the outer surface of the buccal cortical plate was B1 and the place where it intersected the inner surface of the buccal cortical plate was B2 (Figure 2). The line between S and B1 represented the full-depth IZC bone thickness, whereas the line between B1 and B2 represented the cortical bone thickness. Measurements were performed bilaterally. All radiographic evaluations were performed by a single examiner. Intraexaminer reliability was examined by performing all the measurements again after a period of 14 days for 5 CBCTs. Intraclass correlation coefficient value of 0.9 to 1 was obtained for all the measurements indicating excellent reliability.
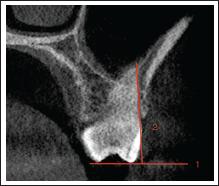
Cross-Sectional View of a CBCT Image Representing the Third Line (Yellow), S, B1, and B2 Points.
Statistical Analysis
Independent sample t test was done for comparing bone thickness measurements between first and second molars. The data were decided to be combined if no statistical difference existed between both sides. The same statistical test was used to differentiate the thickness above the MB root of M1 and M2 molars. The significance value was set as 0.05 for all analyses.
Results
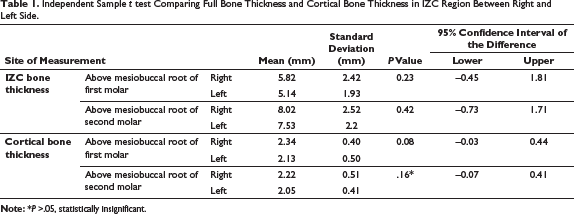
Independent Sample t test Comparing Full Bone Thickness and Cortical Bone Thickness in IZC Region Between Right and Left Side.
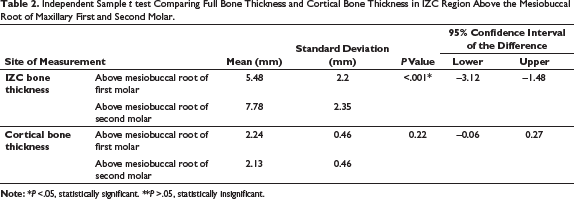
Independent Sample t test Comparing Full Bone Thickness and Cortical Bone Thickness in IZC Region Above the Mesiobuccal Root of Maxillary First and Second Molar.
Graphical Representation of the Mean Bone Thickness in IZC Region Above the Mesiobuccal Root of Maxillary First and Second Molar.
A mean cortical bone thickness of 2.24 mm and 2.13 mm was observed above the M1 and M2 molars, respectively. Independent sample t test with a P value of 0.22 indicated that there was no significant variation in the cortical bone thickness between the 2 sites (Table 2). Figure 4 graphically represents the mean cortical bone thickness seen on the 2 sites.
Graphical Representation of the Mean IZC Cortical Bone Thickness Above the Mesiobuccal Root of Maxillary First and Second Molar.
Discussion
One of the major difficulties faced during the placement of IZC screws is deciding the ideal site for the placement of the miniscrew. There is always a debate on whether to insert the screw above M1 or M2. There are few studies in the literature reporting on the comparison of IZC thickness above M1 and M2. Therefore, the main objective of this retrospective evaluation was to assess the full-depth IZC thickness and cortical bone thickness of IZC above M1 and M2.
The study methodology for measuring IZC thickness was similar to that of Liou et al. 3 The thickness was computed along the angle of insertion of the miniscrew, ie, 70° to the OP of the molar because the thickness was found to be more in this insertion angle.3, 12 Liou et al compared bone thickness among various insertion angles and reported IZC thickness of 5 mm to 9 mm at an angle of 40° to 75° to the OP. This was measured above the MB root of M1. 3 In a previous study conducted among the Dravidian population, a bone thickness of 7 mm was observed above the distobuccal (DB) root of the M1 when measured at an insertion angle of 70° to the OP. 12 Santos et al reported an average of 2.4 mm of bone above the DB root of M1, respectively. 13 In this study, we observed 5.5 mm bone thickness above the MB root of M1 and 7.8 mm above the MB root of M2. The bone thickness increased as we moved posteriorly from M1 to M2. These findings were similar to the findings reported by Paul et al 14 and Murugesan et al, 15 whereas it was contradictory with the results obtained by Vargas et al. 16 Moreover, the bone thickness was the least in vertical growing patients, which needs to be taken into consideration during clinical placement of IZC screws.14–16
IZC screws are mostly available in 2 dimensions, ie, 2 × 12 mm and 2 × 14 mm. Nearly 7 mm of the total length will be occupied by the cutting edge that will lie within the bone. 11 In order to enhance the stability of the implant, the cutting edge should lie completely within the bone. Therefore, a minimum of 7 mm thick bone must be present for safe placement of the IZC screw without sinus penetration. According to the results of this study, the required amount of bone for the safe placement of IZC is present above the MB root of M2. Sinus penetration of more than 2 mm can cause perforation of the Schneiderian sinus membrane, disrupting healing and increasing the incidence of sinusitis. 17 Baumgaertel and Hans reported that an IZC screw of length 6 mm or more can penetrate the maxillary sinus. 18 Sinus penetration can also depend on other factors like anatomical variations in the sinus such as the reverse fold and prevalence of septa. 19
Another important factor deciding the primary stability of the screws is the cortical bone thickness. In this study, we observed cortical bone thickness of 2 mm at the IZC above the molars. Similarly, Farnsworth et al 20 and Chen et al 21 reported thicknesses of 1.58 mm and 2.6 mm in the IZC region, respectively. Chen et al 21 also stated that there was no major difference in the thickness of the upper posterior alveolar region when compared to the IZC. Considering the fact that the cortical bone thickness of greater than 1 mm is necessary for adequate primary stability and increased success rate of the miniscrews,22, 23 the South Indian population has an adequate cortical bone thickness that can provide good primary stability for the IZC screws.
Conclusion
The full-depth bone thickness in the IZC region was significantly high above the MB root of M2 compared to that of M1 in the South Indian subjects, whereas the cortical bone thickness was the same in both sites. Therefore, placing IZC screws above the MB root of M2 will ensure both safety and stability of the miniscrew.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval from Scientific Review Boards (IRBs) was obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.