
Abstract
Objective:
To assess the relationship of pharyngeal airway dimensions and the position of the hyoid bone in several craniofacial morphologies among Nepali adults. To assess the relationship between dimensions of the pharyngeal airway and position of the hyoid bone and compare gender dimorphism.
Materials and Methods:
The cross-sectional observational research comprised lateral cephalograms of 150 subjects aged 16 to 30 years. Samples were separated into three sagittal craniofacial morphological groups based on the ANB (A point, nasion, B point) angle and into gender groups. Different parameters (linear and angular) for measuring dimensions of the pharyngeal airway and position of the hyoid bone were assessed. An ANOVA test and a Pearson correlation test were performed.
Results:
Dimensions of the pharyngeal airway were largest in skeletal Class III when compared to skeletal Class I and Class II subjects, with a lower pharyngeal airway space and the length of the nasal fossa being significantly larger. The hyoid bone was anteriorly and inferiorly placed in Class III skeletal subjects. Males had greater pharyngeal airway dimensions and a hyoid bone positioned more inferiorly and anteriorly. The nasal fossa length had a strong positive correlation with the hyoid bone position vertically.
Conclusion:
There were differences in the dimensions of the pharyngeal airway and position of the hyoid bone in various craniofacial morphologies among Nepali adults. Gender dimorphism was observed in both dimensions of the pharyngeal airway and the position of the hyoid bone.
Introduction
The nasal airway physiology needs adequate anatomical dimensions for the airway. 1 Oral respiration related to nasal obstruction is a common finding among orthodontic patients. 2 Obstruction of nasopharyngeal respiration is often associated with various craniofacial features, such as upward and backward growth of condyle, downward and backward rotation of mandible, anterior open bite, divergent gonial angle, and spacing in the mandibular anterior region. 3 The elimination of respiratory obstruction and achievement of functional nasal breathing with accurate patterns of swallowing boost the stability and functional balance of orthodontic treatment. 4 Angle, Linder-Aronson, Harvold, Fränkel, and others have established that the obstruction of the airway can govern unbalanced development of facial form.5-8 The hyoid bone has an important role in tongue physiology, deviation of which might result in different malocclusions. 9 Positive correlation has been reported with the position of the hyoid bone and the pharyngeal airway space in a group of normally swallowing individuals. 10 Significant correlation is found among hyoid bone position and width of the pharyngeal space inferiorly with the change in ANB (A point, nasion, B point) angle. 11
The lateral cephalogram is considered an effective tool intended for assessing different measurements of the pharyngeal region, the position of the hyoid bone, and their relationship with various skeletal patterns.12, 13 Pharyngeal anatomy and dentofacial form are expected to have a mutual relation because of their close anatomical proximity, thus rationalizing orthodontic attention. The current research attempts to determine whether the size of the nasopharynx and hyoid bone position is associated with any particular type of skeletal configuration of the dentofacial complex. The present study also establishes the correlation among nasopharynx and position of the hyoid bone, opening up the gateway for further research.
Materials and Methods
The study is cross-sectional and observational, carried out at Kathmandu, Nepal, using secondary records. Ethical clearance was obtained from the Institutional Review Committee. The nonprobability convenient sampling technique was used. The sample size was calculated taking into consideration the average number of patients who came for orthodontic treatment at the hospital. A total of 150 lateral cephalograms were carefully chosen for the study. Cephalograms belonging to adults in the age group of 16 to 30 years were chosen, when the hyoid bone is ossified attains the adult position; also, the growth of the pharynx is stable after the age of 16 years.14, 15 The samples’ case history was checked for conformity with the inclusion criteria. Samples were excluded if they had a history of craniofacial trauma, craniofacial deformity, evidence of congenitally absent, extracted, or retained deciduous teeth, previous history of orthopedic/orthodontic treatment, evidence of nasal obstruction, presence of any pharyngeal pathology, enlarged tonsils or adenoids, or a poor-quality radiograph.
Landmarks used in this study were:
For classification of samples:
S: sella, N: nasion, A: subspinale, B: supramentale, ANB angle. 16
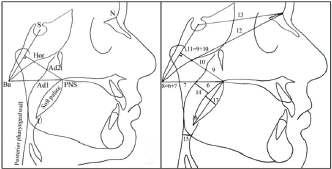
For assessment of the pharyngeal airway dimension (Figure 1):
(1) PNS; (2) Ad1: meeting of the line joining PNS to the basion (BA) with the pharyngeal wall posteriorly; (3) Ad2: meeting of the line joining PNS to Hor with the pharyngeal wall posteriorly; (4) Hormion (Hor): intersection of perpendicular from S-Ba to PNS with the sphenoid bone; (5) U: tip of the soft palate; (6) PNS-Ad1: lower aerial width; distance between closest adenoid tissue measured over the PNS-Ba line (Ad1) and PNS; (7) Ad1-Ba: lower adenoid width, thickness of soft tissue at nasopharynx posteriorly through PNS-Ba; (8) PNS-Ba: lower airway width, distance between Ba and PNS; (9) PNS-Ad2: upper aerial width, distance between PNS and closest adenoid tissue measured over a perpendicular line to S-Ba from PNS (Ad2); (10) Ad2-Hor: upper adenoid width, thickness of soft tissue at nasopharynx posteriorly through PNS-Hor; (11) PNS-Hor: upper airway width, distance between Hor and PNS; (12) N-Hor: length of nasal fossa, distance between Hor and N; (13) S-N: anterior cranial base; (14) McNamara’s upper pharyngeal airway space (UPAS): minimum distance between closest point on the pharyngeal wall posteriorly and upper half of soft palate 17 ; (15) McNamara’s lower pharyngeal airway space (LPAS): minimum distance between closest point on pharyngeal wall posteriorly and the point where posterior contour of tongue crosses mandible 17 ; (16) SPL: soft palate length; distance between PNS and U; and (q) SPT: maximum soft palate thickness.
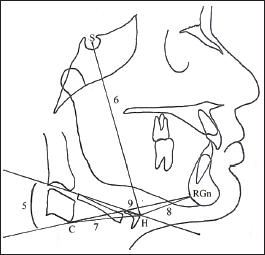
For assessment of the position of the hyoid bone (Figure 2):
C: most anterior, inferior point on cervical vertebrae number three; (2) RGn (retrognathion): midpoint between the most posterior and inferior point on the mandibular symphysis; (3) H (hyoidale): most anterior and superior point on the hyoid bone body; (4) hyoid plane: the plane along the long axis of greater horns (of hyoid bone) from H; (5) hyoid plane angle (HPA): superior posterior angle made by the intersection of the hyoid plane with C-RGn; (6) S-H: line joining sella and hyoidale; (7) C-H: line joining point C and hyoidale; (8) H-RGn: line joining the hyoidale and retrognathion; and (9) C-RGn: line joining point C and retrognathion.
Pharyngeal Airway Dimensions: 6. PNS-Ad1, 7. Ad1-Ba, 8. PNS-Ba, 9. PNS-Ad2, 10. Ad2-Hor, 11. PNS-Hor, 12. N-Hor, 13. S-N, 14. UPAS, 15. LPAS, 16. SPL, 17. SPT.
Hyoid Bone Position: 5. HPA, 6. S-H, 7. C-H, 8. H-RGn, 9. C-RGn.
Samples were distributed into three categories according to angle ANB: skeletal Class I: ANB 2° ± 2°, skeletal Class II: ANB > 4° and skeletal Class III: ANB < 0°, 16 and into two groups according to the gender. Of the samples 20% were reassessed after 2 weeks of initial assessment to test the reliability of the data. Kappa value for each parameter was calculated and perfect intra-observer agreement was observed. The Kolmogorov Smirnov test was done to evaluate the normality of data distribution. Descriptive statistics of the entire parameters were evaluated. An independent t-test was done to assess the gender dimorphism. An ANOVA test was used to check the mean differences among the variables within three categories according to skeletal types. Further, when there was significant difference, a post-hoc Tukey test was performed. The significance level was agreed at p ≤ 0.05. Pearson correlation test was done to evaluate the correlation among the hyoid bone position, pharyngeal dimensions, and anterior cranial base.18, 19
Results
The total sample consisted of 59 males and 91 females. The mean age of the samples was 20.30 ± 3.45 years. Each category of skeletal malocclusion consisted of 50 samples.
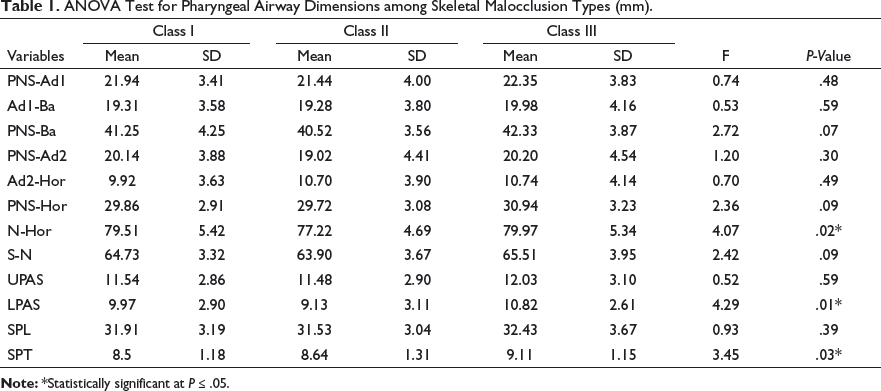
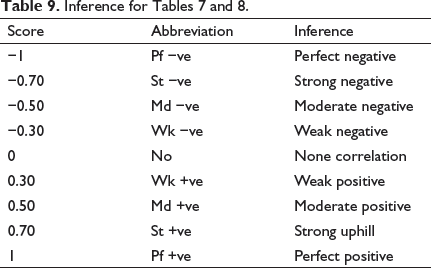
ANOVA Test for Pharyngeal Airway Dimensions among Skeletal Malocclusion Types (mm).
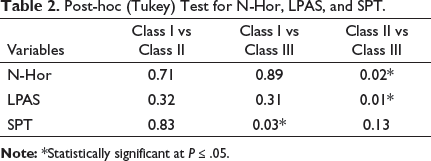
Post-hoc (Tukey) Test for N-Hor, LPAS, and SPT.
Analysis of Variance Test for Hyoid Bone Position Parameters among Skeletal Malocclusion Types (mm).
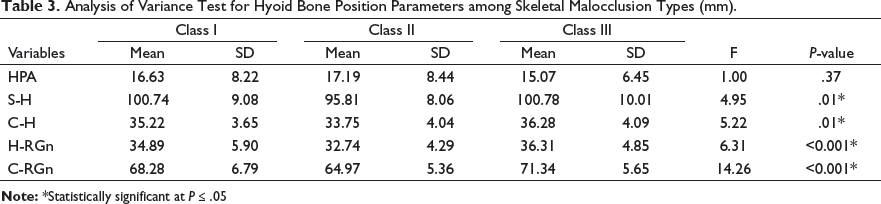
Post-hoc (Tukey) Test for S-H, C-H, H-RGn, and C-RGn.

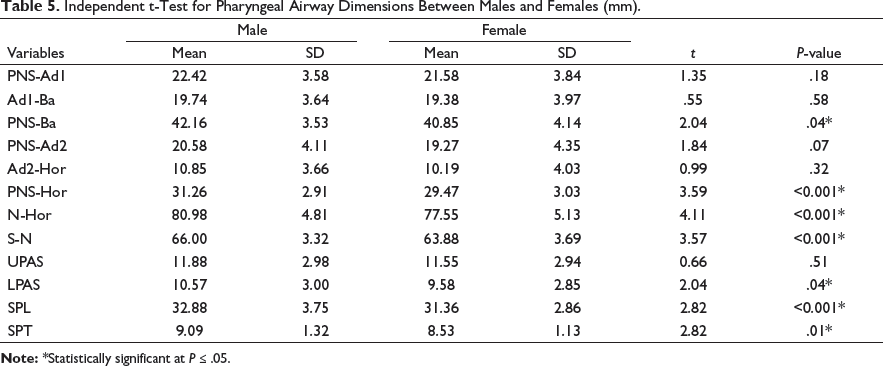
Independent t-Test for Pharyngeal Airway Dimensions Between Males and Females (mm).
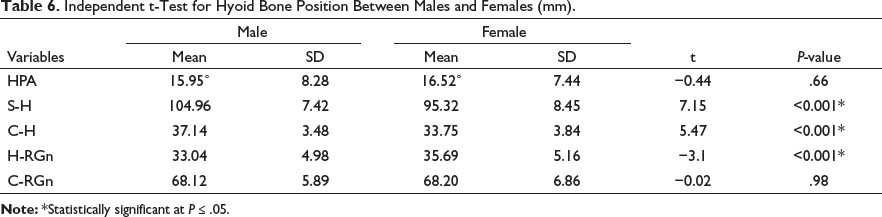
Independent t-Test for Hyoid Bone Position Between Males and Females (mm).
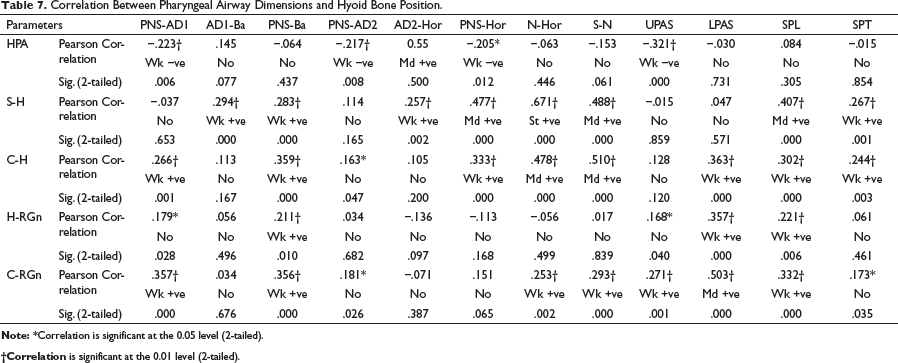
Correlation Between Pharyngeal Airway Dimensions and Hyoid Bone Position.
Correlation Analysis Between Anterior Cranial Base and Pharyngeal Airway Dimensions.

Discussion
Pharyngeal airway dimensions were seen to be the largest in skeletal Class III, followed by skeletal Class I and skeletal Class II. The dimensional differences that were significant were nasal fossa length (N-Hor), lower pharyngeal airway space (LPAS), and soft palate thickness (SPT). Nasal fossa length and lower pharyngeal airway space were found significantly larger in skeletal Class III as compared to skeletal Class II. These results are similar to the results of Muto et al, 20 Takemoto et al, 21 and Martin et al. 22 They established that the diameter of the pharyngeal airway was the highest in the mandibular prognathism, followed by the normognathic mandible, and the lowest in the retrognathic mandible. The mandible being positioned more anteriorly in prognathic patients results in a broader lower pharyngeal airway. Pharyngeal airway dimensions were greater in males compared to females, similar to the findings in the studies by Samman et al, 23 Guttal et al, 24 and Martin et al.22, 25
Hyoid bone was positioned farther ahead and inferiorly placed in skeletal Class III as compared to in skeletal Class I and skeletal Class II cases. Angular Measurement (HPA) was the largest in skeletal Class II and the smallest in skeletal Class III cases. The findings are similar to Galvao, 9 Allhaija and Al-Khateeb, 11 and Erdinc et al. 26 Dimensions of the hyoid triangle (C-H, H-RGn and C-RGn) of Class I samples were similar to the findings of Bibby and Preston. 27 The present study showed the hyoid plane angle to be lower in skeletal Class I samples. This might have resulted because the abnormalities in vertical dimensions were not considered while selecting the samples. Gender dimorphism in hyoid bone position was also noted by Allhaija and Al-Khateeb, 11 for which the reason is cited as the gender difference in neck thickness.
The position of the hyoid bone vertically (S-H) had a strong positive correlation with the length of the nasal fossa (N-Hor) and a moderate positive correlation with the upper airway width and soft palate length. The horizontal hyoid bone position relative to the cervical vertebrae (C-H) had a moderate positive correlation with the nasal fossa length. These relations are similar to Jose et al 28 and Costa et al. 29 The anterior cranial base (S-N) had a strong positive correlation with the nasal fossa length (N-Hor) and a moderate positive correlation with the lower airway width (PNS-Ba). It also had a moderate positive correlation with the vertical hyoid bone position (S-H) and horizontal hyoid bone position in relation to the cervical vertebrae (C-H). These correlations are in accordance with Shilpi et al 30 and Deljo et al. 31
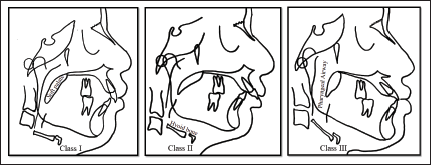
Figure 3 illustrates the dimensions of the pharyngeal airway space and the position of the hyoid bone in different varieties of malocclusion. Variations in the dimensions of the pharyngeal airway space and position of the hyoid bone occur in different skeletal patterns and gender groups in Nepalese adults. The close relationship of pharyngeal and hyoid bone morphologies in respiratory function and normal development of the craniofacial structure justify orthodontic interest. Proper understanding of pharyngeal morphologies and hyoid bone position is crucial in orthognathic surgery involving mandible, myofunctional/orthodontic treatment, besides in the management of obstructive sleep apnea. Thus, assessment of the pharynx and hyoid bone should be done in orthodontic assessment, as well as in the treatment outcome in related cases, to restore proper oral health in patients and greatly improve the quality of their life.
Example Tracings of Different Varieties of Malocclusion.
Conclusion
The following findings are observed in the present study:
Pharyngeal airway dimensions were the largest in Class III skeletal samples, followed by Class I samples, and the lowest in Class II samples. Sexual dimorphism was evident in the pharyngeal airway space dimensions, with male samples having larger pharyngeal airway dimensions.
The hyoid bone was found to be posteriorly and superiorly placed in Class II skeletal samples when compared to Class III and Class I skeletal samples. Male samples had the hyoid bone positioned significantly inferiorly and anteriorly when compared to female ones.
The anterior cranial base had a strong positive correlation with the nasal fossa length and a moderate positive correlation with the hyoid bone vertical position and lower airway width. The hyoid bone vertical position had a strong positive correlation with the length of the nasal fossa.
Footnotes
Acknowledgments
This research was presented as the thesis work for a postgraduate degree in orthodontics at Kathmandu University. The research work has been partially funded by University Grants Commission, Bhaktapur, Nepal (Small RDI Grant # SRDIG-74/75-HS-17). The authors would like to express sincere gratitude towards Dr. Sujita Shrestha, Dr. Rosina Bhattarai, and Dr. Sunita Khanal for their support in statistical analysis. We would also like to acknowledge Dr. Jyoti Dhakal, Dr. Ujjwal Pyakurel, Dr. Alka Gupta, faculties and colleague Dr. Diwash Adhikari, Department of Orthodontics, Kantipur Dental College.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.