
Abstract
Abstract
Aim: To cephalometrically evaluate the alterations taking place in the pharyngeal airway space, hyoid bone, soft palate, and head posture after mandibular setback surgery (bilateral sagittal split osteotomy) for correction of mandibular prognathism, as well as to evaluate the immediate postsurgical and more than 6 months postsurgical adaptations of these structures.
Setting and Design: A retrospective cephalometric study.
Materials and Method: The study group consisted of 40 nongrowing patients (20 females and 20 males) with mandibular prognathism and ANB less than or equal to –2 degree for which mandibular setback surgery by bilateral sagittal split ramus osteotomy was performed along with fixed appliance therapy. There presurgical (T1), immediate postsurgical (T2), and more than 6 months postsurgical (T3) lateral cephalograms were analyzed.
Statistical Analysis Used: Intragroup comparison was done by paired t-test.
Results: Skeletal measurements after orthognathic surgery remained stable in the long term. It was evident that mandibular setback surgery narrowed the pharyngeal airway; however, these changes were not significant except at the base of the tongue. During the follow-up airway measurements at the base of the tongue, the intersection of tongue at the inferior border of mandible and the vallecula increased but they did not reach the presurgical values. Soft palate length increased significantly after surgery. Angulation of soft palate to nasal line also increased significantly following surgery but decreased during follow-up. Extension of the head occurred after surgery which was maintained even at long term.
Conclusion: Careful analysis of airway should be performed, particularly in connection with large anteroposterior discrepancies and in those who have risk factors for development of obstructive sleep apnea. Such cases should be corrected by combined maxillary and mandibular osteotomies.
Introduction
Obstructive sleep apnea syndrome (OSAS) has recently received increased attention due to the multisystem complications associated with it and its high prevalence in adults. 1 The obstructive (peripheral) type of this syndrome is the most common form which is also known as occlusive apnea typically characterized by cessation of airflow due to upper airway obstruction despite simultaneous vigorous thoracic movement.2, 3 OSAS has been characterized by loud snoring, excessive daytime sleepiness, and intellectual deterioration. 4 Etiologic or predisposing factors postulated include an anatomically narrow airway, craniofacial deformities, muscular hypotony, sleep posture, and fatty deposits in the tissues of the upper airway apart from gender, age, and body mass index (BMI). 5 This condition can lead to reduction in blood oxygen saturation giving rise to hypertension and cardiac and pulmonary complications, and becoming potentially life threatening. 6
Studies in the literature state that mandibular advancements improved sleep apnea. If by interference, advancements improve the pharyngeal depth, setbacks should have an adverse effect? 7 A mandibular setback surgery is an important treatment modality in patients with skeletal Class III malocclusion with mandibular prognathism. It improves facial aesthetics, occlusion, and masticatory function by markedly changing the position of mandible.8-11 It may be hypothesized that since the mandible is surgically repositioned posteriorly relative to the other craniofacial structures, it leads to the tongue and hyoid bone being carried back and reducing the lumen of the oropharynx. 12 The changes in the pharyngeal airway space (PAS) after mandibular setback surgery remains controversial, with some studies showing a decrease in the anteroposterior dimension of the pharyngeal airway and others showing no change as compared to before surgery. 13
The aim of this study is to conduct a detailed cephalometric evaluation of the alterations taking place in the PAS, hyoid bone, soft palate, and head posture after mandibular setback surgery, bilateral sagittal split osteotomy, for correction of mandibular prognathism, as well as to evaluate the immediate postsurgical and more than 6 months postsurgical adaptations of these structures.
Materials and Method
Presurgical (T1), immediate postsurgical (T2), and minimum 6 months (8-18 months) postsurgical (T3) lateral cephalograms of patients with skeletal class III malocclusion because of mandibular prognathism were obtained from the file section of the Department of Orthodontics and Dentofacial Orthopedics.
The study group consisted of 40 patients (20 females and 20 males) who were nongrowing adults with mandibular prognathism and ANB in the range of –2 to –6 degrees for which mandibular setback surgery (4-8 mm) by bilateral sagittal split ramus osteotomy (Table 1) was carried out by the same surgical team with the same operative and postoperative regimes along with fixed appliance therapy. These patients did not have any congenital abnormalities and signs and symptoms of OSAS. All patients were of Davangere population with BMI less than 25, collar/size less than 40 cm with average throat length (38-42 mm for females and 40-45 mm for males) with no sag. Lateral cephalograms of the study subjects were obtained under standardized conditions using the same machine.
The analysis included various cephalometric landmarks, reference planes, and the linear and angular measurements done which were as follows (Figures 1-4):
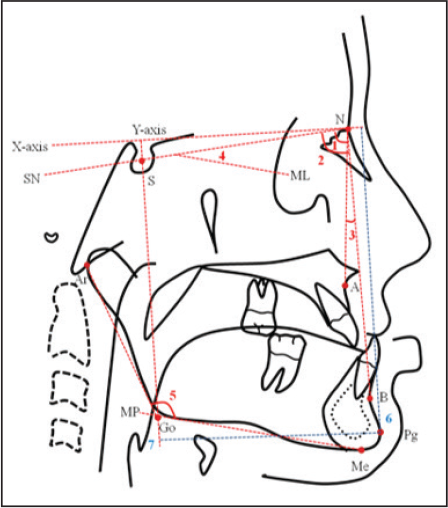
SKELETAL ANGULAR PARAMETERS FOR HARD TISSUE EVALUATION
SNA angle, SNB angle, ANB angle, Mandibular plane angle, Gonial angle
SKELETAL PARAMETERS TO DESCRIBE THE POSITION OF THE MANDIBLE
Pg Vertical, Pg Horizontal 14
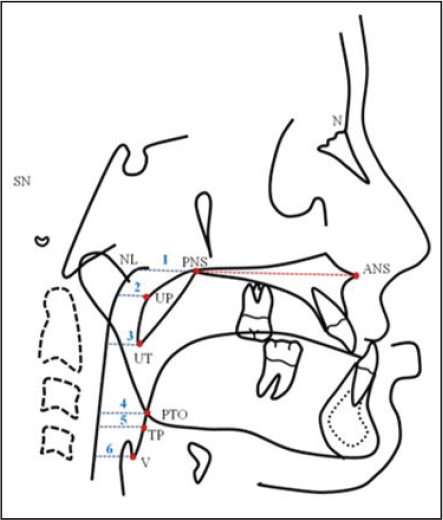
PARAMETERS TO EVALUATE THE AIRWAY 11
PPW-NL, PPW-UP, PPW-UT, PPW-PTO, PPW-TP, PPW-V15, 16
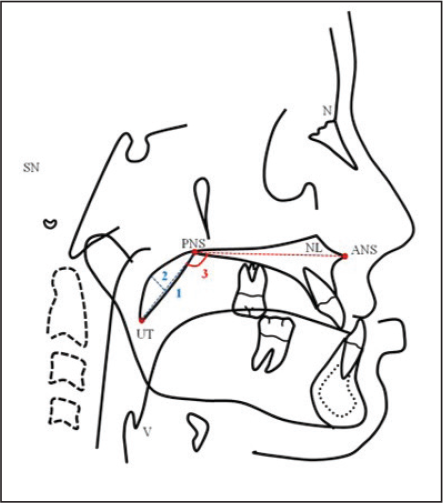
PARAMETERS TO DESCRIBE THE SOFT PALATE DIMENSION12, 17
Soft palate length, Soft palate thickness, Soft palate/NL angle 15, 17
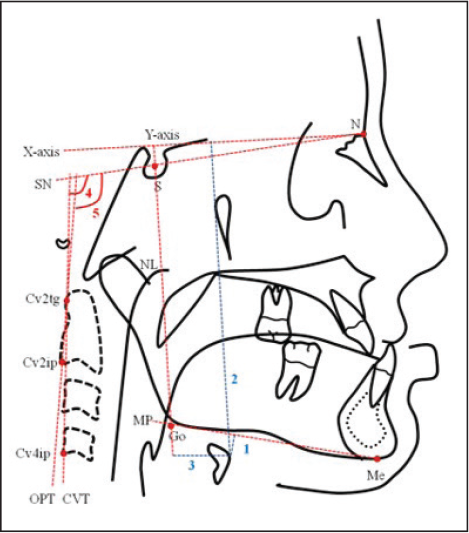
SKELETAL PARAMETERS TO DESCRIBE THE POSITION OF THE HYOID BONE15, 17
Hyoid-MP, Hyoid vertical, Hyoid horizontal
PARAMETERS TO DESCRIBE HEAD POSITION 16
Amount of Mandibular Setback (mm)
Skeletal Measurements
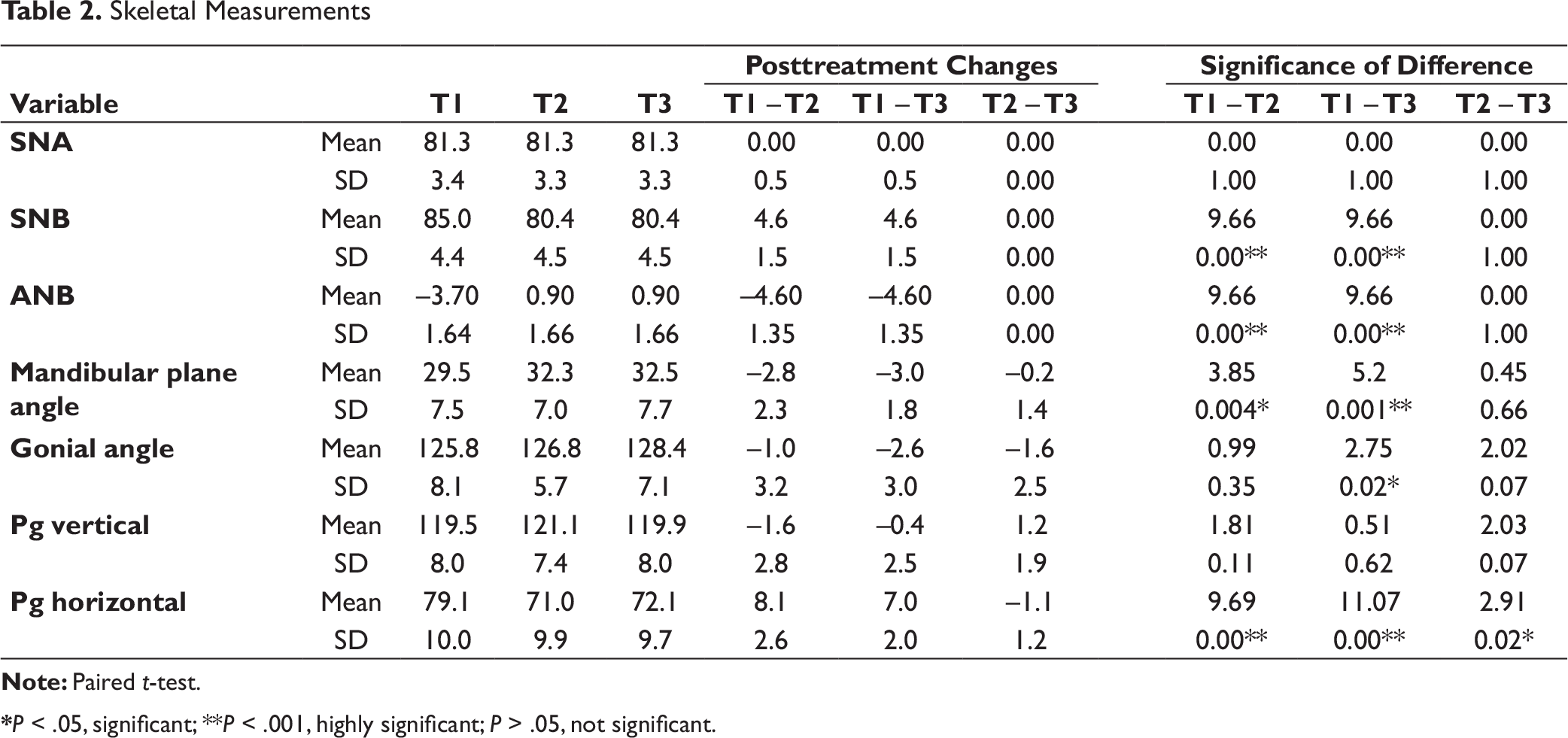
*P < .05, significant; **P < .001, highly significant; P > .05, not significant.
Pharyngeal Airway Measurements
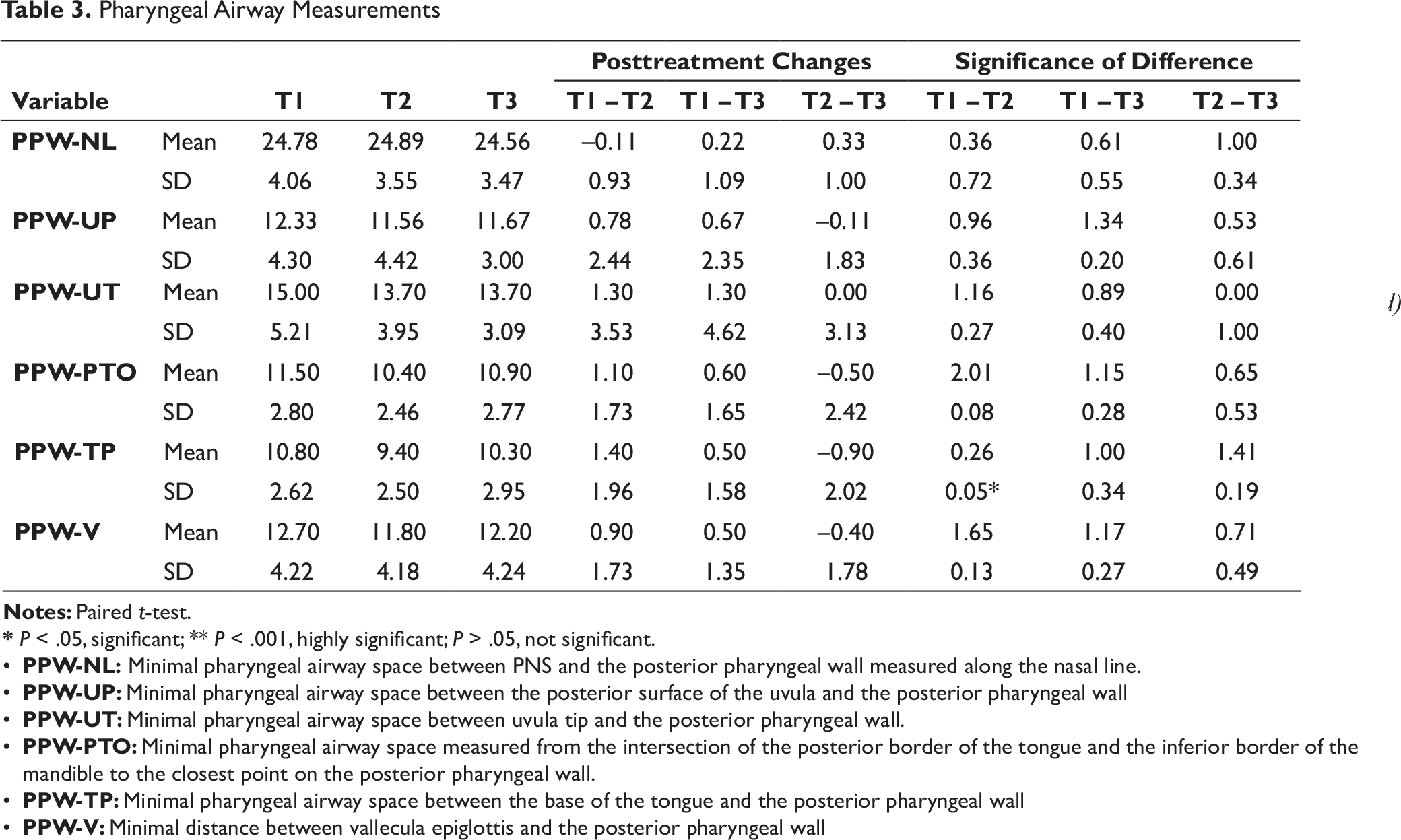
* P < .05, significant; ** P < .001, highly significant; P > .05, not significant.
• PPW-NL: Minimal pharyngeal airway space between PNS and the posterior pharyngeal wall measured along the nasal line.
• PPW-UP: Minimal pharyngeal airway space between the posterior surface of the uvula and the posterior pharyngeal wall
• PPW-UT: Minimal pharyngeal airway space between uvula tip and the posterior pharyngeal wall.
• PPW-PTO: Minimal pharyngeal airway space measured from the intersection of the posterior border of the tongue and the inferior border of the mandible to the closest point on the posterior pharyngeal wall.
• PPW-TP: Minimal pharyngeal airway space between the base of the tongue and the posterior pharyngeal wall
• PPW-V: Minimal distance between vallecula epiglottis and the posterior pharyngeal wall
Soft Palate Measurements
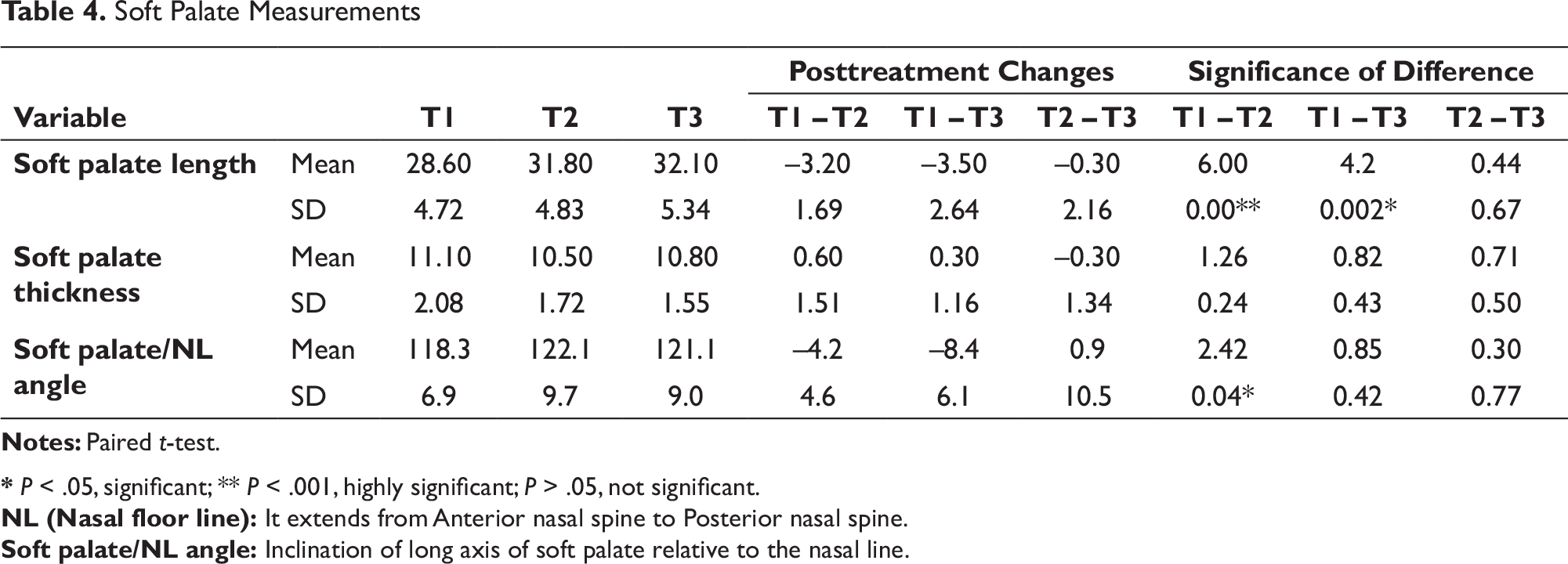
* P < .05, significant; ** P < .001, highly significant; P > .05, not significant.
NL (Nasal floor line): It extends from Anterior nasal spine to Posterior nasal spine.
Soft palate/NL angle: Inclination of long axis of soft palate relative to the nasal line.
A detailed cephalometric evaluation of the alterations taking place in the PAS, hyoid bone, soft palate, and head posture after mandibular setback surgery, bilateral sagittal split osteotomy, for correction of mandibular prognathism was carried out by the same operator. As well as evaluation of the immediate postsurgical and more than 6 months postsurgical adaptations of these structures was also checked. Intragroup comparison was analyzed by paired t-test. A P value < .05 was set for statistical significance.
Results
The results obtained from this study have been divided into 5 headings for description purpose:
The difference between the mean of T1 and T2 was found to be statistically highly significant for SNB angle, ANB angle, and Pg Horizontal. However, it was significant for mandibular plane angle. The difference between the mean of T1 and T3 was found to be highly significant for SNB angle, ANB angle, mandibular plane angle, and Pg Horizontal. However, it was significant for gonial angle. The difference between mean of T2 and T3 was found to be significant for Pg Horizontal.
The difference between mean T1 and T2 was found to be significant for PPW-TP.
Hyoid Bone Measurements
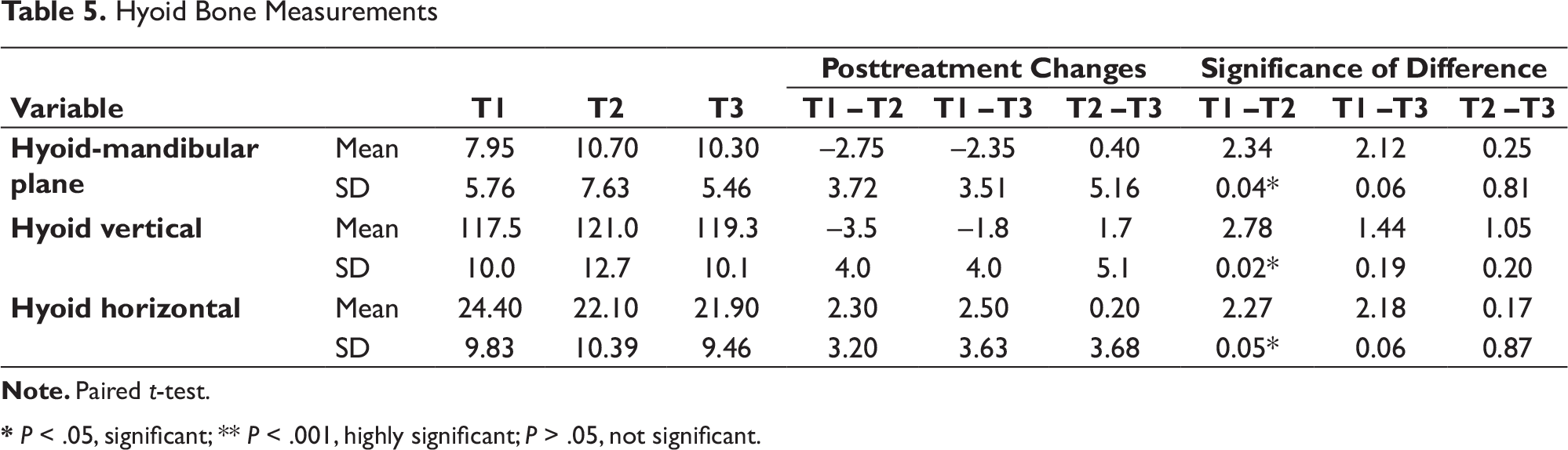
* P < .05, significant; ** P < .001, highly significant; P > .05, not significant.
Head Posture Measurements
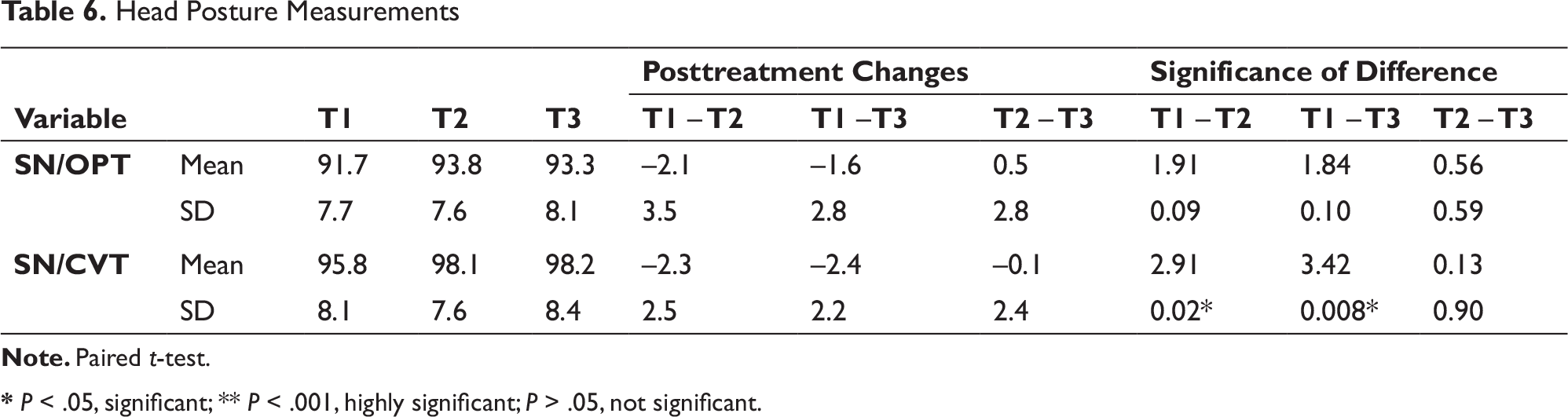
* P < .05, significant; ** P < .001, highly significant; P > .05, not significant.
The difference between mean T1 and T2 was found to be significant for H-MP, Hyoid vertical and Hyoid Horizontal.
The difference between mean T1 and T2 was found to be significant for SN/CVT and between T1 and T3 too for the same parameter.
Discussion
The aim of this study was to cephalometrically evaluate the alterations taking place in the PAS, hyoid bone, soft palate, and head posture after mandibular setback surgery, bilateral sagittal split osteotomy for correction of mandibular prognathism, as well as to evaluate the immediate postsurgical and more than 6 months postsurgical adaptations of these structures.
Effect on Skeletal Measurements
SNA angle did not show any changes including the follow up. After surgery the SNB angle was found to have decreased on average by 4.6 degree while ANB angle increased on average by 4.6 degree since a mandibular setback surgery was performed. No significant difference was seen from postsurgical to follow-up. These results showed that these skeletal measurements after orthognathic surgery were retained and remained stable in the long term. These changes are similar to previous studies on the stability of orthognathic surgery to correct Class III skeletal deformities.8, 10
Mandibular plane angle increased significantly from T1 to T2 and T1 to T3, indicating that mandible was rotated clockwise during surgery. However, it did not increase significantly from T2 to T3, indicating that there was negligible change in the mandibular plane from immediate postsurgery to follow up. Similarly, the gonial angle increased from T1 to T2 to T3. However, only significant change was from T1 to T3, indicating increase in the inclination of posterior border of ramus to the mandibular plane following surgery. In spite of these changes, stable occlusion was maintained in all cases because of postoperative orthodontic alignment. Other studies have also found similar changes in the mandibular plane angle postoperatively. 18
Vertically, the mean inferior movement at pogonion was 1.6 mm at surgery and it relapsed back upward during follow-up, but it did not reach the presurgical level. Pg horizontal decreased on average by 8.1 mm indicating the amount of setback of the mandible. There was a relapse of 1.1 mm from postsurgery to follow-up. Similar findings were noted by few other studies.12, 19 Eggensperger et al found a skeletal relapse of 1.3 mm measured at pogonion, amounting to 23% of surgical setback after 1 year. 14 However, Kitagawara et al found no significant horizontal relapse after surgery. 18
Effect on Pharyngeal Airway Measurements
Most cephalometric studies of airway diameters in OSAS have used conventional skeletal reference points to define lines along which airway diameters were measured. Reference lines dictated by the facial skeletal morphology are very prone to be altered at osteotomy and usually do not represent minimum cross-sections. To rule out these discrepancies, the definitions of airway diameters used in the present study were narrowest diameters of the airway at different landmarks. 20
Since a two-dimensional lateral cephalogram has been used to evaluate three-dimensional pharyngeal airway and hyoid bone, its validity can be questioned and CT might be considered a better option instead. However, Riley and Powell have reported a high reliability of CT scans and cephalograms in determining the posterior airway space with statistically significant correlation between posterior airway space and volume of the pharyngeal airway. 12 Therefore, lateral cephalograms are still used widely in the assessment of sleep apnea and craniofacial form. Its advantages include wide accessibility, simplicity, low expenditure, minimal radiation exposure, and ease of comparison with extensive normative data and other studies.9-11
Pharyngeal airway space along the nasal line showed no significant changes from T1 to T2 to T3. Minimum airway distance between the soft palate and pharyngeal wall, and the distance between the uvula tip and posterior pharyngeal wall showed a decrease from T1 to T2 but no change from T2 to T3. This indicated that the airway decrease after surgery although not significant remained stable in the follow-up. Whereas airway measurements at the intersection of tongue to the inferior border of mandible, at the base of the tongue, and at the vallecula showed a decrease in the PAS from T1 to T2 but an increase from T2 to T3. Although the measurements at T3 were larger than T2 they did not reach the T1 values.
Saitoh, Eggensperger et al, and Marsan et al found significant decrease in pharyngeal airway size at all levels after mandibular setback surgery.8, 14, 21 Eggensperger et al stated the continuation of decrease in the sizes of the upper and middle pharyngeal airways with time. 14 However, the lower pharyngeal airway diameter remained almost unchanged.
Chen et al, Kitahara et al,, and Liukkonen et al found a significant reduction in the pharyngeal airway at the oropharyngeal and hypopharyngeal levels.10, 11, 22
Other study which showed contradictory results was that of Kitagawara et al in which the nasopharyngeal depth significantly increased 3 days after surgery and posterior airway space was stable during the whole period. 18 However, Tselnik and Pogrel noted that mandibular setback surgery resulted in an initial increase in both the area and anteroposterior dimension of the PAS which was followed by a significant long-term decrease in both parameters. 23
Hochbanet et al have reported larger than average preoperative airway space in patients with prognathic mandible and following mandibular setback surgery airway size decreases to values within a normal range. 24 The findings of this study do not support this postulate, preoperative airway size was found to be on average 11.5 mm at the intersection of the posterior border of the tongue and the inferior border of the mandible to the closest point on posterior pharyngeal wall, thereby corresponding to normal values by Mc Namara (10-12mm). 25 This finding is in accordance with that reported by Liukkonen et al. 22
Kim et al and Degerliyurt et al reported that the pharyngeal dimensions after surgery did not demonstrate sex dimorphism.26, 27 However, few found gender difference in the airway after surgery.26, 28 Due to these contradictory results in literature the number of males and females taken in this study were equal to eliminate gender bias.
Effect on Soft Palate Measurements
Soft palate length increased from T1 to T2 to T3. There was significant increase from T1 to T2 and from T1 to T3. Similar changes were noted by Achilleos et al and Saitoh.8, 12
Soft palate thickness reduced from T1 to T2 and increased from T2 to T3 but these changes were not statistically significant. This was in accordance with the findings of Achilleos et al 12
Angulation of soft palate to nasal line increased significantly from T1 to T2. Although it decreased from T2 to T3, but this change was not statistically significant. Similar changes were noted by Achilleos et al, Saitoh, Marsan et al, and Kim et al8, 12, 21, 26 Significant alteration in the soft palate inclination reflected changes in the oropharyngeal airway space that is as the angle increased from T1 to T2, the minimal airway between the soft palate and the posterior pharyngeal wall decreased. From T2 to T3 as the inclination of the soft palate to the nasal line decreased that is as the soft palate moved away from the posterior pharyngeal wall, this airway measurement increased.
Both the tongue and soft palate positions influence the pharyngeal airway size. Mandibular setback surgery shifts the tongue posteriorly, hence causing the soft palate to extend posteriorly leading to change in its length, angulation, and altering pharyngeal airway measurements. Although some studies attribute mandibular setback group to be at a greater risk of developing obstructive sleep apnea, at the same time the compensatory mechanisms in the soft palate explains their probability of being at a low risk.
Effect on Hyoid Bone Measurements
Following mandibular setback surgery, the hyoid bone moved inferiorly with respect to the mandibular plane as well as the true horizontal. This is consistent with findings of other studies.29, 30 This movement is thus a physiologic adaptation to prevent hyoid-related encroachment on the pharyngeal airway following mandibular setback surgery. However, during long-term follow-up, the hyoid bone tended to move up slightly, although not significant. While the hyoid bone tends to return to its preoperative position, it never regained its original location with respect to both the mandibular plane and the true horizontal. Mean displacement therefore from T1 to T3 was also in an inferior direction and changes in hyoid in the vertical plane from presurgical to follow-up were not statistically significant.
However, Achilleos et al, Kitahara et al, and Kitagawara et al found that the hyoid bone moved inferiorly at short-term follow-up, a transient finding as the long-term follow-up showed a significant elevation of the hyoid bone almost to its presurgical level.11, 12, 18 There are conflicting views on the degree and duration of the postoperative changes in the hyoid bone position and PAS decrease. Eggensperger et al also found inferior movement of the hyoid bone; however, after 11 years they found that the hyoid bone moved further inferiorly. 14 Whereas Kim et al noted no inferior displacement of the hyoid in both males and females,26 a few found significant downward displacement of the hyoid bone one year postoperatively in males. 28 Although a similar tendency was seen in females this trend was insignificant.
In this study, the hyoid bone moved posteriorly toward the pharyngeal wall from T1 to T2 to T3, but only changes from T1 to T2 were statistically significant. This is in accordance with the study by Kim et al 26 Significant narrowing of minimal airway distance at the base of the tongue immediately following surgery is due to this posterior and inferior movement of tongue represented by the hyoid bone changes.
Kitahara et al and Eggensperger et al also found significant posterior movement of the hyoid immediately after orthognathic surgery.11, 14 But during the follow-up stage they found that the hyoid bone moved forward. It however did not fully regain its original preoperative position, whereas Achilleos et al noted insignificant changes in the anteroposterior relationship of the hyoid bone. 12
In contrast, Tselnik and Pogrel observed an early downward and forward movement of the hyoid bone as a part of physiological adaptation to preserve airway patency. 23
Effect on Head Posture Measurements
SN/OPT showed increased angular measurements between T1 and T2 and decreased from T2 to T3, but none of these changes were statistically significant. However, SN/CVT increased from T1 to T2 to T3, only changes from T1 to T2 and T1 to T3 were statistically significant. It indicated extension of the head which was maintained even at long term after setback. Thus, cervical hyperflexion had taken place after correction of mandibular prognathism.
Achilleos et al and Gu et al also reported that the head posture was raised as a result of mandibular setback surgery.12, 30
The immediate response to setback surgery involves the musculature of the neck and frequently leads to a different head posture. An altered head posture was found to influence the position of the hyoid bone that is as the craniocervical angle increased significantly at follow-up the hyoid bone moved upward toward its original position. This finding could indicate long-term adaptation to maintain airway patency.
Thus, skeletal relapse and the size of the airway can be clinically seen due to postoperative changes in the pharyngeal complex. Suprahyoid musculature relaxation can be attributed to the postoperative positional alterations of the hyoid bone. This decreased suprahyoidal musculature tension may change the muscular balance within the head and neck, thus resulting in an increased forwardly directed force exerted by the neck muscles and hence leading to pulling the mandible forward again. 30 However, the long-term biomechanical adaptation of the tongue, supra and infra hyoid, and all neck muscles balance the stomatognathic system resulting in increase in the airway during the follow-up. The net result was a decrease in the airway from presurgical to follow-up; however, these values were neither clinically nor statistically significant.
Conclusion
Skeletal measurements after orthognathic surgery were retained and remained stable in the long term.
It is seen that mandibular setback surgery causes narrowing of the pharyngeal airway; however, these changes were not significant except at the base of the tongue. During the follow-up, airway measurements at the base of the tongue, intersection of tongue to the inferior border of mandible, and the vallecula increased but they did not reach the presurgical values. Soft palate length increased significantly after surgery. Angulation of soft palate to nasal line also increased significantly following surgery but decreased during follow-up. Extension of the head occurred after surgery which was maintained even at long term. Compensatory changes of the hyoid, soft palate, and cervical musculature should be taken into consideration when planning mandibular setback osteotomies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.