
Abstract
Aim:
To examine pharyngeal airway dimensions and hyoid bone position according to the subgroups of Class III malocclusion.
Materials and Methods:
This retrospective study consisted of patients divided into three subgroups with skeletal Class III malocclusion. The study included a total of 151 individuals (61 females and 90 males). The authors divided individuals with skeletal Class III malocclusion into three subgroups: maxillary retrognathia, mandibular prognathia, and combined. The study’s cephalometric analysis used eight nasopharyngeal, seven oropharyngeal, two hypopharyngeal, nine hyoid, and four area measurements. One-way analysis of variance was used to evaluate patients. Tukey’s post-hoc tests were used for bilateral comparisons of significant parameters. The results were considered statistically significant at a P < .05 significance level.
Results:
The study found no significant differences between the groups’ pharyngeal airway and area measurements (P > .05). When the authors evaluated hyoid bone position, a statistically significant difference was found between the three groups’ Hy-A (mm), Hy-S (mm), Hy-SN (mm), and Hy-FH (mm) measurements (P < .05).
Conclusion:
Linear and areal pharyngeal airway dimensions are similar in subgroups of Class III malocclusions, while the hyoid bone is vertically higher in individuals with maxillary retrognathia.
Introduction
Skeletal Class III malocclusion is characterized by maxillary retrognathia or insufficiency, mandibular prognathia, and/or increased mandibular growth. Clinically, Class III patients have a concave profile since the lower face is protrusive and the middle face is retrusive.1,2 Craniofacial growth development has a complex and multifactorial structure. 3 Pharyngeal airway, head posture, functional anterior displacement, and vertical as well as sagittal skeletal relationship can be affected by factors such as maxilla and mandible positions.4–11
In pharyngeal airway studies of Class III patients, the oropharyngeal area has been reported to be wider and flatter, the tongue is located lower, and the palatinal tonsils are hypertrophic. Reports have also shown that the oropharyngeal region is wider in Class III individuals than in Class II individuals. 12 Takemoto et al. evaluated the pharyngeal airway dimensions of prepubertal individuals with Class III malocclusion using cephalometric measurements. They found that females with Class III malocclusion had a lower pharyngeal airway size, however, larger than females with Class I occlusion. 13
A study by Alves et al. comparing the airway sizes of patients with Class II and Class III malocclusion in the prepubertal period using cone beam computed tomography reported that the individuals with Class III malocclusion had a larger nasopharyngeal airway size than individuals with Class II malocclusion. 14 In addition, while the oropharyngeal airway sizes of patients with mandibular prognatism were measured at high values, the nasopharyngeal and hypopharyngeal dimensions were reported to be independent of sagittal mandibular development. 15 Individuals with Class III malocclusion were found to have wider oropharyngeal and hypopharyngeal airway sizes than individuals with Class I and Class II malocclusion.
The literature shows that many studies have examined Class III malocclusions alongside other malocclusions in terms of both pharyngeal airway dimension and hyoid bone position. However, these studies are limited to comparing pharyngeal airways among the subgroups of Class III malocclusion with subgroups defined by individuals’ jaws, from which the condition originates. 16
The aim of this study is to examine the pharyngeal airway sizes and hyoid bone position according to subgroups of Class III malocclusion. Our initial hypothesis is, “There is no difference between different subgroups of patients with Class III malocclusion in terms of pharyngeal airway size and hyoid bone position.”
Materials and Methods
Setting and Design
Ethical approval of this retrospective study was obtained from the Clinical Research Ethics Committee of Suleyman Demirel University. We evaluated patients with Class III malocclusion who were treated at our clinic at Süleyman Demirel University (Faculty of Dentistry, Department of Orthodontics) between June 2018 and June 2019. The authors determined Class III individuals according to their ANB angle and divided them into three groups using SNA and SNB angles. The sample size was calculated based on a power analysis using G* Power analysis (G* Power Ver.3.0.10, Kiel, Germany) for superior airway space at an alpha error probability of 0.05 and a power of 90%. 17 The power analysis showed that, at minimum, 32 individuals were required for each subgroup. In order to increase the study’s power, the authors included more individuals.
Sampling Criteria
The inclusion criteria for the present study comprised the absence of any craniofacial anomalies or systemic disorders, the absence of airway pathologies, adequate imaging quality for cephametric radiographs, and no history of previous orthodontic treatments. The study excluded patients whose head postures were erroneous during radiographic exposure, patients over 17 years of age, and patients with artifacts on their radiographs. The authors obtained patients’ radiographs only from the device at our clinic used for orthodontic patients. While the authors obtained the radiographs, patients’ heads were fixed with cephalostat and exposure was made using a natural head posture with the help of a mirror located opposite the device (Planmeca [Planmeca Promax, Helsinki, Finland] device, 85 kV and 8 mA, during a 15-s exposure time). In addition, patients’ heads were fixed with cephalostat and radiographs were obtained while the teeth were in centric occlusion. Although the authors routinely performed this standardization for each patient, we excluded the patients who kept their heads under extension or flexion during radiography from the study. A total of 151 individuals (61 females and 90 males) were included in the study from 608 patients who were blindly included in our evaluation.
Study Method
The ANB (ANB < 0°) angle was used to distinguish individuals with skeletal Class III malocclusion. 18 The SN/GoGn angle was used to distinguish also normodivergent individuals (26° < SN/GoGn <38°). Individuals with skeletal Class III malocclusion were divided into three subgroups: maxillary retrognathia (SNA < 80°, Group 1, 44 patients), mandibular prognathia (SNB > 82°, Group 2, 59 patients), and combined (SNA < 80° and SNB > 82°, Group 3, 48 patients). The authors also compared airway measurements and hyoid measurements.
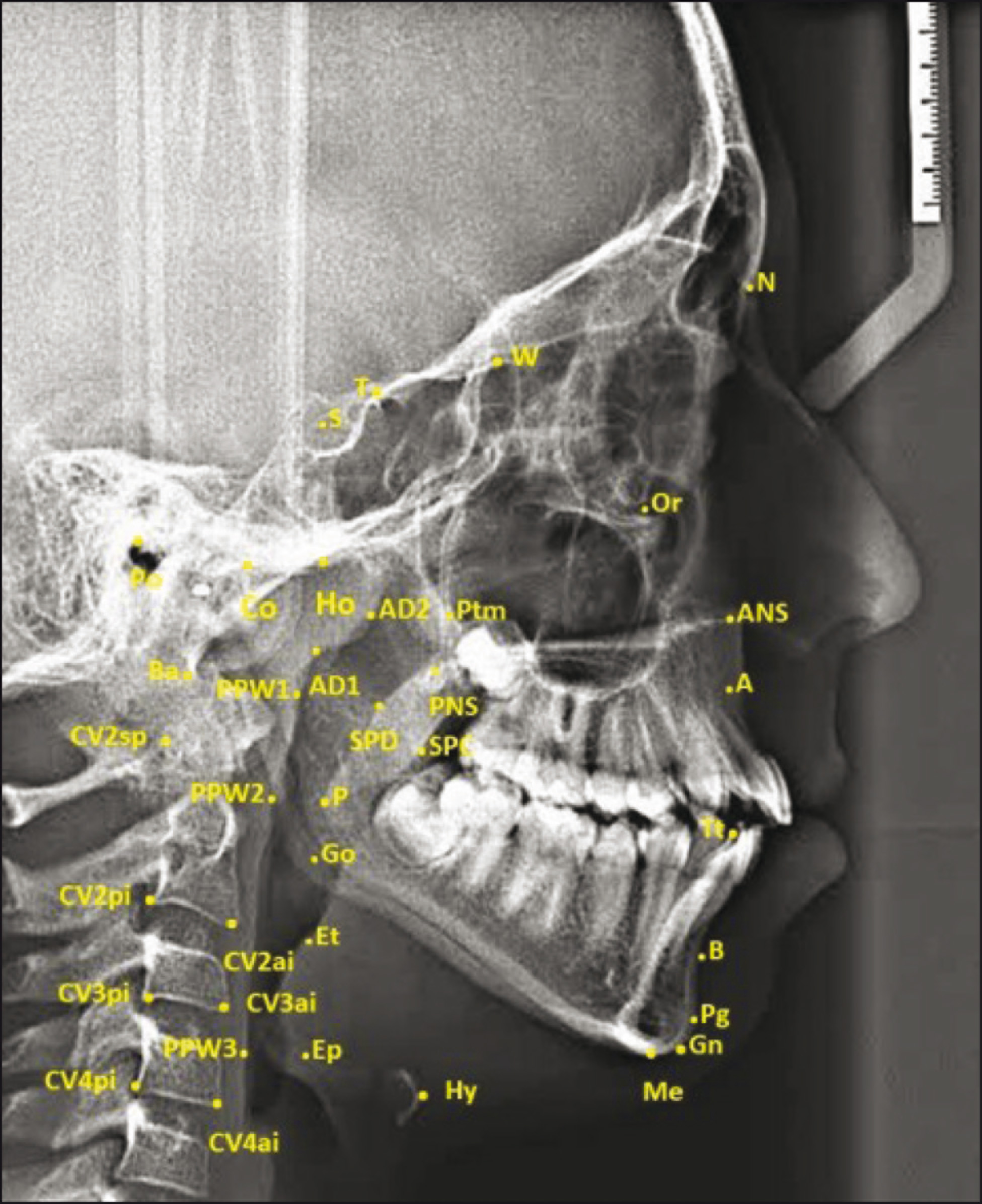
Cephalometric Landmarks Used in Study
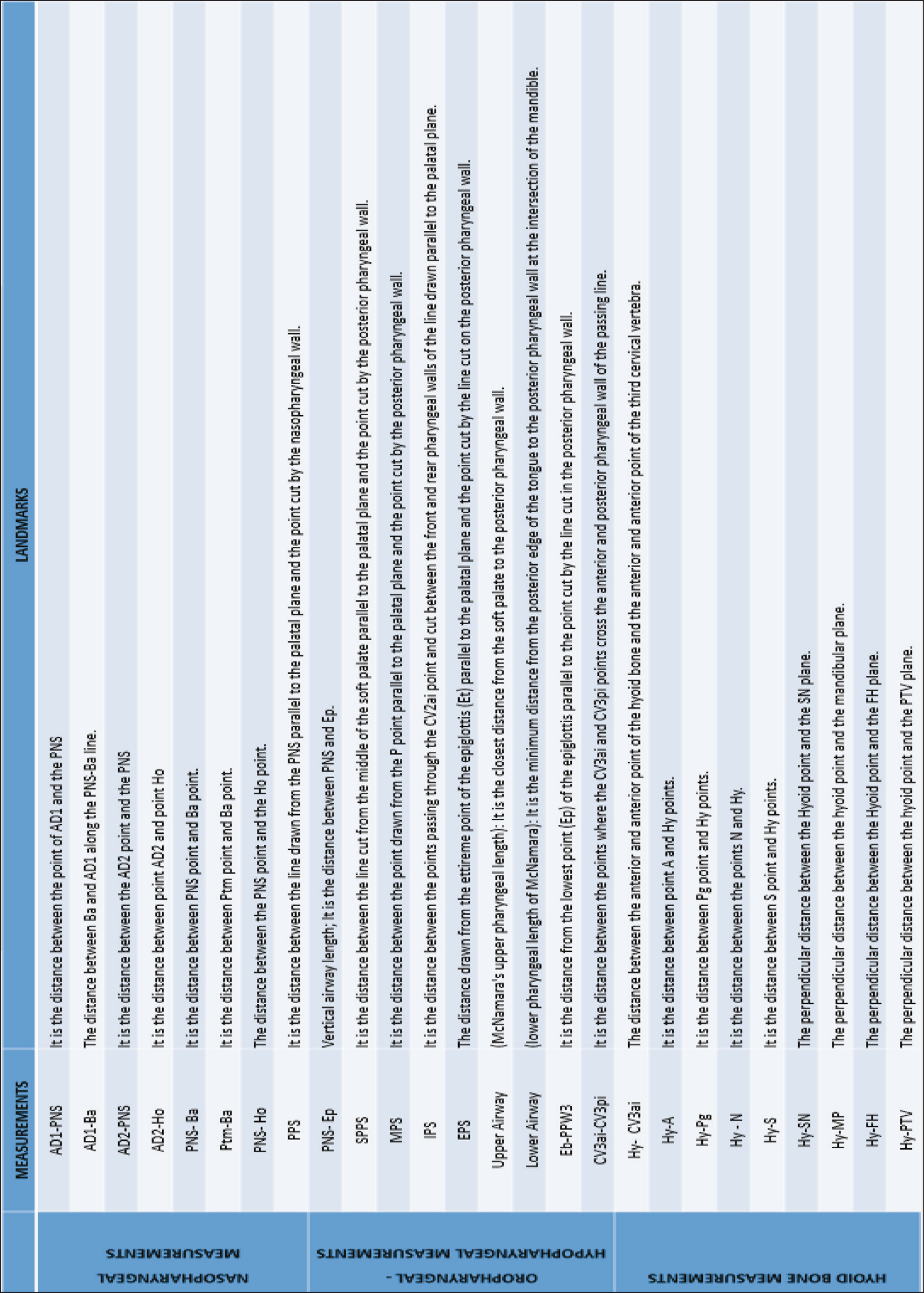
Measurements and Explanations Used in Study
Cephalometric Analysis
The study used NemoCeph software (NX 2009 for Windows, Nemotec, Madrid, Spain) for linear measurements and SketchAndCalc software (SketchAndCalc Area Calculation software, Axiom Welldone,
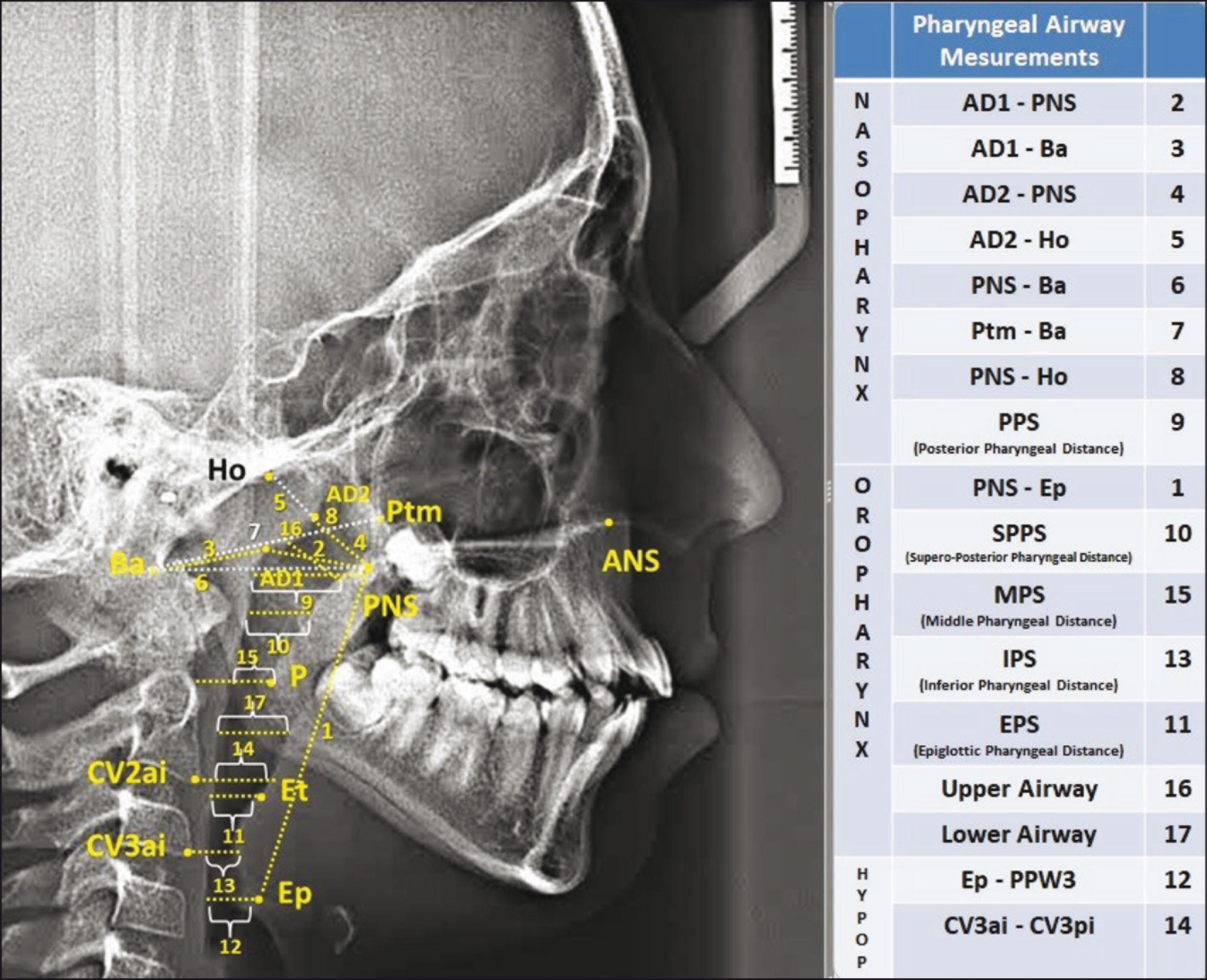
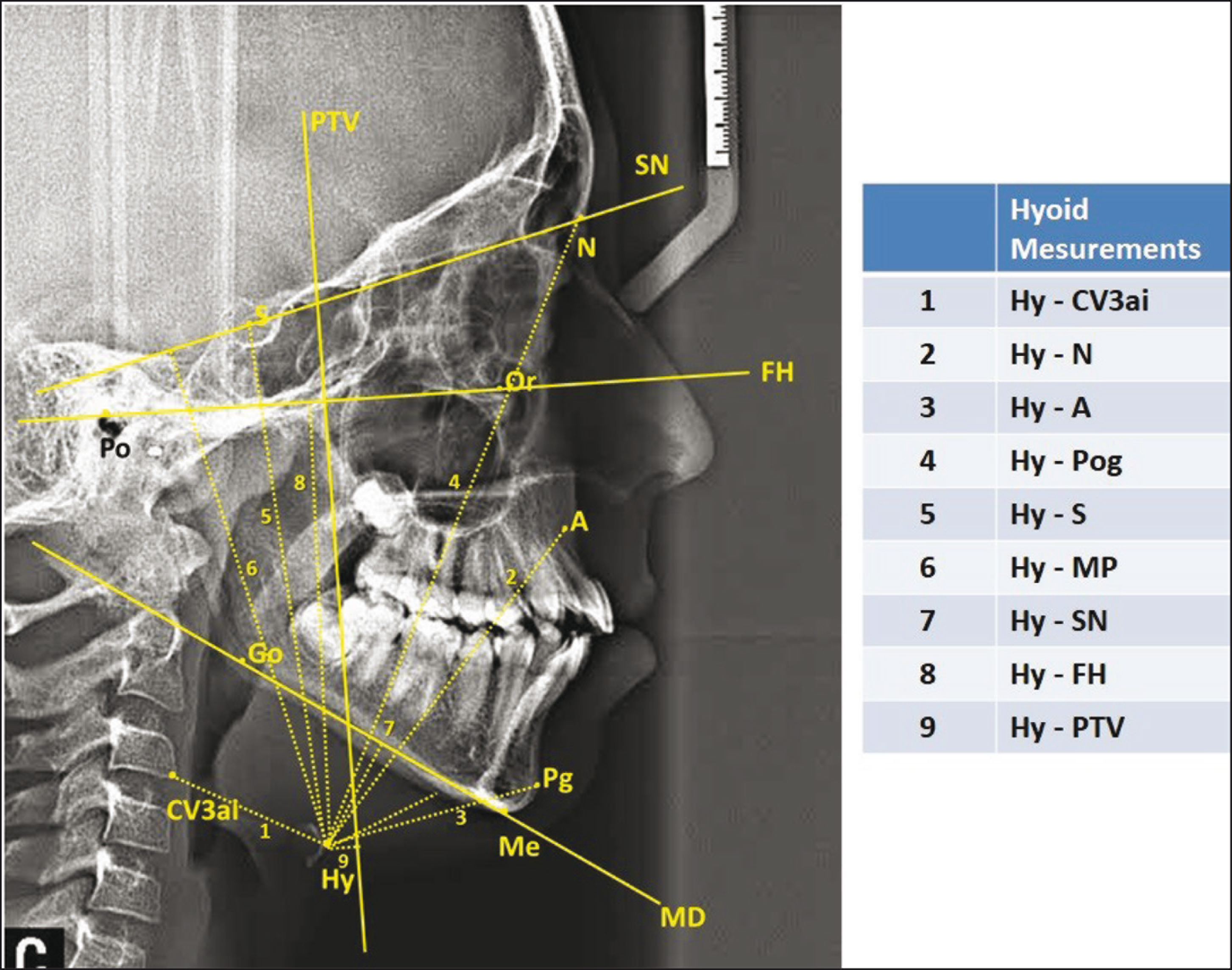
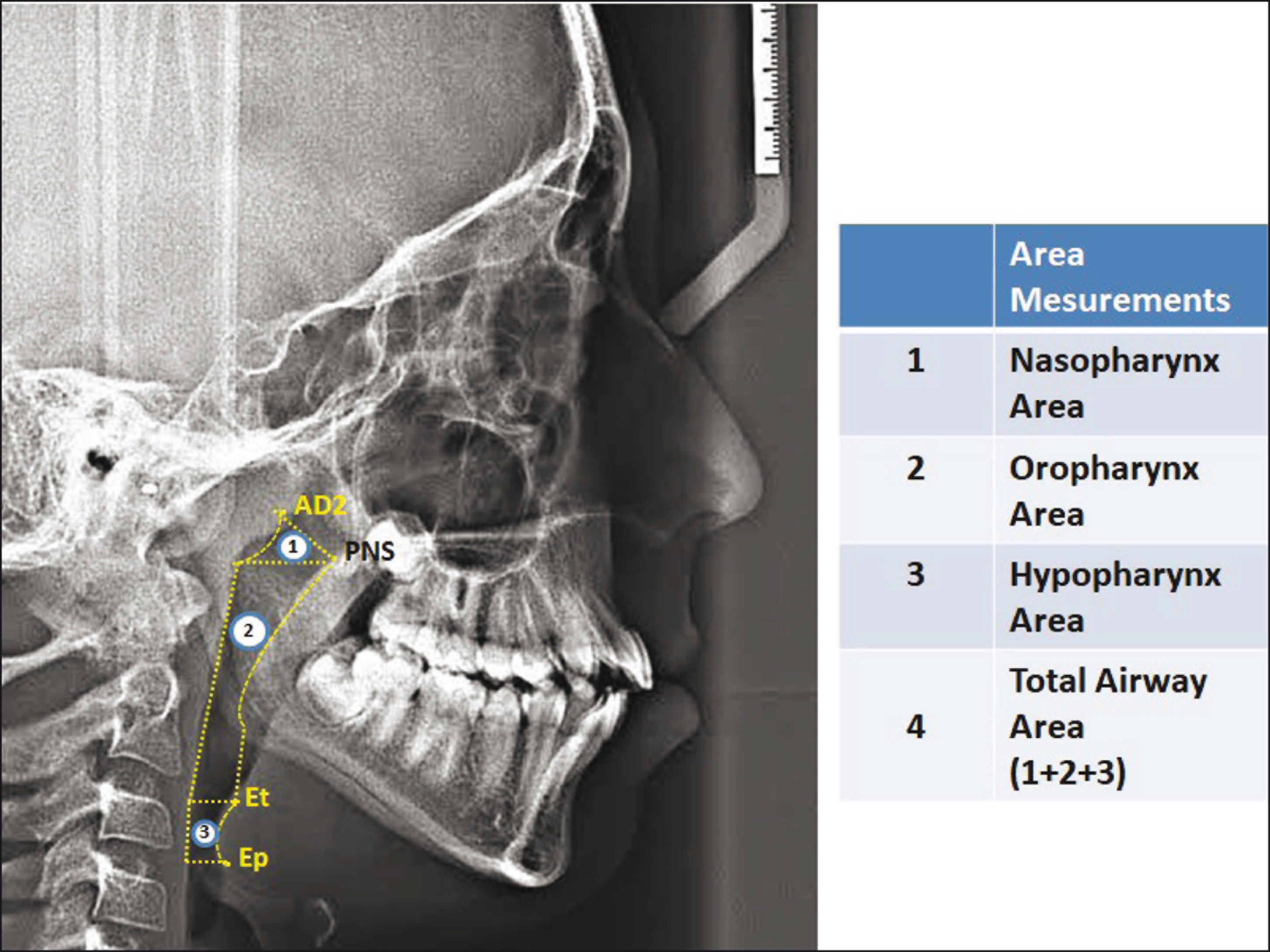
In addition, the study used 35 cephalometric points (Figure 1), eight cephalometric planes, and 30 cephalometric measurements (Figure 2). The cephalometric analysis used five craniofacial, eight nasopharyngeal, seven oropharyngeal, two hypopharyngeal (Figure 3), nine hyoid (Figure 4), and four area measurements (Figure 5).
Statistical Analysis
The authors used a Kolmogorov–Smirnov test to determine whether the data had a normal distribution. Since the parameters evaluated in the study were generally distributed homogenously in the subgroups, parametric tests were used.
The distribution of patients’ sex and growth development (CVM—cervical vertebral maturation) stages were compared with Pearson’s chi-square test. In determining the growth and development period, we used the Lamparski method to identify the cervical vertebral maturation period, using lateral cephalometric films taken at the beginning of patients’ treatment. Among all three of the study’s groups, it was seen that individuals in the pre-peak and peak periods (CS2–CS3) were the majority. The authors used one-way analysis of variance to evaluate patients subdivided according to Class III malocclusion. For bilateral comparisons, Tukey’s post-hoc tests were used. To determine the measurements’ error margin, the authors randomly selected 40 of the 151 lateral cephalometric films for remeasurement by the same researcher who had conducted the first measurements. Cronbach α coefficients were determined for each measurement. For each measurement, the repeatability coefficients were found to be high (α ≥ 906).
The authors used an SPSS package program (SPSS for Win, Ver.20.0; SPSS Inc., Chicago, Ill.) for data analysis. The results were considered statistically significant at a P < .05 significance level.
Results
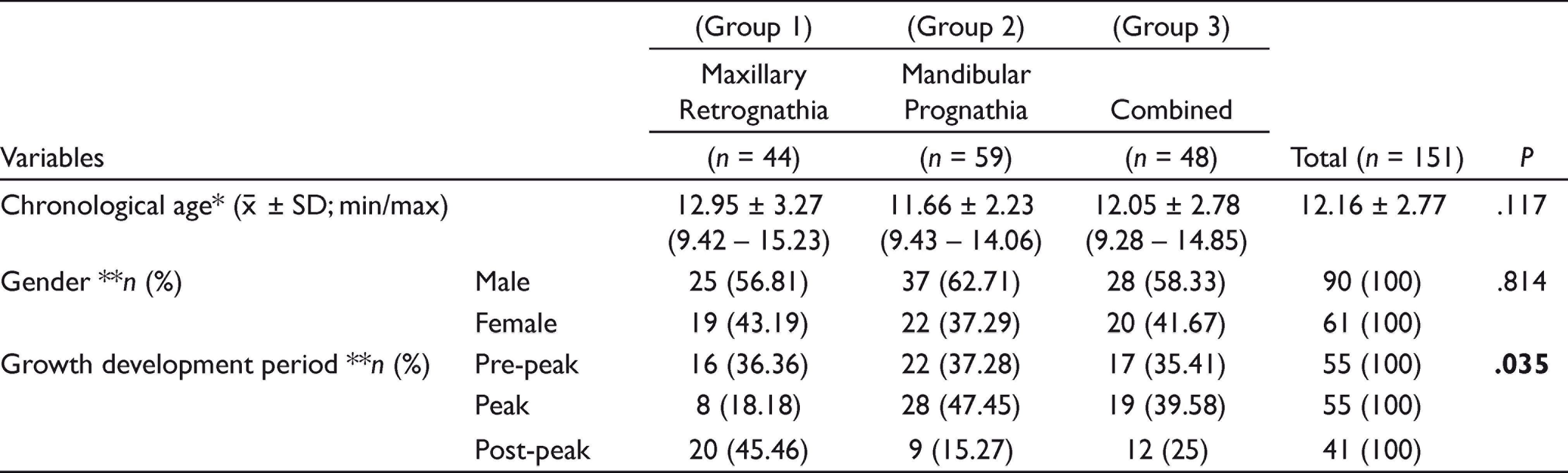
Table 1 shows the distribution of patients with skeletal Class III malocclusion included in the study, according to chronological age, gender, and growth development period. The mean age of the 151 patients (61 females and 90 males) with Class III malocclusion in this study was 12.16 ± 2.77 years. Of the Class III patients in this study, 29% had maxillary retrognathia (44 patients: 19 females, 25 males; mean age, 12.95 ± 3.27 years), 39% had mandibular prognathia (59 patients: 22 females, 37 males; mean age, 11.66 ± 2.23 years), and 32% were identified as “combined” (48 patients: 20 females, 28 males; mean age, 12.05 ± 2.78 years). Most Class III patients (55 patients—36.42%) were in pre-peak and peak growth periods.
Pharyngeal Airway Measurements Used in Study
Hyoid Measurements Used in Study
Area Measurements Used in Study
The authors observed no significant relation between the types of Class III malocclusion and chronological age or gender (P > .05). However, the authors observed a significant relationship between the types of Class III malocclusion and growth development periods (P < .05). When the authors examined the effects of the subgroups of skeletal Class III malocclusion on the pharyngeal airway, they observed no statistically significant difference between the three groups separated by the types of skeletal Class III malocclusion in the nasopharyngeal, oropharyngeal, and hypopharyngeal parts (P > .05; Table 2).
Demographic Data According to the Subgroups of Skeletal Class III Malocclusion
With the study’s measurements, the author evaluated the position of the hyoid bone and found a statistically significant difference between the three groups’ Hy-A measurements (mm; P < .05). When the authors examined the results of the Tukey’s test, they observed that the mandibular prognathia group’s results were statistically significantly higher than that of the other two groups. The maxillary retrognathia group’s Hy-S (mm) measurements were statistically significantly higher than that of the other two groups (P < .05). The mandibular prognathia group’s Hy-SN (mm) and Hy-FH (mm) measurements were statistically significantly higher than that of the other two groups (P < .05; Table 3). There was no statistically significant difference between the three groups’ field measurements (P > .05; Table 3).
Comparison of Pharyngeal Airway Measurements According to the Subgroups of Skeletal Class III Malocclusion
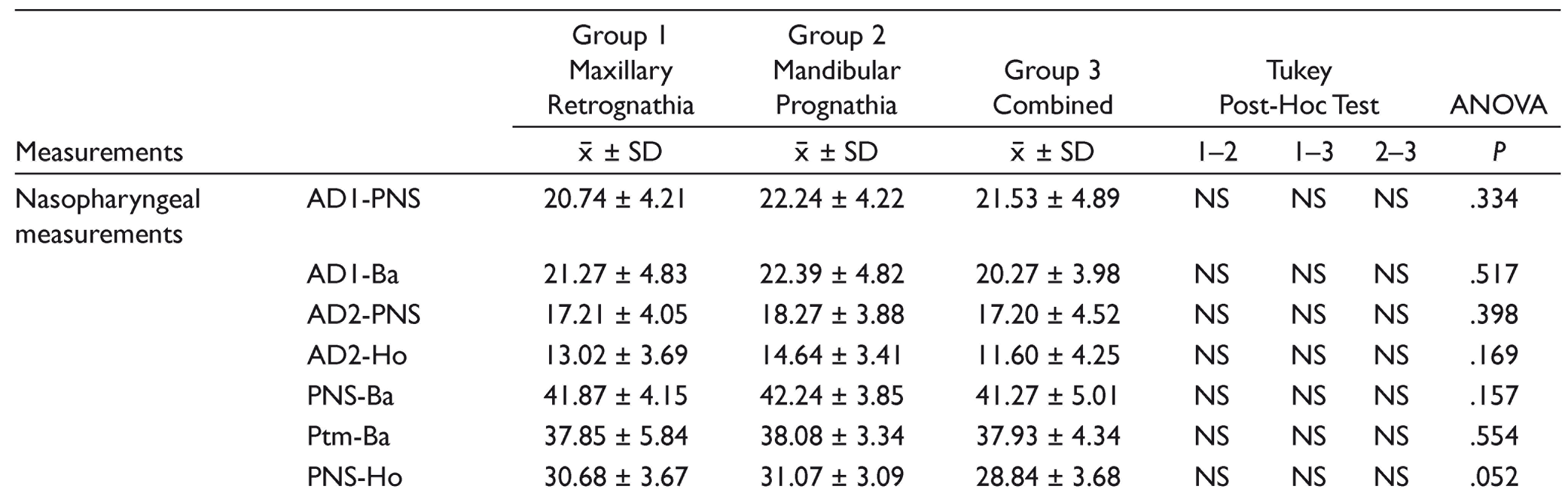
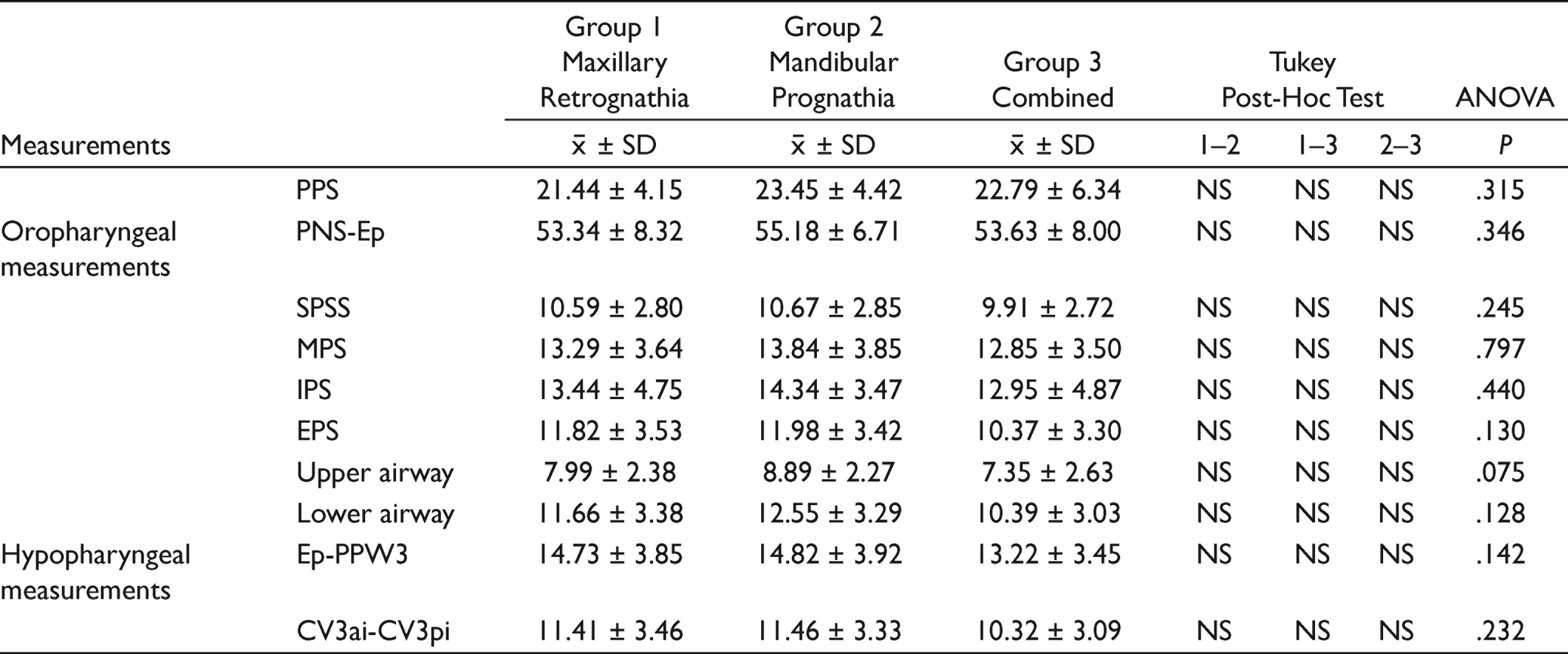
Abbreviations: x-, mean; SD, standard deviation; P, one-way ANOVA test; NS, not-significant P > .0.
Comparison of Hyoid and Area Measurements According to the Subgroups of Skeletal Class III Malocclusion
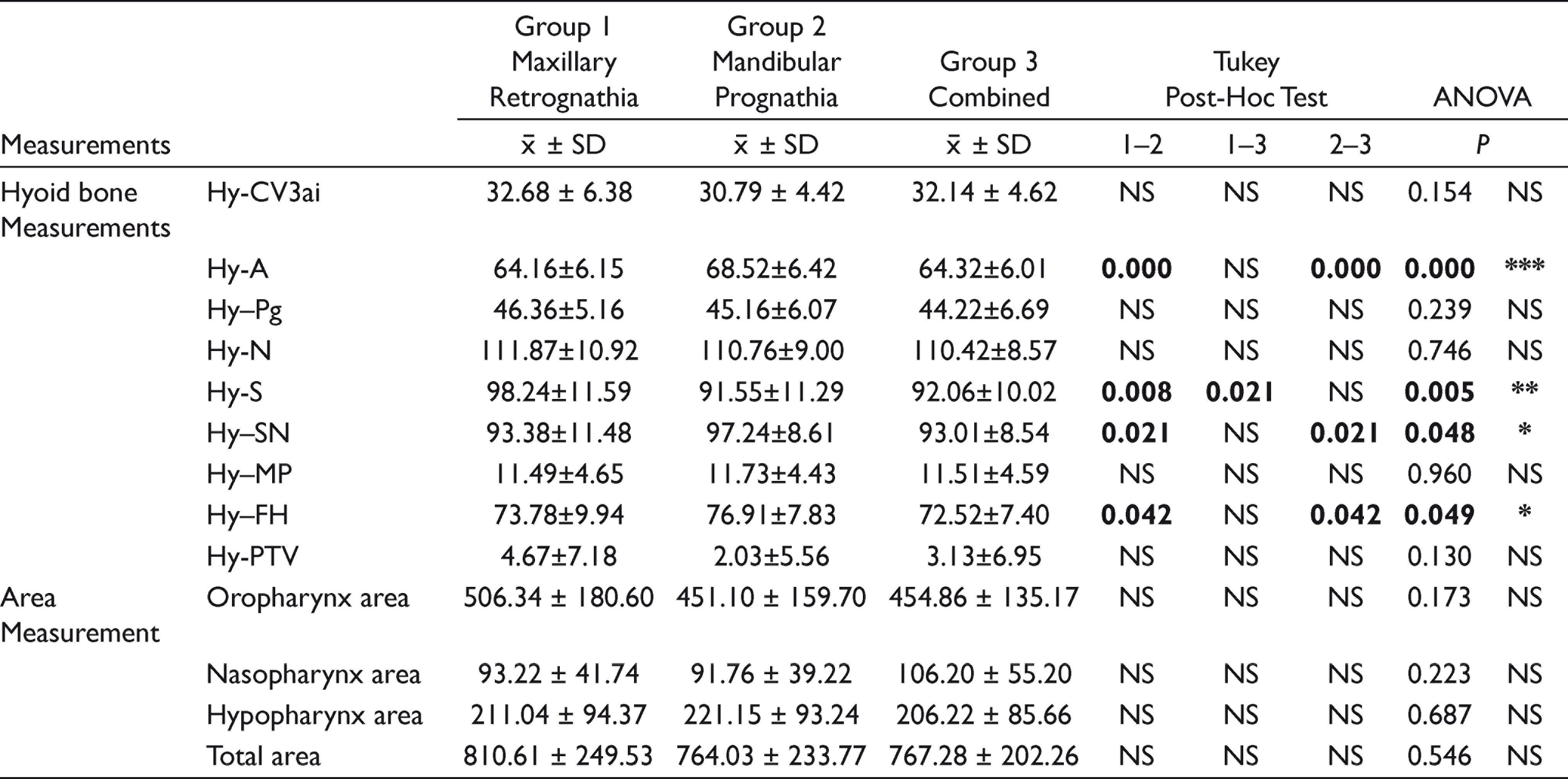
Abbreviations: x- mean; SD, standard deviation; P, one-way ANOVA test; NS, not significant P > .05 *P < .05; **P < .01; ***P < .001.
Discussion
Defining nasopharyngeal characteristics between the subgroups of Class III malocclusion carries an important role in orthodontic treatment planning during patients’ early childhood as well as adolescence, and in assessing the possibility of orthognathic surgery. 19 Although studies in previous years have examined both pharyngeal airway dimensions and the position of the hyoid bone according to different types of malocclusion, only limited studies have evaluated the airway dimensions by dividing them into different groups according to patients’ jaws, from which the condition originates.
Class III anomalies may result from maxillary retrognathia or mandibular prognathia—or a combination of these two conditions. In our study, each group included a similar number of individuals, and the groups did not differ significantly in terms of mean age, and gender. However, the groups’ growth and development periods constituted a statistically significant difference.
Our research is clinically important in terms of planning orthodontic and orthognathic surgeries. Another parameter that orthodontists examine during treatment planning is a patient’s airway because the etiological factor of Class III malocclusions may be an airway obstruction. In addition to orthodontic treatment, long-term treatment outcomes may not need to narrow—or even increase—the airway to reduce recurrence. In orthognathic surgery, the airway and position of the hyoid bone are important references in selecting a surgical procedure in accordance with the amount of motion in a patient’s jaw. Clinicians must evaluate the airway to treat the prognathic mandible because the airway may contract during Class III malocclusions. Similar or different findings regarding airway features in different subtypes of Class III malocclusions are also important for clinicians in determining which treatments to apply. This study’s results observe that airway dimensions were similar for Class III malocclusions in different jaw-borne cases. Considering this finding, since patients’ airway characteristics are similar to patients with mandibular prognathia, the movements of the jaws—especially in the sagittal direction—can be determined accordingly. The results also create a normative value for clinicians.
In the subgroups of Class III malocclusion, the authors observed no differences in pharyngeal airway dimensions or area measurements. The authors observed also differences in hyoid bone position between Class III malocclusions originating from different jaws. Altuğ and Kurt reported that pharyngeal airway dimensions were wider, while soft palate lengths were shorter, in the mandibular prognathia group. 16
The relationships between the maxilla and the mandible’s sagittal, vertical, and transversal positions have a major impact on the pharyngeal airway, and the craniofacial skeletal pattern also affects the upper airway’s dimensions. 17 The literature offers no consensus on how different craniofacial structures affect the airway—although the jaws have a vertical growth pattern, and maxillary retrognathia is often associated with an upper airway obstruction. The available studies’ different results may relate to airway dimensions’ effects on many different conditions. In parallel with this information in the literature, the authors found a narrowing of the upper airway in the maxillary retrognathia group and the widest lower airway in the mandibular prognathia group, although not by a statistically significant amount difference in measurement. Many reasons may account for these findings (age, growth and development period, racial and gender differences, sample size, etc.).
A thesis study in 2017 evaluated hyoid position and stated that the position of the hyoid bone in the maxillary retrognathia group—which is one of the subgroups of Class III malocclusion—was vertically higher than in the mandibular prognathia group. 20 The hyoid bone’s position also relates to the mandible position, to which it is attached by the muscles. For the maxillary retrognathia group, the thesis study reported that the mandible rotates counterclockwise by following the maxilla and that the hyoid bone rotates counterclockwise by following the mandible’s movement. The study also reported that the hyoid bone was positioned higher accordingly. In our study, similar to this thesis study, the author’s found the hyoid bone to be higher in the maxillary retrognathia group.
Fromm and Lundberg compared hyoid bone positions between individuals with mandibular prognathia and individuals with normal occlusion. 21 They observed that the hyoid bone’s position was vertically similar in the groups, and they also found sagitally significant differences between the sexes. In addition, the hyoid bone position was significantly forward in women with mandibular prognathy, and changes in hyoid bone position have been reported to be associated with the mandible’s position.
Sayın reported that the hyoid bone was not associated with any craniofacial features in the sagittal and vertical direction and that it was not affected by the relationships between the maxilla and mandible. 22 He reported that the hyoid bone was positioned above the mandible as the overjet decreased (i.e., Class III malocclusion) and that the hyoid bone was positioned below the mandible as the overjet increased (i.e., Class II malocclusion). Consistent with the authors’ findings, Sayın reported that the Hy-MP distance is affected not by the mandible’s vertical position but by the maxilla’s vertical position, and argued that maxillary posterior rotation elevated the hyoid bone so that it approached the mandible, and with anterior rotation, the hyoid bone underwent posterior rotation relative to the cervical column.
Limitations
Since the current study was retrospectively designed, it could not be standardized in terms of the growth and development period. This lack of standardization can be considered a limitation of this study.
Moreover, the authors did not use cone beam computed tomography in the current study because of reasons such as a high radiation dose, unsuitability for routine use, and the high cost. Thus, the present prospective clinical study’s findings should be assessed within the limitations of two-dimensional radiography design.
Conclusion
Although the authors confirmed their hypothesis in terms of pharyngeal airway dimensions, their findings rejected our hypothesis in terms of hyoid bone position.
Airway dimensions in the nasopharynx are similar among the subgroups of skeletal Class III malocclusion.
Airway dimensions in the oropharynx and hypopharynx were increased in the mandibular prognathia group, but not significantly.
Because of the position of the mandible where the hyoid bone is attached by the muscles, the distance of the hyoid bone from the cranial base (Hy-SN, Hy-FH) is significantly higher in the mandibular prognathia group.
Clinical Significance/Future Scope
The relationship between skeletal Class III malocclusion and pharyngeal dimensions is important as these individuals are strong candidates for possible orthognathic surgery. In addition, determining the pharyngeal characteristics of the subgroups of Class III malocclusion is important in terms of orthodontic treatment planning in early childhood and adolescence, as well as the possibility of orthognathic surgery in the future. For this reason, this study aimed to guide both academicians and clinicians on this subject, which has a limited number of studies in the literature.
With larger sample sizes, this issue will be further clarified, especially in future prospective studies on CBCT.
Footnotes
Acknowledgements
We thank to Dr Hikmet Orhan, for statistical analysis.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.