
Abstract
Malocclusions in the vertical plane are more difficult to treat as compared to the malocclusions in the sagittal plane as they often require multidisciplinary (surgical) approach. Skeletal vertical deficiency and excess causes jaw discrepancies in the sagittal vector too due to rotation of the mandible, thus presenting a complex situation which requires astute treatment planning and implementation. In this article, two cases treated with combined orthodontics and orthognathic surgery to treat skeletal class II malocclusion with vertical deficiency and excess are shown and all details of treatment planning are discussed.
Introduction
Smile is the most recognized expression in the world and is the cornerstone of social interaction. A smile is defined as pleasant when the upper teeth and approximately 1 mm gum tissue are exposed. 1 Gum tissue exposure > 3 mm is generally not considered as attractive. 2 Excessive gingival display or gummy smile, as commonly described, poses an aesthetic problem and makes a person conscious of his/her smile. Insufficient tooth display in low-angle cases (horizontal growth pattern) during smiling also results in poor aesthetics.
Such conditions occur as a result of interplay of several etiological factors 3 such as skeletal vertical maxillary excess/deficiency, incomplete gingival descent (passive eruption), hypermobility of the upper lip, short upper lip, and excessive horizontal or vertical growth pattern. Therefore, it is essential to analyze several aspects, such as symmetry of lips and face during smile, level of the gingival margins, smile line, skeletal proportions, to arrive at an accurate treatment plan.
In vertical maxillary excess, clinically recognizable smile features are manifested by a gummy smile, complete exposure of the maxillary incisors at rest, incompetent lips, increased lower facial height, and high mandibular plane angle. The surgical orthodontic correction of vertical maxillary excess by superior repositioning of the maxilla is generally an accepted treatment plan based on skeletal stability and aesthetic soft-tissue changes.4, 5
In severe horizontally growing cases, especially class II division 2 malocclusions, reduced lower anterior facial height, insufficient incisor display, deep bite, and a retruded mandible with a backward path of closure is seen. In adults, such cases need to be managed by advancing the mandible sagittally and vertically either with a fixed functional appliance or surgically, depending on the severity of the problem.6, 7
Significant jaw discrepancies render people less attractive leading to their nonacceptance socially. 8 This case report describes the combined orthodontic and surgical approach in the treatment of two skeletal class II cases with different growth patterns.
Case Report 1
A female patient aged 18 years presented with a chief complaint of irregularly placed lower and upper front teeth.
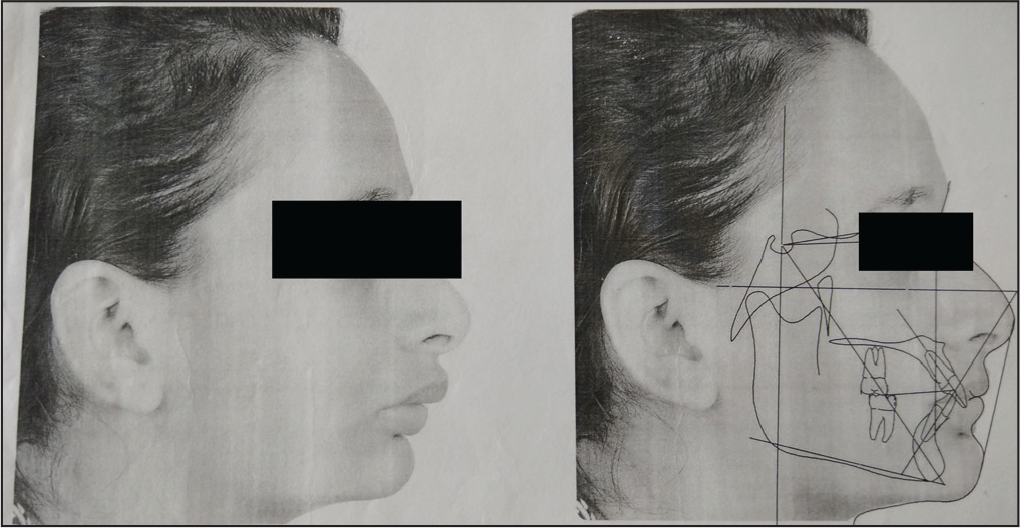
Extraoral examination (Figure 1) shows a convex soft tissue profile, deep mentolabial sulcus, reduced anterior lower facial height, non-consonant smile arc, reduced incisor display on smiling, competent lips, and everted lower lip. Visual treatment objective was positive.
Pretreatment Extraoral

Intraoral examination (Figure 2) shows Angle class II molar relation with division 2 incisor relation and class II canine relation bilaterally, 100% deep overbite. The lower midline is shifted toward the left side by 2 mm and severe crowding in the lower arch with lingually locked lower right canine and lower right lateral incisor. Patient has a large freeway space suggesting true deep bite due to infraocclusion of the molars. Upper arch is “v” shaped and the lower arch is “u” shaped.
Pretreatment Intraoral

Orthopantomogram (Figure 3) shows all the permanent teeth have erupted and all the third molars are present.
Pretreatment Orthopantomogram

Pretreatment Extraoral

Cephalometric Analysis (Case Report 1)
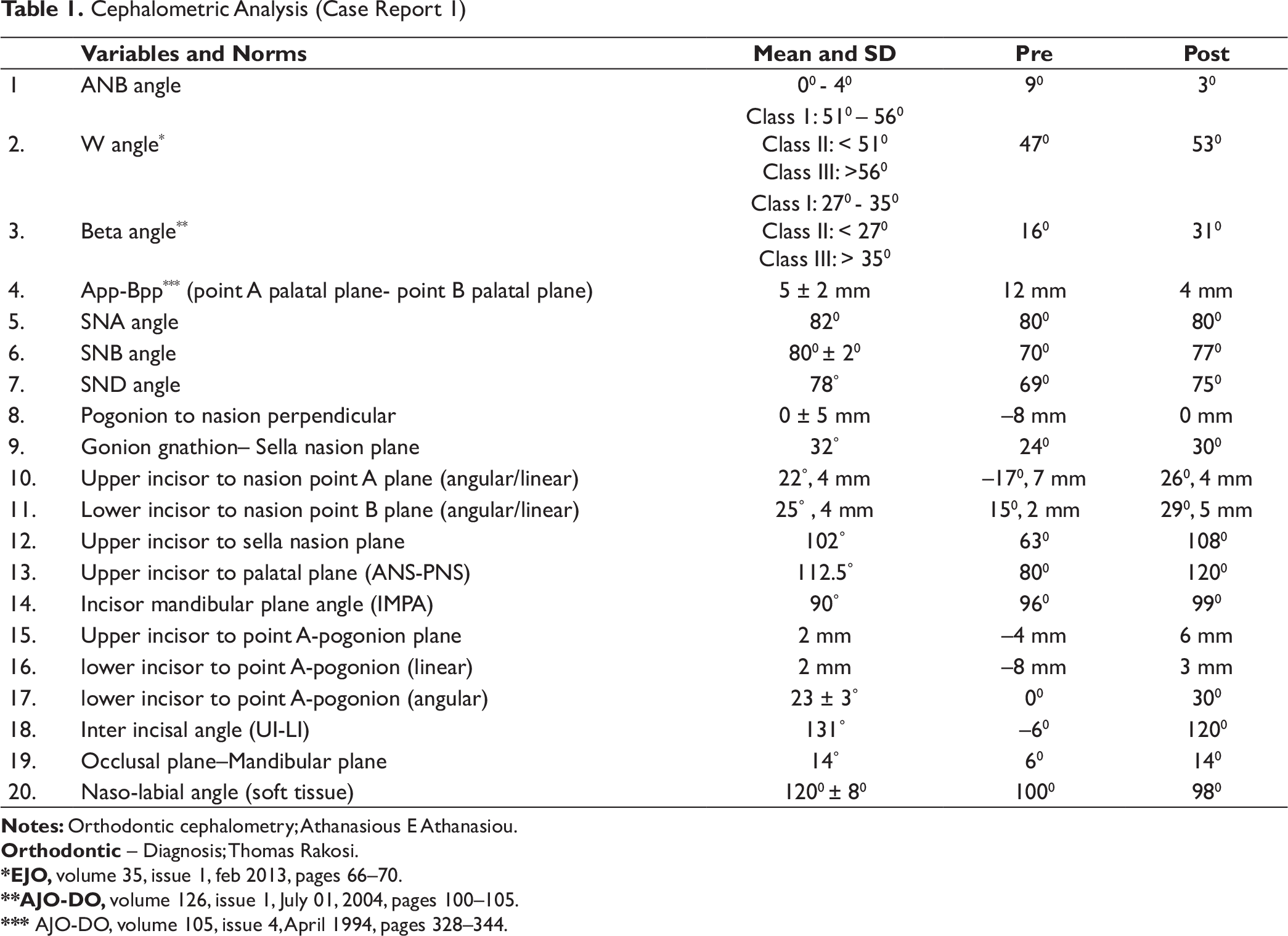
Orthodontic – Diagnosis; Thomas Rakosi.
*EJO, volume 35, issue 1, feb 2013, pages 66–70.
**AJO-DO, volume 126, issue 1, July 01, 2004, pages 100–105.
*** AJO-DO, volume 105, issue 4, April 1994, pages 328–344.
Model Analysis
Carey analysis reveals a severe tooth size–arch length discrepancy in the lower arch. Bolton analysis confirms lower anterior and overall tooth material excess. Index of Orthodontic Treatment Need suggests a definite need for orthodontic treatment.
The case was diagnosed as a class II division 2 malocclusion superimposed over a skeletal class 2 base due to retrognathic mandible with a horizontal growth pattern.
Problem List
Retroclined upper incisors, traumatic bite, and severe crowding in the lower anterior segment
Class II molar and canine relationship bilaterally
100% deep overbite
Class II maxilla–mandibular relation with severe retrognathia of the mandible
Reduced lower anterior facial height and a convex profile
Deep mentolabial sulcus and a non-consonant smile arc
Reduced incisal display on smile with wide buccal corridors
Treatment Objectives
To align the upper and lower anterior teeth and correct the overjet.
To achieve a class 1 canine and molar relationship.
To treat the skeletal deep bite and achieve an ideal vertical overlap of the incisors.
To correct the deep mentolabial sulcus, reduce the lower lip eversion, and increase the lower anterior facial height and achieve ideal facial proportions.
To correct the sagittal maxillomandibular discrepancy and vertical jaw deficiency by advancing the mandible in a sagittal and vertical direction.
To improve the tooth–lip relationship and achieve smile arc consonancy.
Treatment Options
Option 1
Alignment of the upper and lower incisors followed by correction of the overjet and overbite by surgical advancement of the lower jaw.
This treatment option would be able to achieve all the treatment objectives.
Option 2
Alignment of the incisors followed by nonsurgical advancement of the lower jaw with a hybrid fixed functional appliance.
The above treatment option would lead to skeletal changes in prepubertal patients. Postpubertal patients, such as the above described case, would not have significant skeletal changes. 9 In addition, deficient lower anterior facial height cannot be corrected satisfactorily with this option.
Option 3
Alignment of the incisors followed by correction of overjet and overbite by either upper premolar extraction or en-mass maxillary arch distalization using infrazygomatic screw OrthoBoneScrew) microimplants.
The above treatment option would not solve the mandibular retrognathia and deficient lower facial height.
The treatment option 1 was selected.
Treatment Plan and Sequence
Before starting the treatment, a visual treatment objective (Figure 5) was done by advancing the lower jaw to evaluate the best possible position of the lower incisor in accordance with the new mandibular position. Accordingly, it was decided to only align the upper incisors and extract the lower lateral incisors to relieve the crowding and upright the lower incisors.
Visual Treatment Objective
Bonding was done with a 022 MBT bracket system. The upper arch was bonded first and alignment was done with a wire progression of 014 NiTi, 016 NiTi, 016 × 022 NiTi, 017 × 025 NiTi, 017 × 025 SS, 019 × 025 SS.
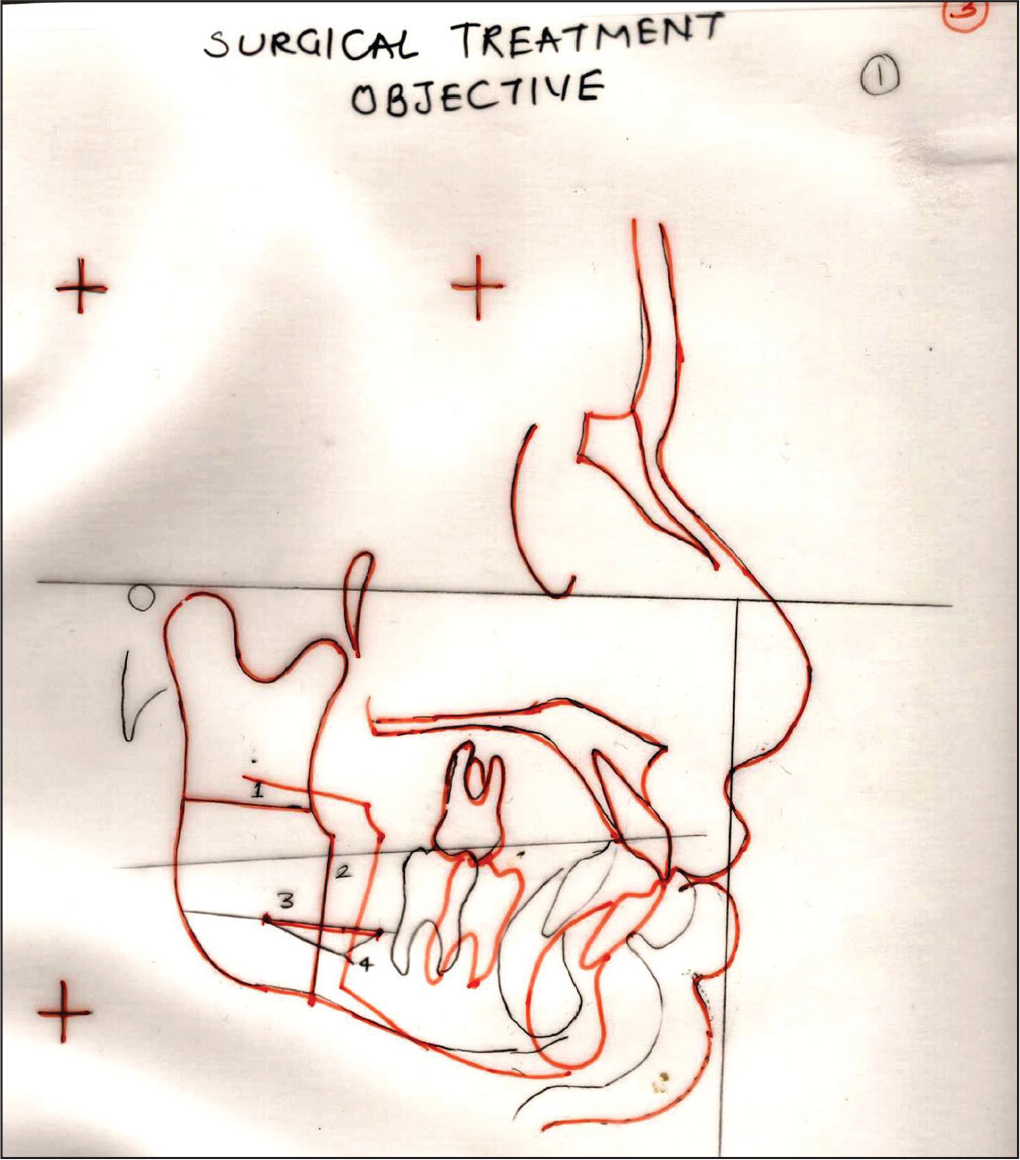
Lower strap-up was done as soon as the bite interference got relieved and a similar wire progression was done. Lower lateral incisor was extracted. The lower curve of Spee was maintained to be leveled postsurgically. All the presurgical dental objectives were achieved in 12 months (Figure 6). Surgical treatment objective (Figure 7) was done and a 9-mm mandibular advancement was planned.
Presurgical Intraoral

Surgical Treatment Objective
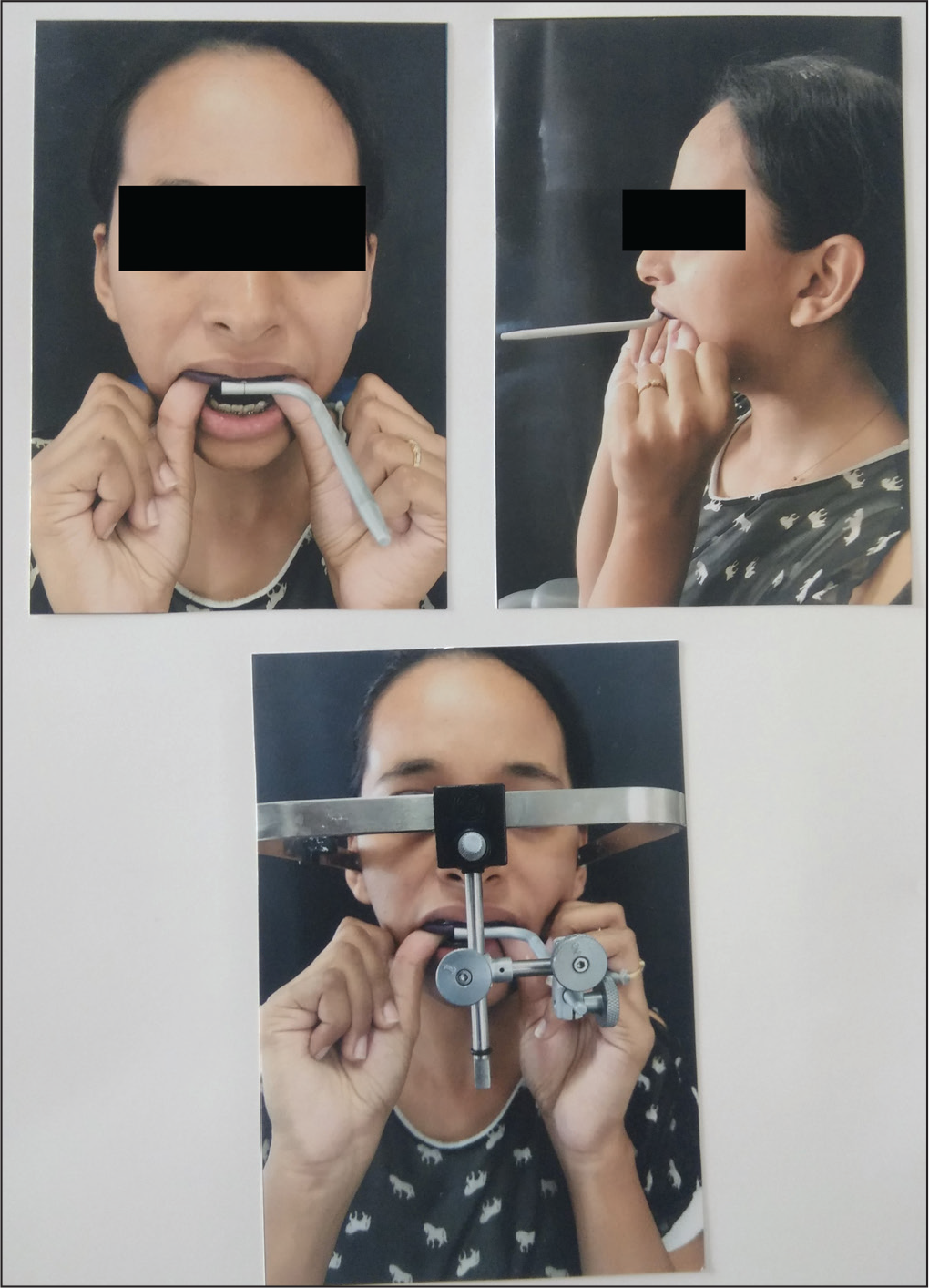
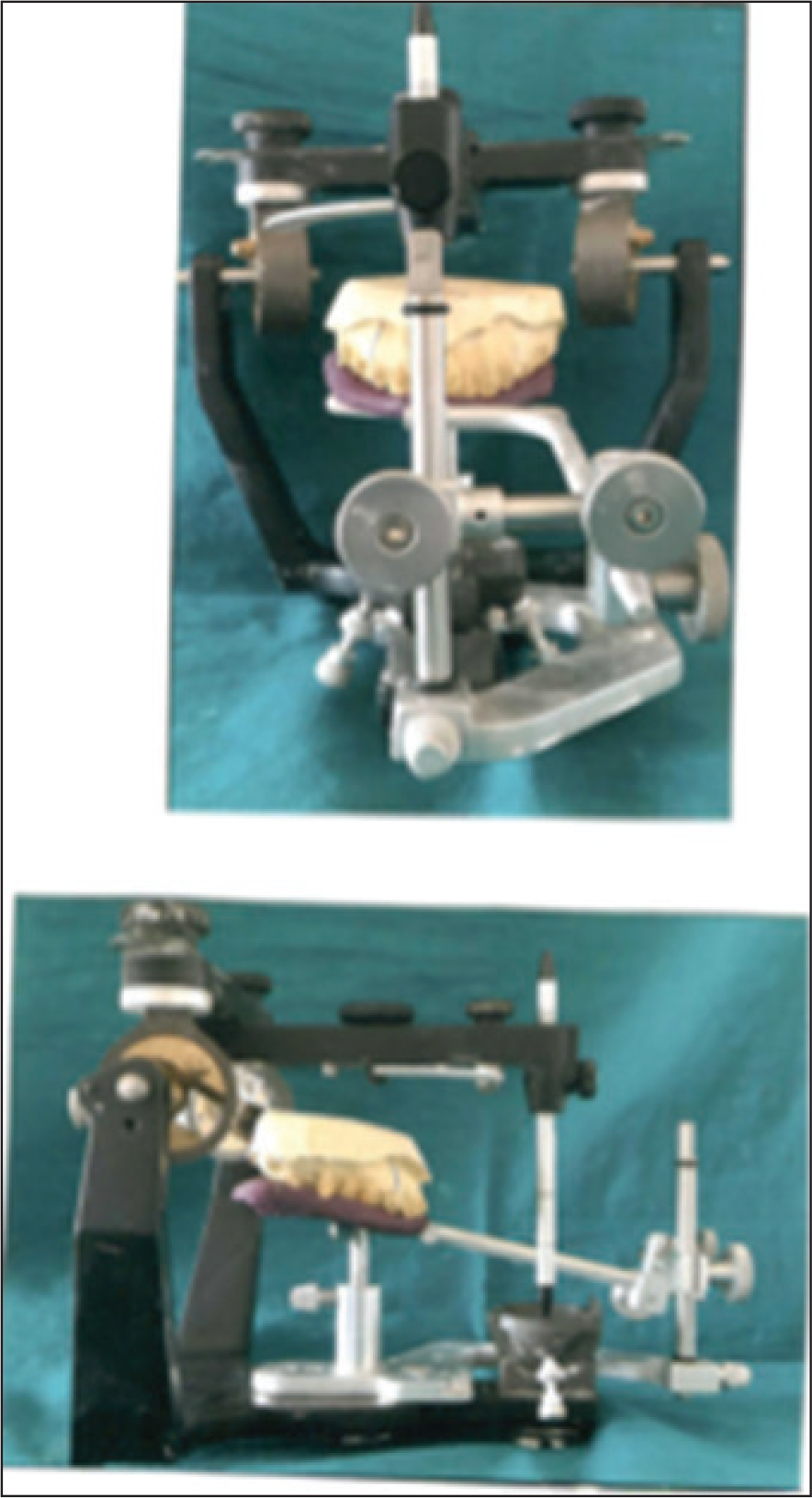
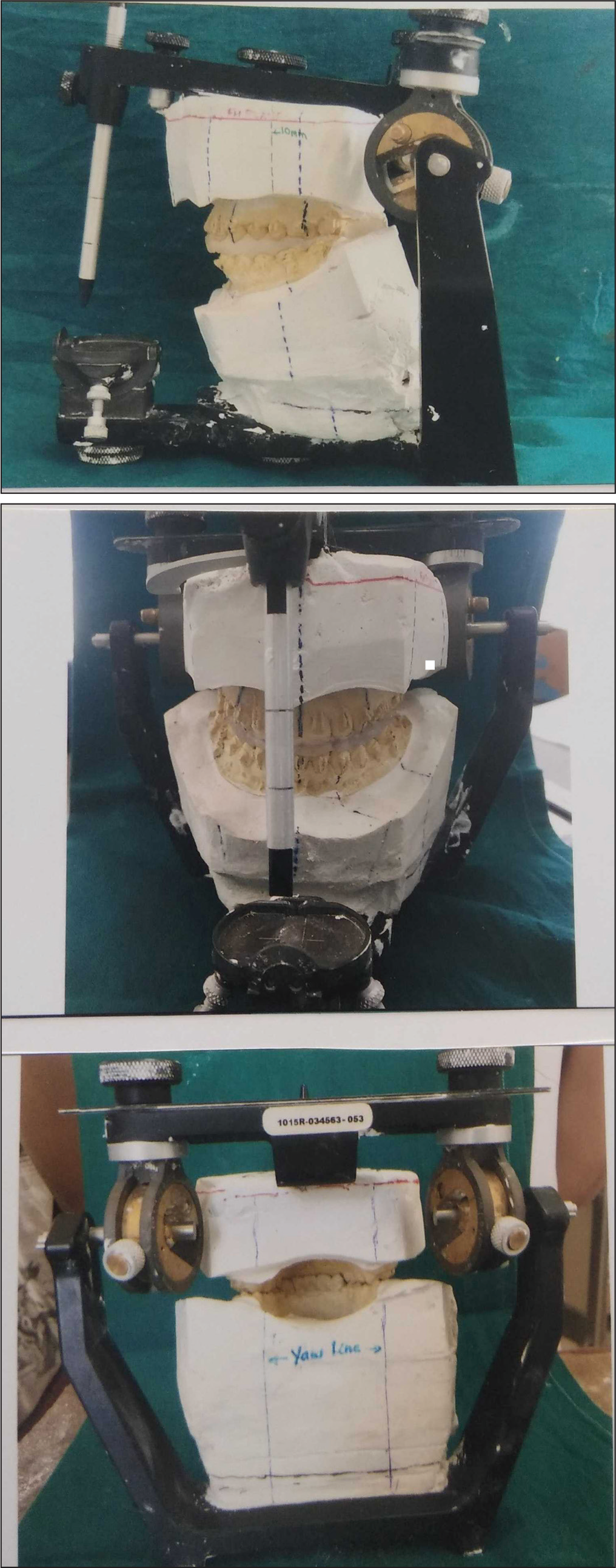
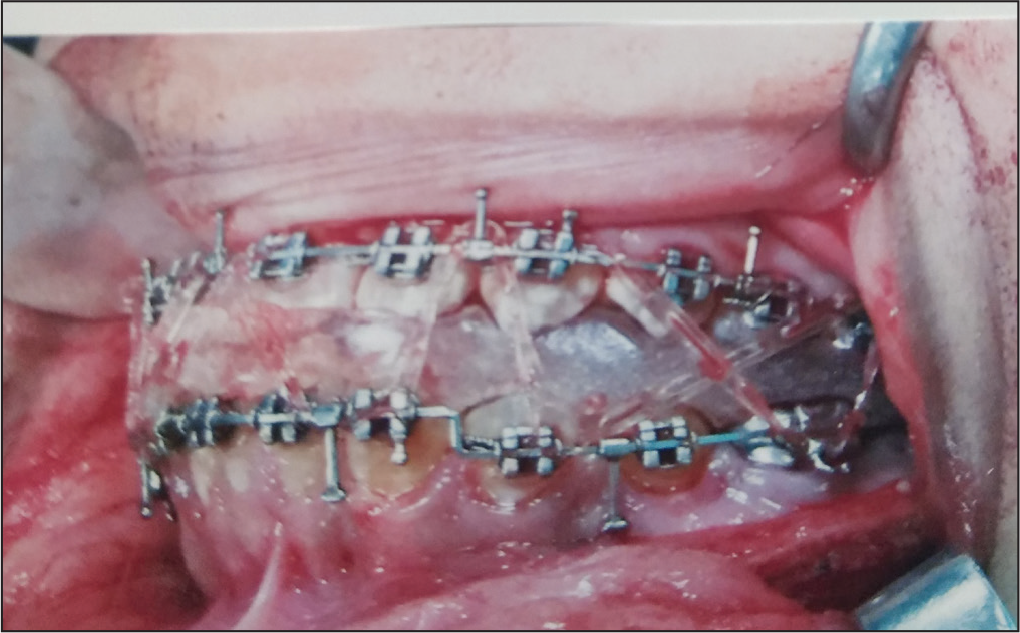
To orient the maxillary cast along the patient’s cranial base a face bow transfer (Figure 8) was done and models were mounted on a semi-adjustable Hanau articulator (Figure 9). Mock surgery was done and the mandible advanced downward and forward by 9 mm. There was an open bite in the premolar region to be closed by extrusion of the premolars postsurgically. A surgical splint was fabricated to guide the surgeon during surgery to accurately position the mandible according to the plan (Figures 10 and 11).
Face Bow Transfer
Articulator Mounting
Mock Surgery
Intraoperative Splint Fixation
Postsurgical lateral open bite (Figure 12) was closed by extrusion of the premolars and molars. Occlusal interdigitation was achieved in 7 weeks. Upper and lower fixed retainers were fixed and brackets were removed. Posttreatment records were taken.
Immediate Postsurgical Cephalogram

Results Achieved
After treatment, the upper and lower arches were well aligned, unilateral (right side) class I molar and canine relation was achieved, and an end-on canine and super class I molar relationship on the left side was achieved.
Ideal overjet and overbite was also achieved (Figure 13).
An aesthetic straight profile was achieved with a significant increase in the lower anterior facial height (Figure 14).
Optimum smile aesthetics was achieved with smile consonance and a much-improved incisor display on smiling.
The posttreatment cephalogram (Figure 15) shows a much-improved sagittal and vertical correction of the lower jaw. Cephalometric analysis (Table 1) confirms the class 1 jaw relationship and a significant change in the lower anterior facial height.
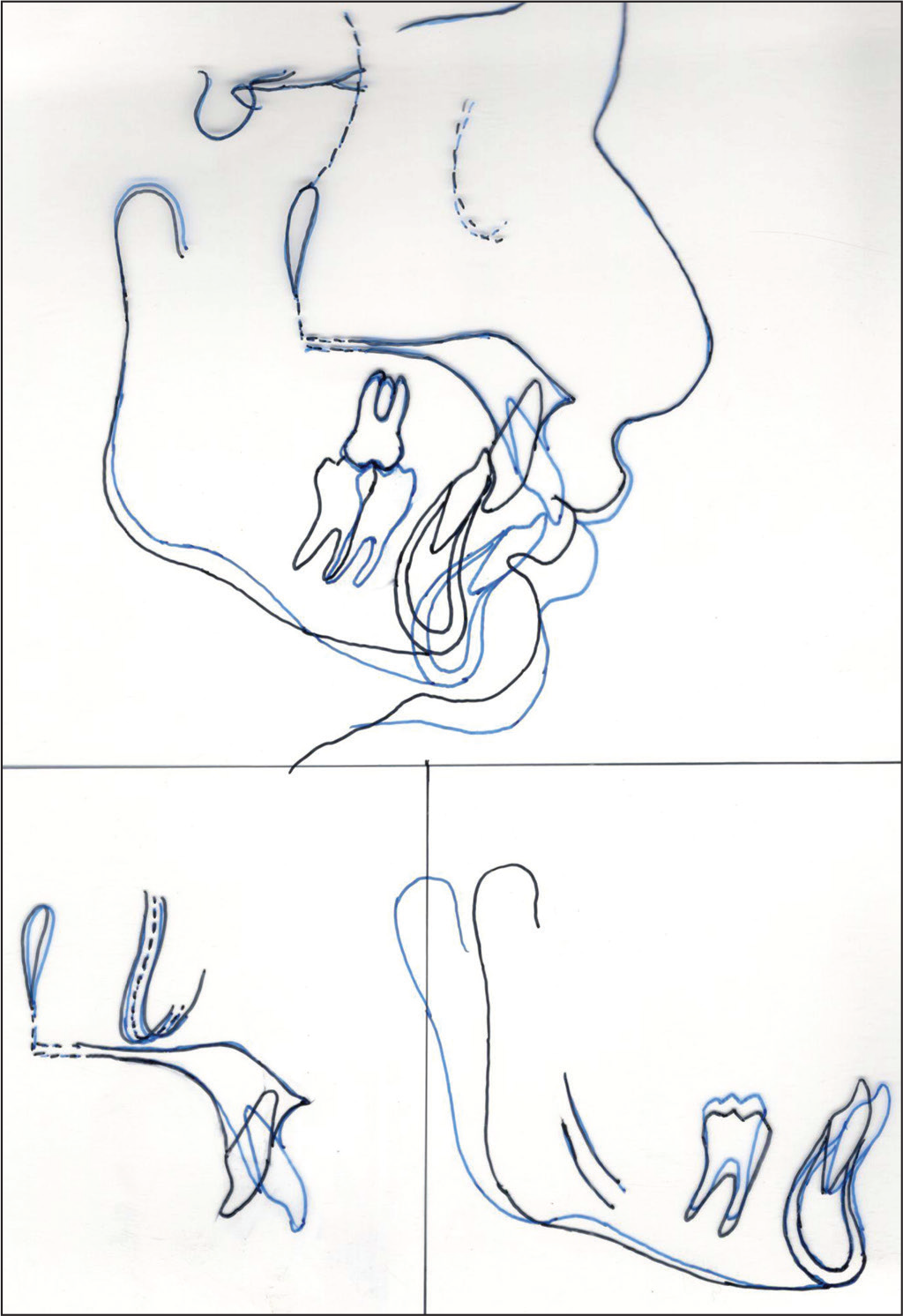
Cephalometric superimposition of pre- and posttreatment cephalograms clearly displays the treatment changes brought about by the treatment (Figure 16).
Posttreatment Intraoral

Posttreatment Extraoral

Posttreatment Cephalogram

Cephalometric Superimposition
Critical Appraisal
Maxillary position was normal in the above case with severely retrognathic mandible. In addition to sagittal discrepancy, the mandible was deficient in the vertical vector too. Since the patient was beyond the age of favorable growth modification, a surgical treatment option was considered.
The patient had a horizontal growth pattern and therefore a wide symphysis, 10 thus the lower incisor roots could be placed within the cancellous bone by the extraction of the lingually placed lower lateral incisor alone. Post treatment class I occlusion was achieved on the right side. A class I molar and canine relation was not possible on the left side but a cusp fossa and cusp embrasure relationship was achieved.
The upper midline was matching with the midline of the face. The lower incisor roots were in the center of the cancellous bone post treatment. Extraction of the lower incisors to correct dental crowding and proclination has been shown to be an effective and stable procedure. 11
Retention Plan
Upper and lower fixed flexible spiral wire permanent retainers were placed to prevent relapse of the crowding. A removable Hawley appliance was given for night time wear.
Case Report 2
A male patient 25 years of age presented to the department of orthodontics with a complaint of prominent front teeth and excessive gum display on smiling.
On extraoral examination (Figure 17), a leptoprosopic face with incompetent lips and an interlabial gap of 5 mm at rest were seen. Lower lip was everted with hyperactive mentalis muscle activity. There was excessive gum display on smiling (5 mm). Patient had a convex profile and a deep mentolabial sulcus. The lower anterior facial height was increased.
Pretreatment Photographs
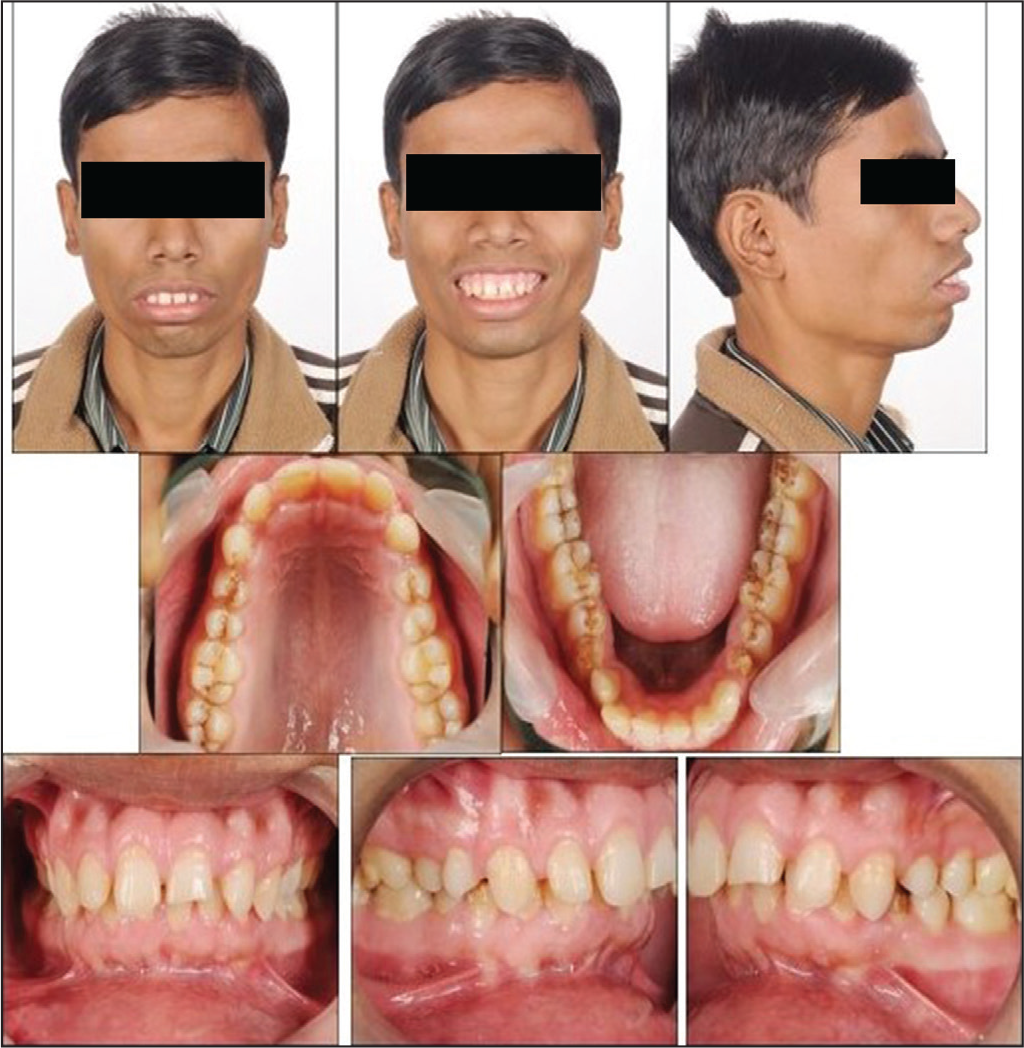
Intraoral examination showed a class 1 molar and end-on canine relationship. Patient had moderate spacing between the upper incisors. The lower incisors were flared labially. There was a 7-mm overjet and 8 mm of overbite present. The lower midline was shifted toward the right.
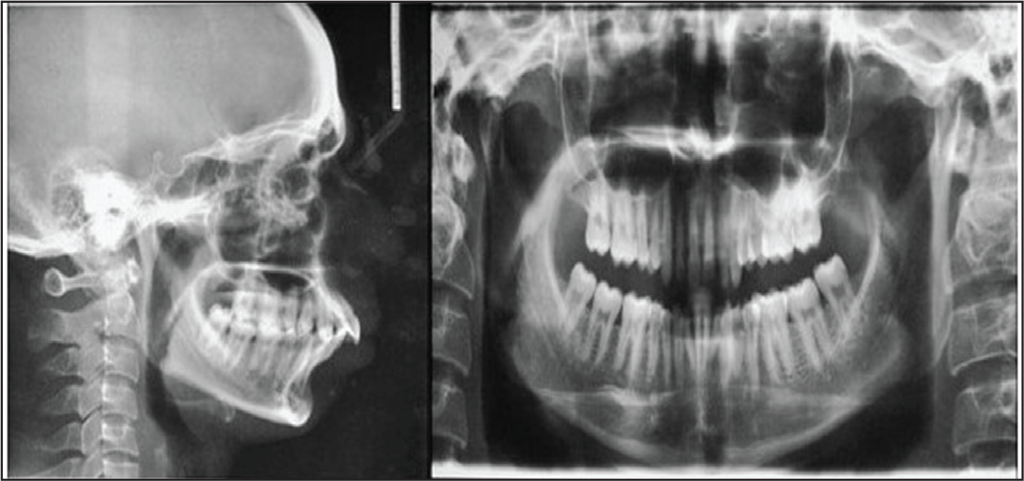
Panoramic X-ray (Figure 18) showed the absence of maxillary third molars and the mandibular third molars had completely erupted in the oral cavity.
Pretreatment Radiographs
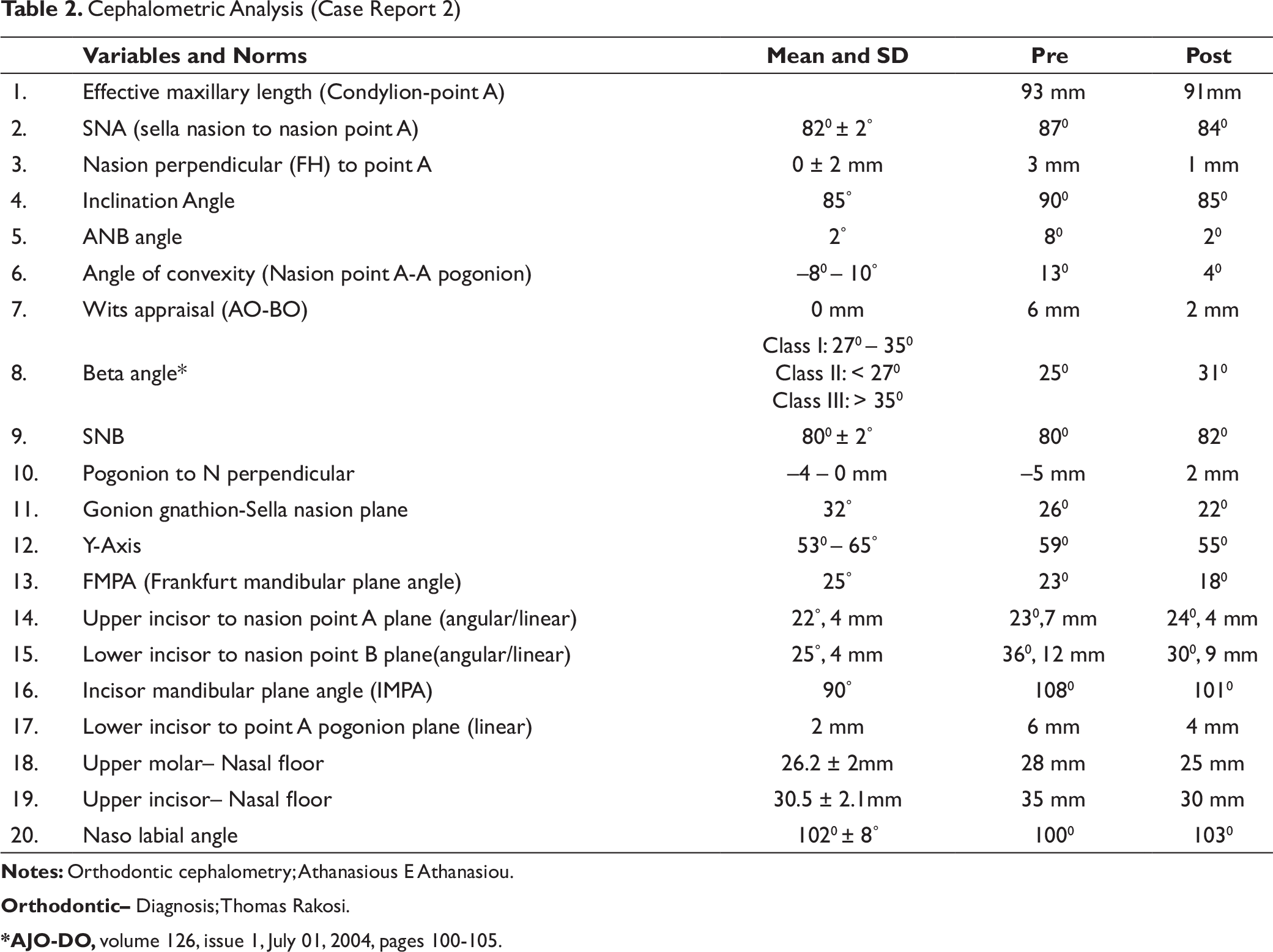
Cephalometric Analysis (Case Report 2)
Orthodontic– Diagnosis; Thomas Rakosi.
*AJO-DO, volume 126, issue 1, July 01, 2004, pages 100-105.
The case was diagnosed as skeletal class 2 base with sagittal and vertical maxillary excess with forwardly placed upper incisors and flared lower incisors.
Problem List
Excessive display of upper incisors at rest with excessive overall gingival display on smiling
Increased overjet with deep overbite and spacing between the upper and lower incisors
Increased lower anterior facial height and increased interlabial gap at rest. Hypotonic upper lips with everted lower lips and hyperactive mentalis activity
A class 2 skeletal base with maxillary vertical excess resulting in clockwise rotation of the mandible resulting in deficient chin
Treatment Objectives
To close the dental spacing between the upper and lower incisors.
To correct the dental midlines and position the lower incisors upright over the basal bone. Achieve class I molar and canine relation, and provide a stable cusp fossa and cusp embrasure occlusion.
To reduce the interlabial gap at rest and achieve lip competence.
To reduce the incisal exposure at rest and reduce the gum display on smiling.
To correct the class 2 skeletal base and improve the chin prominence.
To provide an aesthetic and pleasing soft tissue profile.
Treatment Options
Option 1
Surgical impaction of the maxilla and setback causing counterclockwise autorotation of the mandible, followed by chin augmentation by advancement genioplasty.
This option would correct the vertical maxillary excess. Autorotation of the mandible with chin advancement will correct the chin deficiency.
Option 2
It involved maxillary dentoalveolar intrusion with temporary anchorage devices. Literature suggested that the mean absolute intrusion of the incisors of 2.1 mm is possible with the help of temporary anchorage devices. 12 Patient had severe vertical excess in relation to incisors and molars Table 2) which might not be corrected entirely with the help of temporary anchorage devices.
Option 1 was selected as it would predictably solve all the patients’ problems.
Treatment Plan and Progress
Visual treatment objective was done. It was clear that impaction and setback of the maxilla would cause the mandibular autorotation and there was improvement in the patient’s profile. Further chin augmentation was planned by advancement genioplasty. The lower incisors were to be retracted and kept upright on the basal bone to allow for the mandibular autorotation.
A 022 MBT strap-up was done. Wires were progressed to level and align the dental arches. All the upper anterior spaces were closed and an extra labial root torque was added in the anterior segment of the lower arch wire to upright the lower incisors. 4-mm overjet was maintained to setback the maxilla. After 16 months, the presurgical objectives were achieved (Figure 19). Surgical treatment objective was done (Figure 20), face bow transfer was performed, and the casts transferred to an articulator. Mock surgery was performed and as determined in the surgical treatment objective, the maxillary cast was impacted 5 mm anteriorly and 3.5 mm posteriorly. Autorotation of the mandibular cast followed. A class I molar and canine relation was achieved. A surgical splint was fabricated with cold cure acrylic.
Mid-Stage Photographs

Surgical Treatment Objective
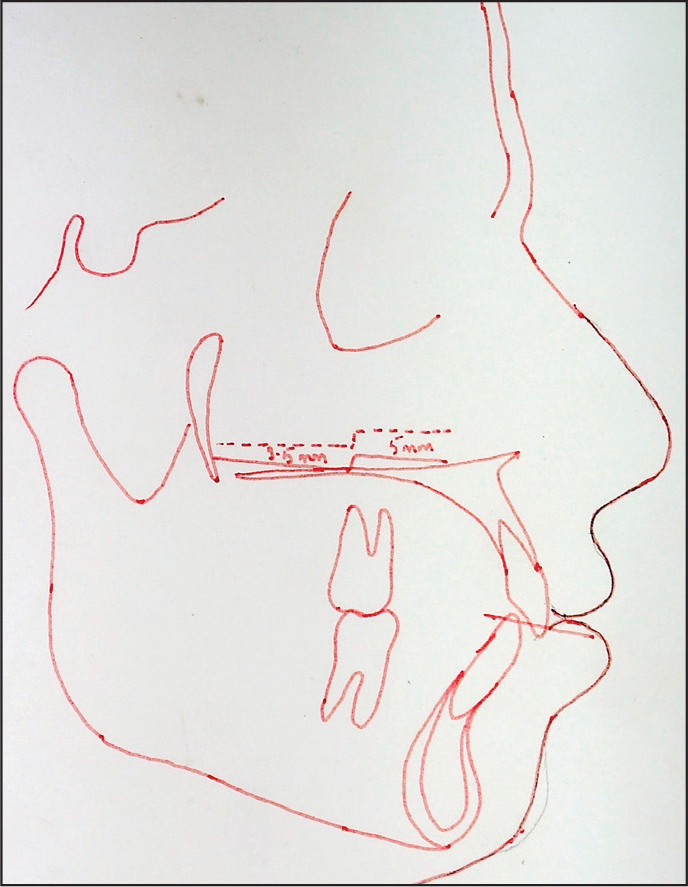
A LeFort 1 osteotomy of the maxilla was done to impact and set back the maxilla followed by the autorotation of the mandible as predicted in the surgical treatment objective. 5-mm maxillary superior impaction in the anterior region and 3.5-mm impaction in the posterior region was done.
An advancement genioplasty was done in order to improve the chin deficiency. Surgery was performed as planned without any complications. Correction was maintained by rigid fixation. Post the surgery, the patient recovered well and was pleased with his new appearance. After 10 months of postsurgical finishing and detailing, the brackets were removed and fixed upper and lower lingual retainers were placed to prevent opening of the anterior interdental spaces. The total treatment time was 26 months.
Treatment Results
All dental spacings were closed. Canines and molars were in class I relation. Ideal overjet and overbite was achieved (Figure 21).
Vertical maxillary excess was corrected. Excessive incisal and gingival display at rest and on smiling was corrected. Smile arc consonance was achieved.
Chin deficiency was corrected and good chin prominence was achieved.
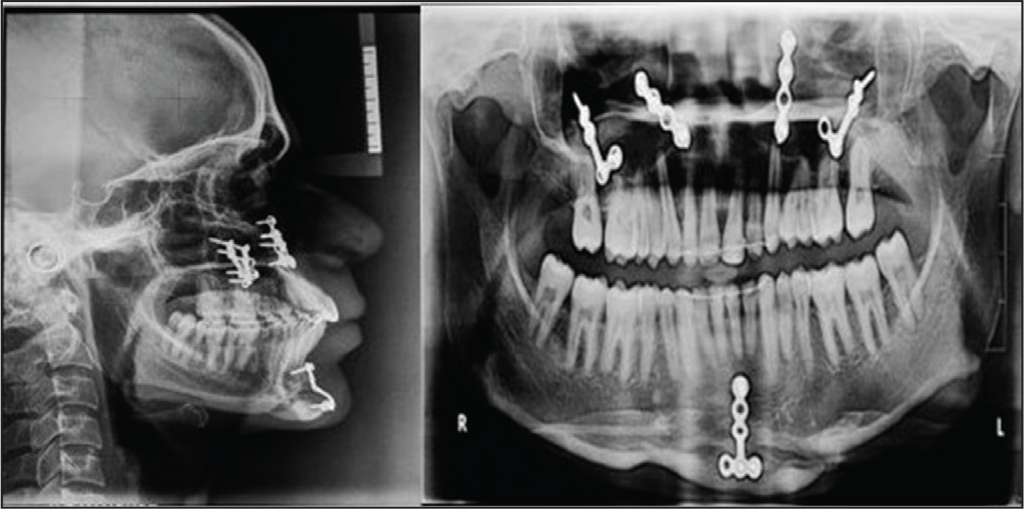
Posttreatment cephalogram (Figure 22) shows the correction of the vertical and anteroposterior jaw discrepancy by the setback of the maxilla and the forward rotation of the mandible.
Posttreatment facial proportions and aesthetics were good and all the treatment objectives were achieved.
Posttreatment Photographs

Posttreatment Radiographs
Critical Appraisal
In many patients, with maxillomandibular deformity, disproportionate growth of the maxilla causes long facial appearance that is known as vertical maxillary excess. The deformity presents most often in the vertical dimension, with or without anteroposterior or transverse discrepancy.
Excessive gingival display is regarded as the hallmark of this deformity that is not related to altered passive eruption, short clinical crown of upper anterior teeth, hyperactivity, or short upper lip. 13 Its correction requires a well-planned and orchestrated orthodontic preparation followed by orthognathic surgery.
Cephalometric superimposition (Figure 23) clearly demonstrates the impaction and setback of the maxilla which has resulted in the counterclockwise rotation of the mandible, the magnitude of which is predicted as a proportion of superior impaction. 14
Cephalometric Superimposition
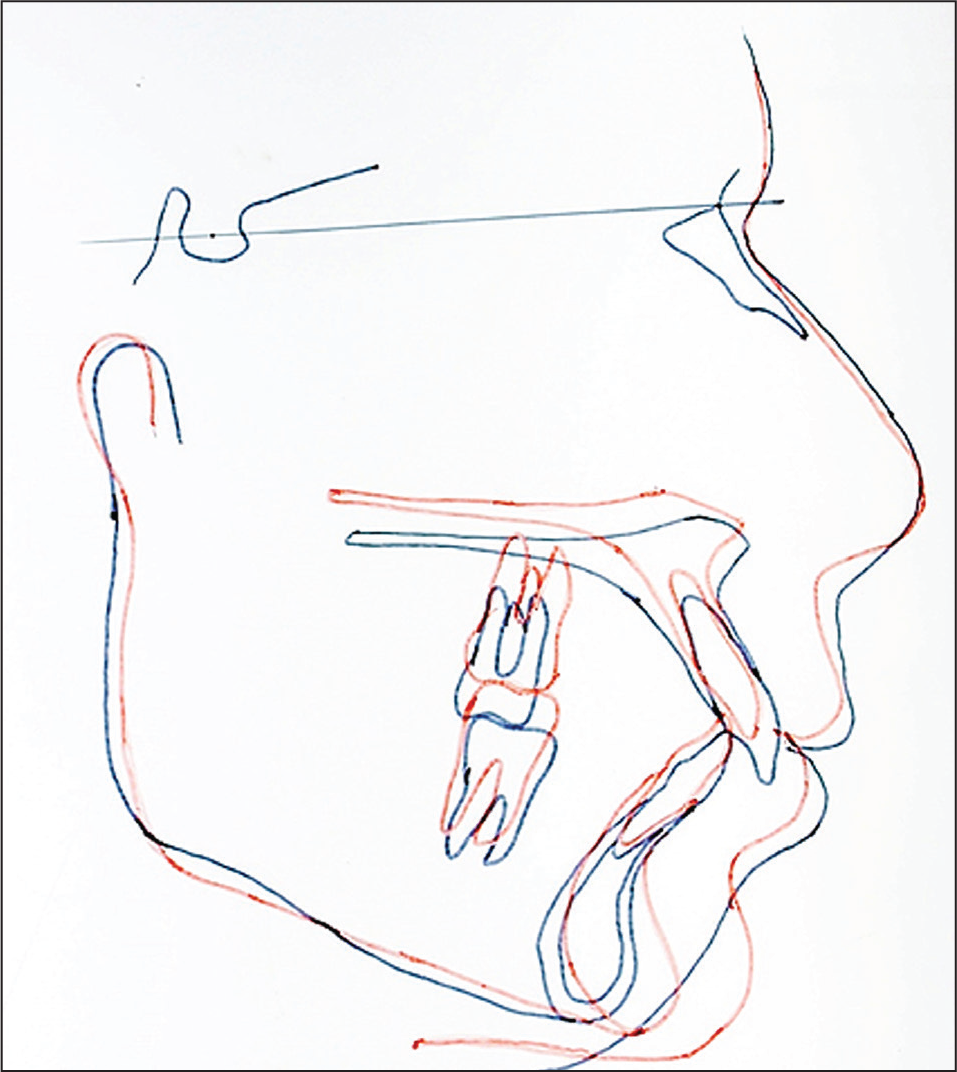
In the above case, the mandible was appropriately related to the maxilla and therefore, mandibular surgery was unnecessary.
Small discrepancy between the actual and ideal position of the mandible was correctable by small movements of the maxilla in anteroposterior or vertical planes to accommodate the position of the autorotated mandible. Thus in accordance with literature, the above procedure has proved to be a useful surgical method for adult patients with little or no remaining growth potential. 15
The impaction of the maxilla in the above case was facilitated by partial resection of the nasal septum and palatal septal crest to prevent buckling and nasal deviation to prevent any subsequent airway problems. The preservation of the nasal spine contributed significantly in the preservation of flaring of the nose, which was augmented by the application of alar cinch sutures. The mobilized maxilla was fixed in its telescopic position with flush contact at piriform region and the zygomaticomaxillary junction in accordance with the preplanned position.
Patient had a convex profile with hyperactive mentalis muscle; therefore, chin augmentation surgery was performed after repositioning of the maxilla and mandible. One of the advantages of augmentation of the chin via inferior border osteotomy is that the ratio of soft tissue to hard tissue change is quite predictable. 16 The advancement of the chin in the above case resulted in tremendous improvement in the profile and reduced mentalis muscle hyperactivity.
Summary
Mandibular advancement by bilateral sagittal split osteotomy in the above case is a stable procedure 17 to treat adult patients having severe skeletal class 2 malocclusions with deep bite. The resulting facial aesthetic changes are satisfactory.
Vertical repositioning of the maxilla has proven to be one of the most stable orthognathic surgeries, and with its increased stability, it offers a significant benefit particularly for long-faced patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no receipt of financial support for the research, authorship, and/or publication of this article.