
Abstract
Abstract
This case report was adjudged one of the best-treated cases displayed in the Indian Board of Orthodontics after the board certification process. The summary of the treatment and various records are reprinted here with minimal editing and reformatting so that the presentation resembles the actual documents submitted to the board.
Keywords
Introduction
Severe bi-jaw discrepancies can now be predictably treated by orthognathic surgery. The use of orthodontic microimplants, also known as miniscrews, mini-implants, and temporary anchorage devices (TADs), and their range of applications in dentoalveolar structures have undergone a paradigm shift since their introduction almost two decades ago. 1 The adjunctive use of TADs has been documented to improve the biomechanical effectiveness three-dimensionally, 2 when intrusion and torque control of the maxillary anteriors were attempted with conventional fixed mechanotherapy. Their versatile applications in the correction of complex vertical skeletal discrepancies have been reported.3-6 Following an alert diagnosis of the nature and severity of the orthodontic problem, it is essential to determine the parameters of tooth movement and the mode of orthodontic intervention that will be necessary to accomplish it. This case report provides an insight into contemporary management strategies, wherein the biomechanical advantage provided by TADs was utilized to expand the scope and range of orthodontic tooth movement in an adult patient with a Class II skeletal discrepancy involving both the jaws.
Case Report
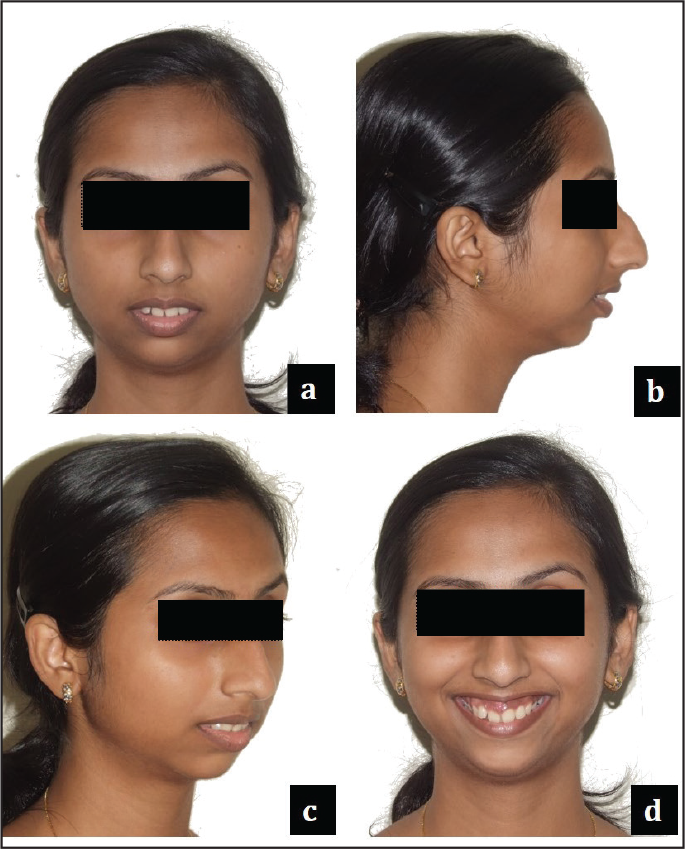
MS, a 21-year 8-month-old adult female, presented with skeletal Class II malocclusion having marked retrognathism of the mandible and vertical maxillary excess (VME). End-on molar and canine relation on right and left sides with crowding in relation to both upper and lower anteriors was observed. The incisor relationship was toward Class II. She had an obtuse nasolabial angle with a prominent dorsal hump. There was excessive display of incisors at rest, with 7 mm of gingival exposure during smile. Her clinical lower anterior facial height was significantly reduced. Based on the extent of her skeletal malocclusion, it was decided to address her anteroposterior skeletal discrepancy with surgical orthodontics. As the excessive incisor display was more due to the dentoalveolar component, it was decided to camouflage her vertical excess with skeletal anchorage, primarily aimed at intrusion mechanics. After presurgical orthodontics, bilateral sagittal split osteotomy (BSSO) with mandibular advancement and augmentation genioplasty was performed. At the end of postsurgical orthodontics, the ideal anteroposterior relation was established along with a Class I molar, incisor, canine relationship and ideal overjet and overbite. Gingival microesthetics were addressed, and the overall facial esthetics were significantly improved. The retention protocol involved upper and lower wrap around retainers and bonded lingual retainers.
Section 1. Pretreatment Assessment Details
Initials: MS
Sex: Female
Date of birth: May 4, 1990
Age at start of treatment: 21 years 8 months
Patient’s complaint: “Excessive show of gums on smile and irregularly arranged upper front teeth.”
Relevant medical history: Her medical history revealed her to be asthmatic. She had a history of nocturnal mouth breathing and snoring.
Clinical Examination: Extraoral Features
Skeletal Assessment
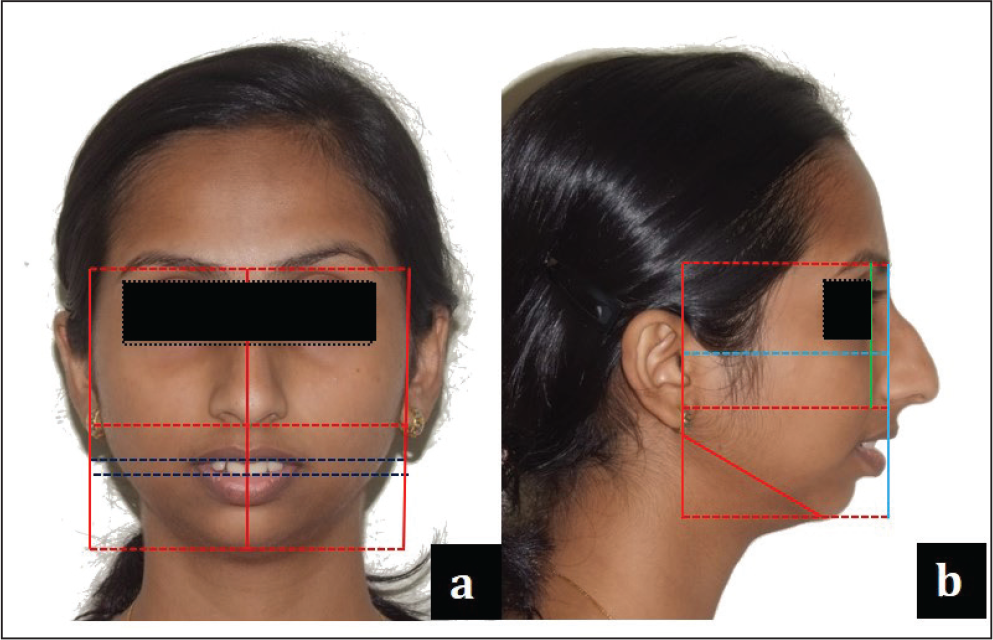
Anteroposterior: Class II skeletal pattern with markedly convex facial profile and posterior divergence. Soft tissue pogonion is severely retrusive relative to zero meridian. Has a prominent dorsal hump of the nose. The mandible was underprojected relative to the upper face, resulting in a short chin-throat length.
Vertical: Increased Frankfort-Mandibular plane Angle (FMA). A reduced LAFH (Lower Anterior Facial Height) was apparent (62:65:55). Within the lower third, her upper one-third was reduced in comparison to the lower two-third. All of the patient’s maxillary incisors were visible at rest (6 mm), and there was 7-mm display of gingiva on smile, but with a consonant smile arc.
Transverse: Mesoprosopic facial form with acceptable facial symmetry and balance on frontal examination. Intercanthal distance is proportional with the alar base width (29:30). The facial and dental midlines were coincidental.
Soft Tissue Assessment
Upper and lower lips had normal tonicity. Lower lip was everted and protrusive relative to Ricketts’ E-plane. The lips were potentially incompetent with an interlabial gap of 6 mm; anterior oral seal created by lip-to-lip contact with mild hyperactivity. The nasolabial angle was obtuse, with average mentolabial sulcus. The philtrum and commissure height was proportional (20:21).
(Measurement values in mm)
Clinical Examination: Intraoral Features
Soft tissues: No abnormality detected
Oral hygiene: Good
Erupted teeth present:
General dental condition: Good dental health with a Class I amalgam restoration on 36.

Crowding/Spacing
Maxillary arch: Asymmetrical with anterior spacing present in relation to 11 and 21, proclination of 12, retroclination of 11 and 21, and a high vault palate. No effective crowding present (in terms of arch length-tooth material size, the space required is 72 mm and space available is 73 mm).
Mandibular arch: U shaped, asymmetrical with crowding in relation to the anterior teeth. Total arch crowding of 6 mm (in terms of arch length-tooth material size, the space required is 63 mm and space available is 57 mm).
Occlusal Features

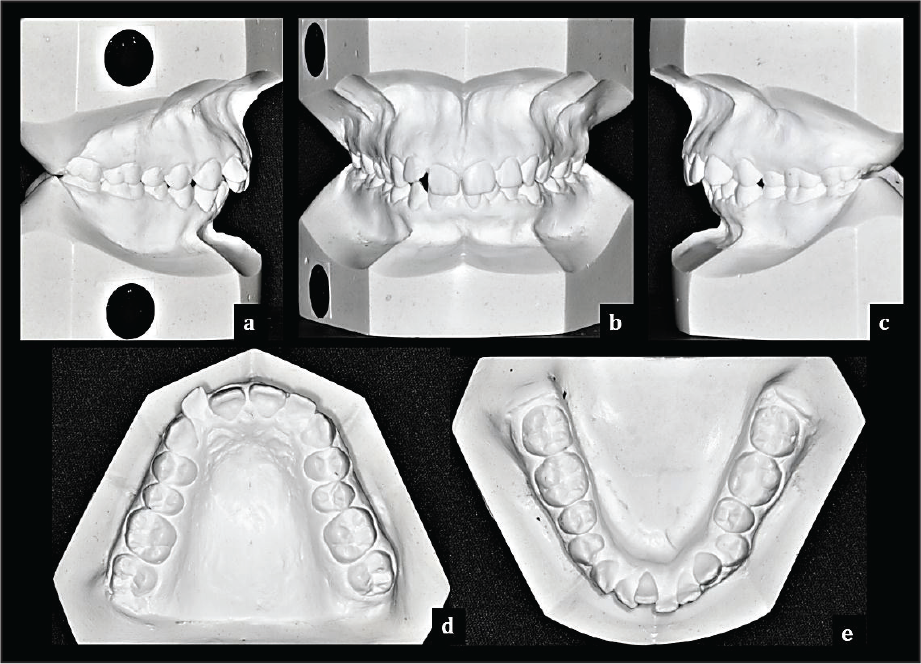
Incisor relationship: Class II Div 2
Overjet (mm): 5.5 mm
Overbite: 4 mm (50%)
Centerlines: Upper and lower dental midlines were coinciding with the facial midline.
Left buccal segment relationship: Class II (End on) molar (by 3 mm) and Class II canine (by 3 mm) relationship associated with normal buccal overlap.
Right buccal segment relationship: Class II (End on) molar (by 1 mm) and Class II canine (by 2 mm) relationship associated with normal buccal overlap.
Crossbites: Nil
Displacements: Labioversion of 12; mesiolabial rotation of 21; mesiobuccal rotation of 24; distopalatal rotation of 25; buccoversion of 34; linguoversion of 41.
Other occlusal features: Marginal ridge discrepancy in relation to 16-17, 13-12, 24-25, 26-27, 34-35, 33-34, and 43-44. Imbrication of lower anteriors.
Bolton’s Discrepancy: Overall ratio = 90.42%, corresponds to maxillary tooth material excess, but within the normal range (overall excess = 0.90 mm). Anterior ratio = 76.08%, corresponds to maxillary tooth material excess, but within the normal range (anterior excess = 0.66 mm).
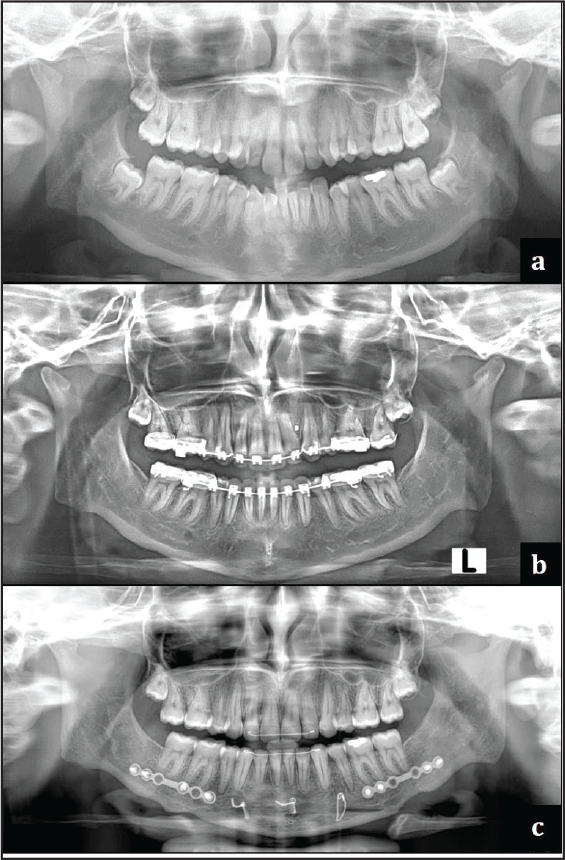
General Radiographic Examination
Pretreatment radiographs taken:
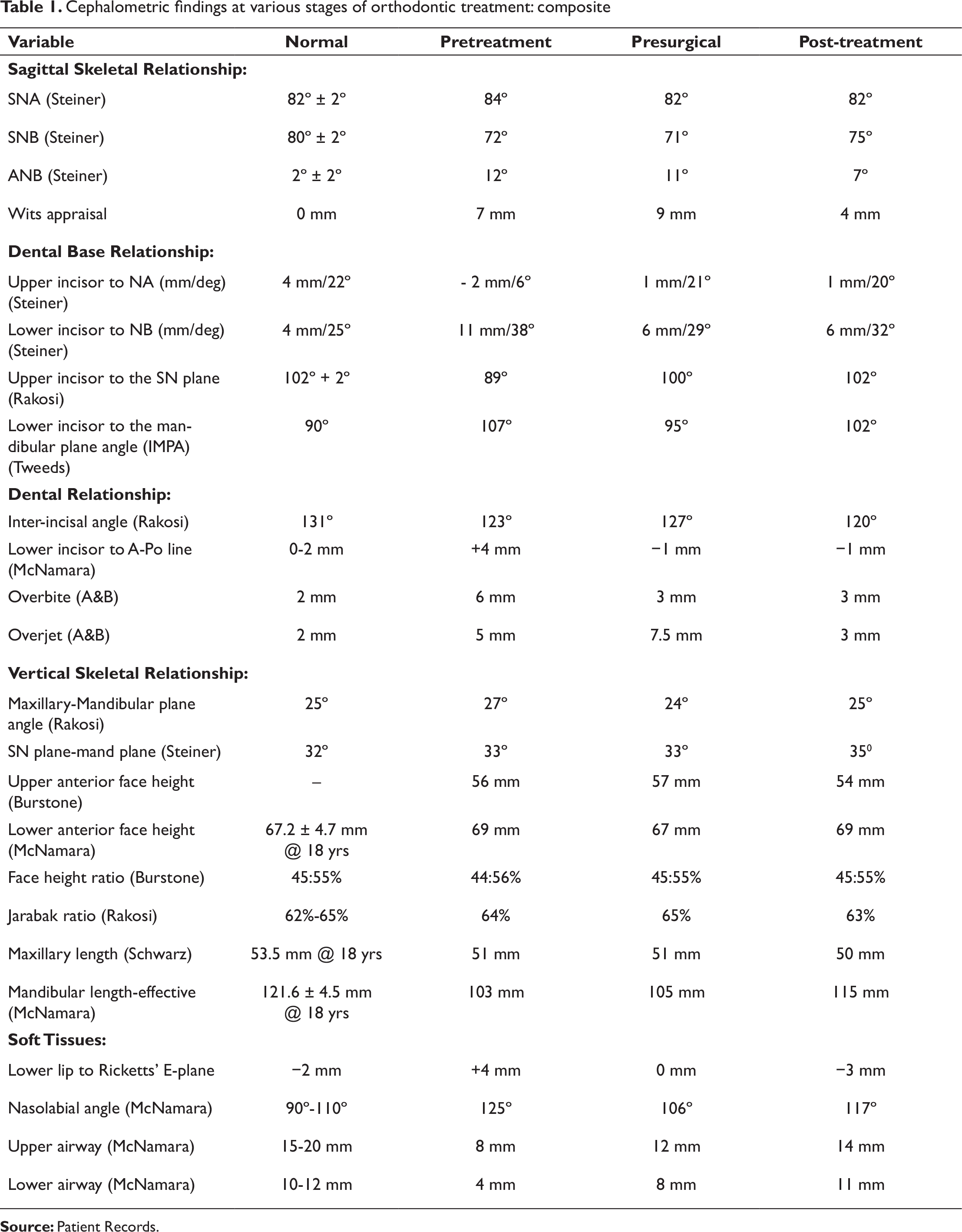
Cephalometric findings at various stages of orthodontic treatment: composite
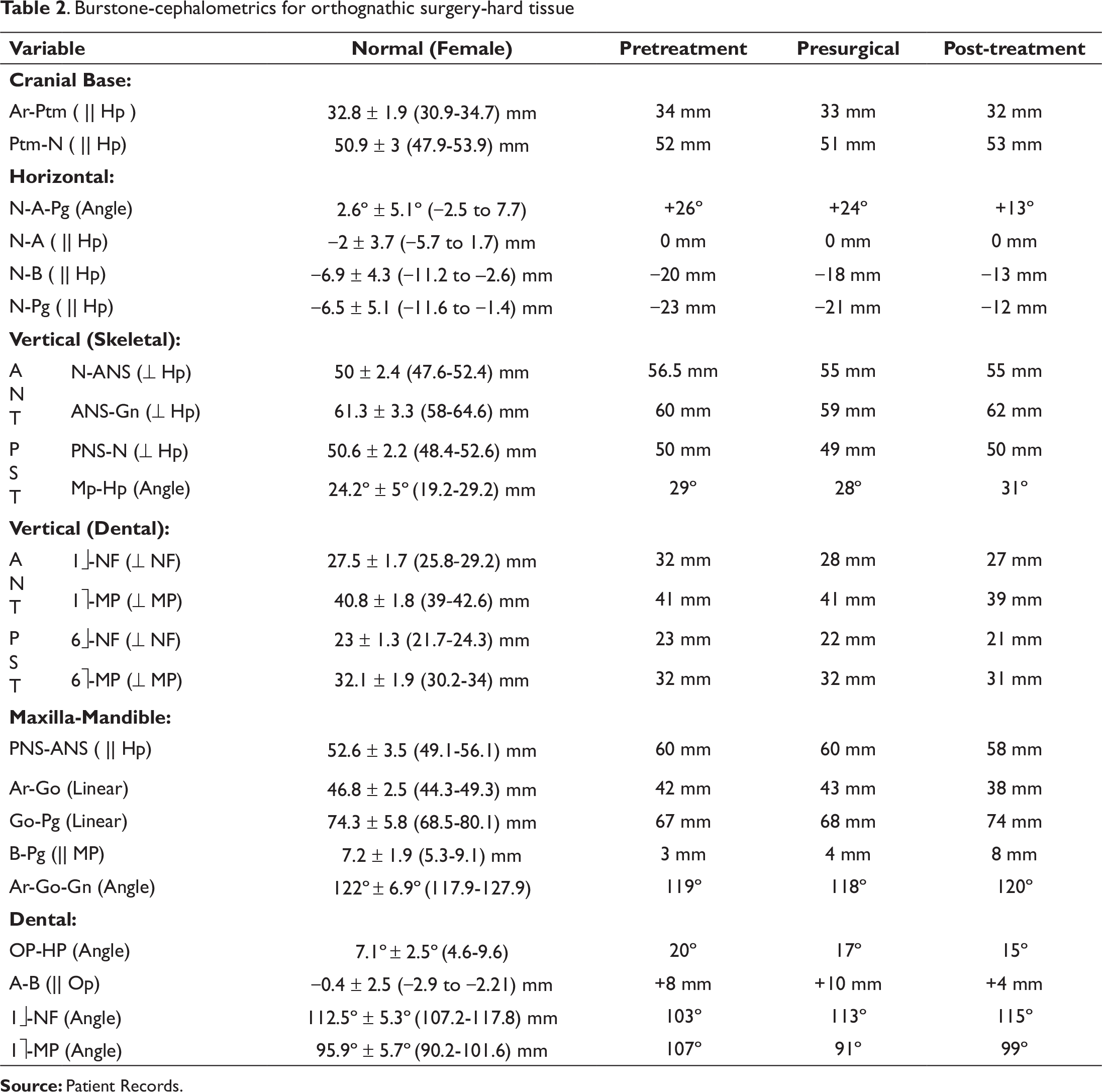
Burstone-cephalometrics for orthognathic surgery-hard tissue
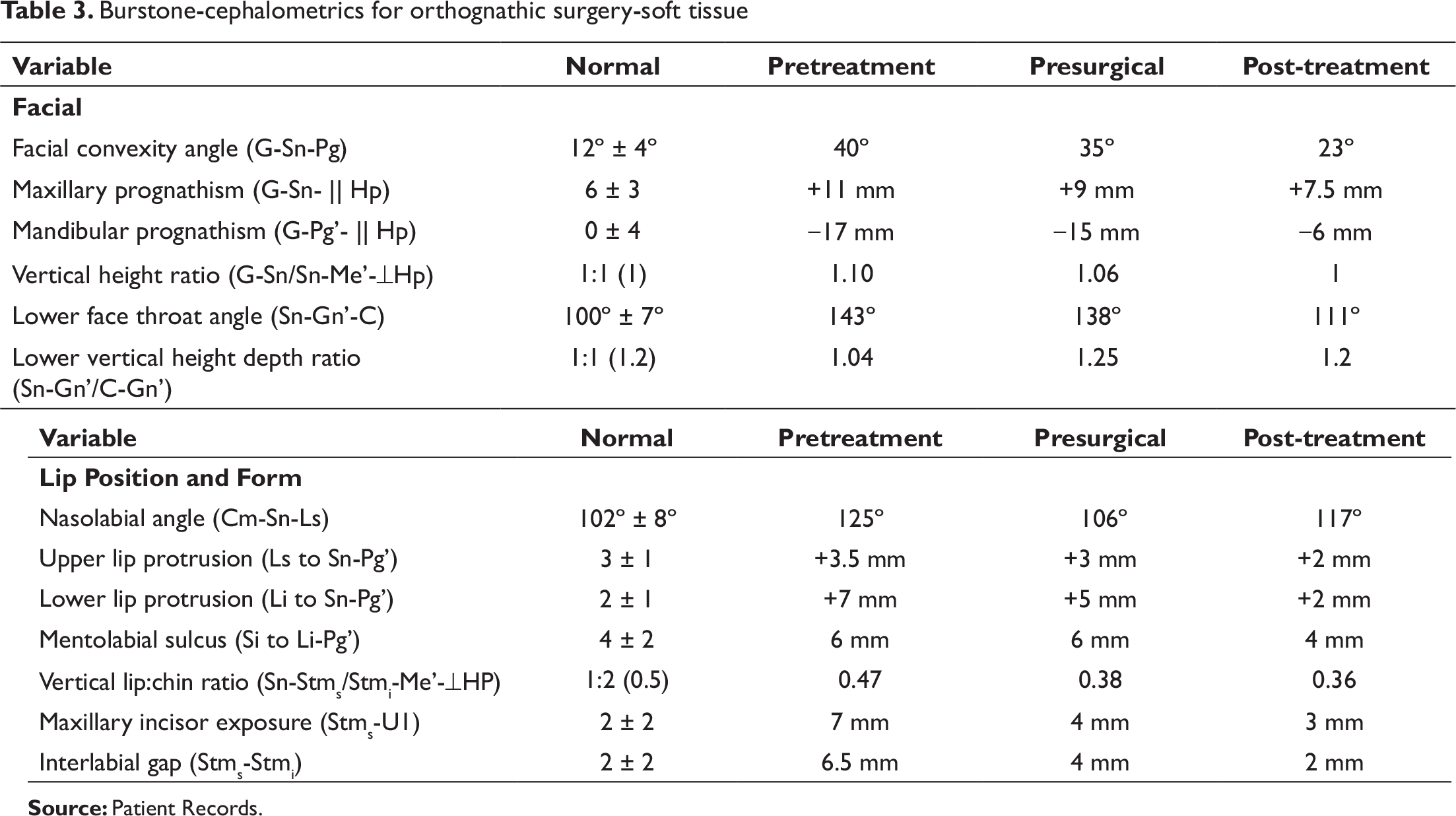
Burstone-cephalometrics for orthognathic surgery-soft tissue
Relevant radiographic findings:
The normal complement of permanent teeth was present with no abnormalities of the surrounding structures and regions; additionally, there were no abnormalities in the tooth form. The third molars were present in all the quadrants but were impacted. The alveolar crestal bone level of the teeth present was within the normal limits of the CEJ. (Cemento-Enamel Junction) The condylar morphology was “angulated.”
Pretreatment Cephalometric Findings and Their Interpretation
Various cephalometric findings are described in Tables 1-3.
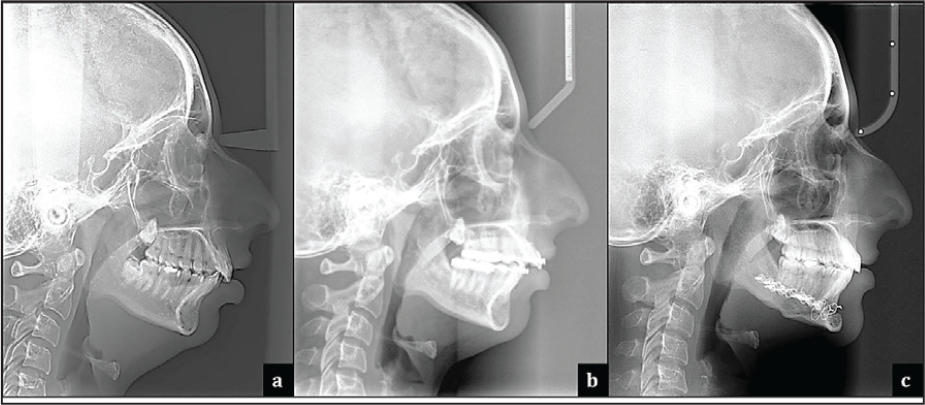
Skeletal: The cephalometric analysis revealed a severe Class II skeletal base with marked convexity, having an ANB of 12° and a Wits appraisal of +7 mm. This was due to a retrognathic mandible with a reduced effective length by 18 mm from ideal. In relation to the cranial base, her mandible was deficient (N-B || Hp = −20 mm & N-Pg || Hp = −23 mm). This was complicated along with VME indicated by an increase in the middle facial height (N-ANS) by 6.5 mm and maxillary anterior dental height (1≈ - NF) by 4.5 mm. The maxillary posterior skeletal and dental heights were normal. The ramal length (Ar-Go by 4.8 mm) and the mandibular body length (Go-Pg by 7.3 mm) were reduced. Her chin prominence (B-Pg by 4.2 mm) was also reduced. She had a relatively average growth pattern (higher end), and her lower anterior facial height was within the average.
Dental: The maxillary anteriors (centrals) were retroclined by both U1-NA (6°) and U1-SN (89°) angles and retropositioned as well, and the mandibular anteriors were significantly proclined by the values of L1-NB (38°) and IMPA (107°). Overbite and overjet were increased at 6 mm and 5 mm, respectively. There was increased incisor exposure at rest (7 mm) with an increased interlabial gap (6.5 mm).
Soft tissues: Has an obtuse nasolabial angle (125°), with protrusion of the lower lip relative to the Ricketts’ E-plane (4 mm). The lower face throat angle was obtuse (143°). The upper and lower airway dimensions, as measured by McNamara analysis, were reduced at 8 mm and 4 mm, respectively.
Diagnostic Summary
The skeletal and dental relationships confirm a Class II skeletal base malocclusion due to retrognathic mandible, along with VME, and reduced upper and lower airway dimensions and retrogenia. Both middle third skeletal facial height and maxillary anterior dental height were increased. Clinically, LAFH was reduced; within the lower third, her upper one-third was reduced in comparison to the lower two-third. The right and left first molars and canines were at end-on relation, and the incisor relationship was in Class II. Upper central incisors were retroclined, whereas lower incisors had significant proclination and crowding. Upper incisors exhibited Class II Div 2-like features. There was labioversion of 12. Upper and lower midlines were relatively coincident with the facial midline. She has potentially incompetent lips with an everted and protrusive lower lip. The nasolabial angle was obtuse, and nasal type was leptorrhine with a prominent dorsal hump. There was excessive display of incisors at rest, with 7 mm of gingival exposure at smile. Overjet measured 5.5 mm and the overbite was 4 mm. There was no functional shift.
Problem List
Class II skeletal base due to retrognathic mandible
VME with increased incisal show at rest and smile
Reduced airway dimensions
Retroclined maxillary central incisors, with labioversion of 12
Crowding and proclination of lower anterior teeth
Bilaterally end-on molar and canine relation; Class II incisor relation
Potentially incompetent lips and everted lower lip
Prominent nose morphology
Aims and Objectives of Treatment
Correction of the Class II skeletal base and vertical skeletal discrepancy
Establish proper buccal occlusion
Achieve Class I molar and canine relation on both sides
Achieve normal overjet, overbite, and midline relations
Achieve soft tissue esthetics and maintain the consonant smile arc
Treatment Plan
Due to the severity of her skeletal malocclusion, it was decided to address her anteroposterior skeletal discrepancy with surgical orthodontics. For the correction of the VME, LeFort I with differential maxillary impaction was ruled out during the Joint Clinic discussion because of the clinically reduced lower anterior facial height. Hence, it was decided to camouflage her VME with skeletal anchorage, primarily aimed at intrusion mechanics. A surgical treatment objective was performed to confirm the predicted range of surgical correction.
Dentos® 1312-06 mm microimplants apically b/w 12-13 and 22-23
Dentos® 1312-07 mm microimplants apically and mesial to U 6’s.
The TADs are to be used for achieving maxillary dental intrusion and for any necessary retraction mechanics.
Section 2. Treatment
Treatment Progress
Start of active treatment: [February 17, 2012]
Age at start of active treatment: [21 years 9 months]
End of active treatment: [February 25, 2016]
Active treatment time: [48 months]
End of retention: [March 15, 2018]
Key Stages in Treatment Progress (Date and Stage)
February 17, 2012: Banding and bonding of upper and lower arches. U & L 0.014 Cu NiTi placed.
November 28, 2012: Upper and lower leveling and aligning achieved on 19 × 25 SS. Lower en masse retraction initiated with friction mechanics on hooks crimped distal of lateral incisors
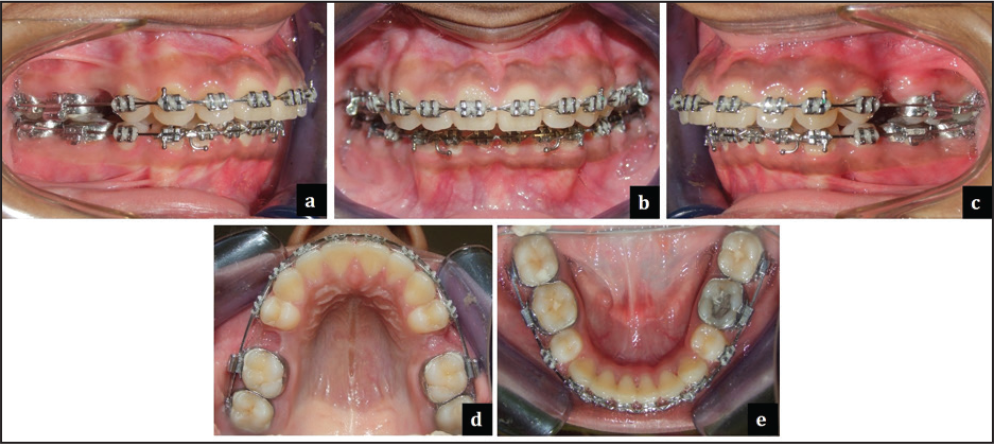
August 6, 2013: Lower arch retraction and decompensation completed; all second molars banded for further leveling and aligning (Figure 7)
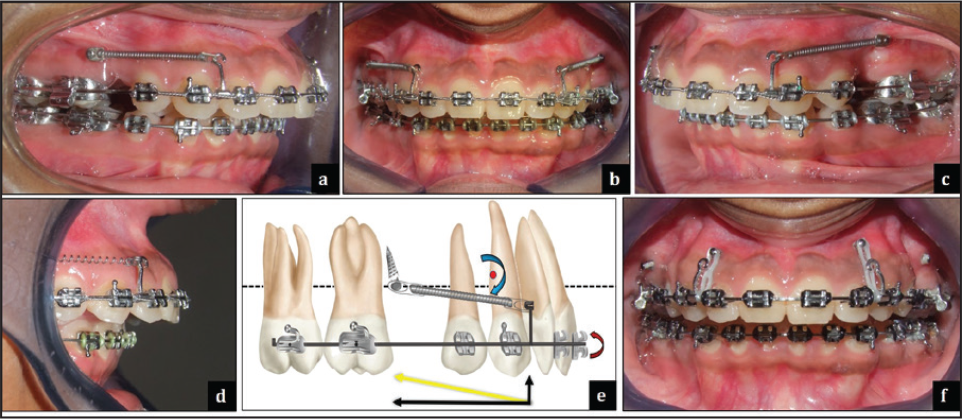
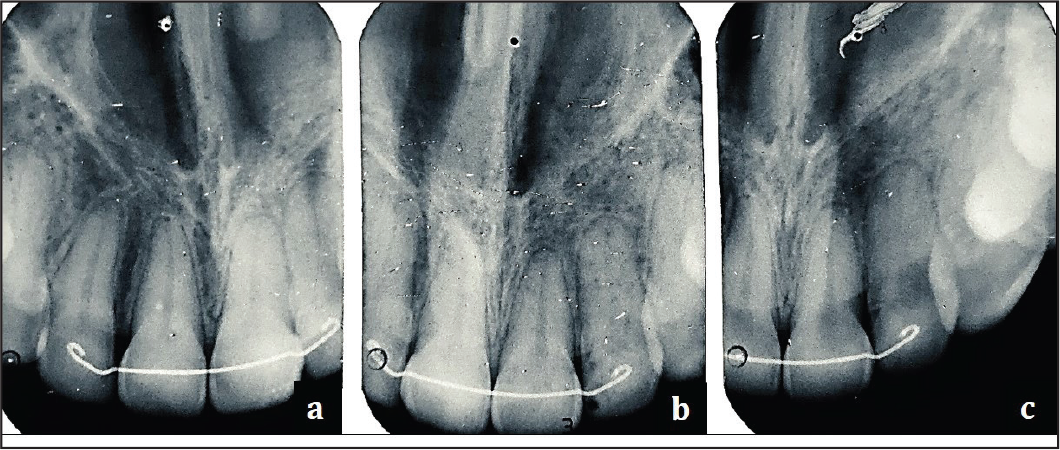
November 16, 2013: (7-7) leveling and aligning achieved on 19 × 25 SS. Patient underwent delayed extraction of upper 5’s. January 17, 2014: After radiographic and clinical assessment, a 7 mm length × 1.3 mm diameter microimplant was placed mesial to upper first molars. The upper 19 × 25 SS posterior section was slenderized and space closure was initiated, with extended hooks/power arm and NiTi closed coil springs for bodily retraction and intrusion. 1 Force measured at 250 gm per side 7 (Figure 8).
May 17, 2014: After radiographic and clinical assessment, a 6 mm length × 1.3 mm diameter microimplant was placed between upper lateral incisor and canine bilaterally for intrusion mechanics. Vertical E-chains placed for the same; force measured at approximately 100 gm (Figure 8).
July 5, 2014: Posterior microimplants removed and mesialization of upper molars initiated with Class I vector
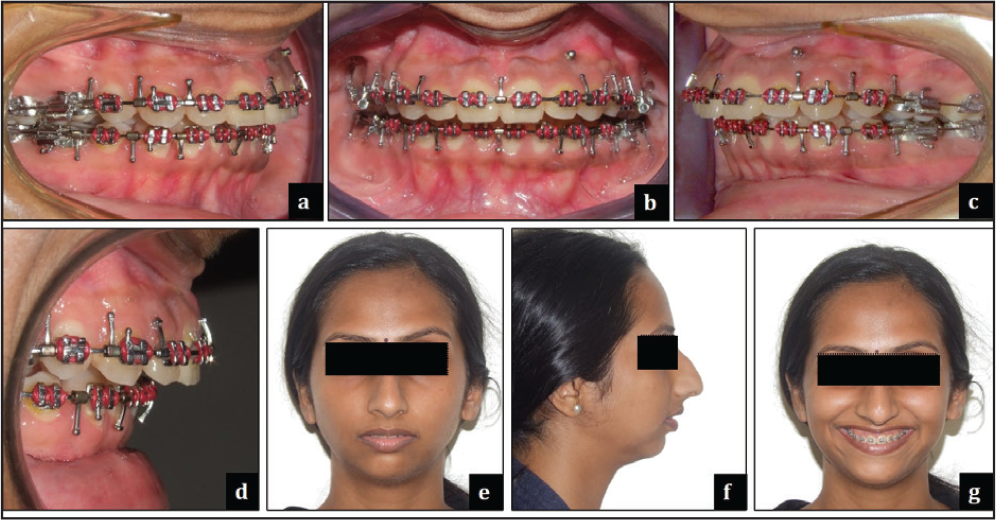
November 20, 2014: Presurgical phase completed with Class II molar and canine relation, bilaterally and with an overjet of 8.5 mm (Figure 9). Patient opted for surgery in June 2015. Stage lateral cephalogram and OPG recorded (Figures 5 and 6).
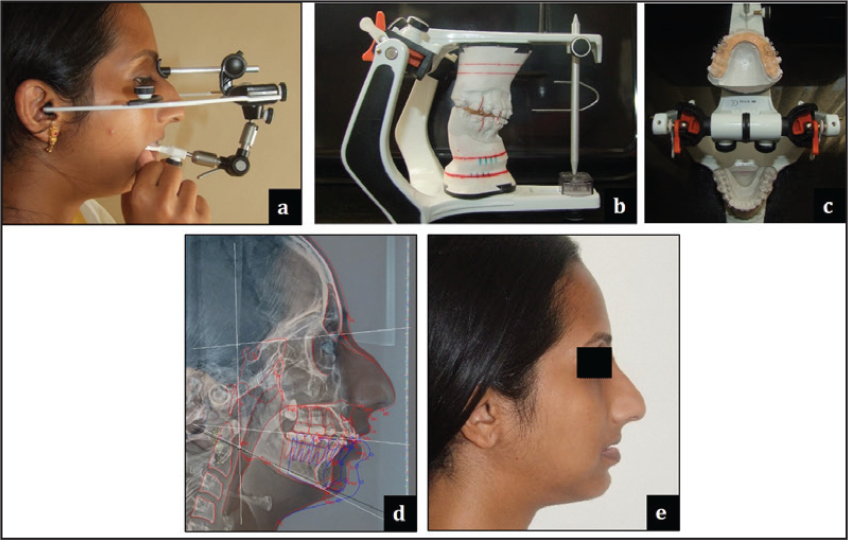
May 2, 2015: Jaw relations recorded for mock surgery and splint fabrication. Following face-bow transfer and articulation, 6.5-mm advancement model surgery was performed before splint fabrication (Figure 10).
Surgical hooks placed on upper and lower 21 × 25 SS AW’s (Figure 9).
June 12, 2015: Surgery: BSSO mandibular advancement of 6.5 mm and augmentation genioplasty of +4 mm. The patient did not opt for rhinoplasty (Figure 11).
June 26, 2015: The postsurgical phase initiated. Advised light Class II vector elastics.
July 10, 2015: Ligature consolidated and AW sectioned. Postsurgical settling of occlusion initiated.
September 25, 2015: Maxillary anterior intrusion completed. Passively ligated the AW to the TADs predebonding finishing and detailing8 initiated.
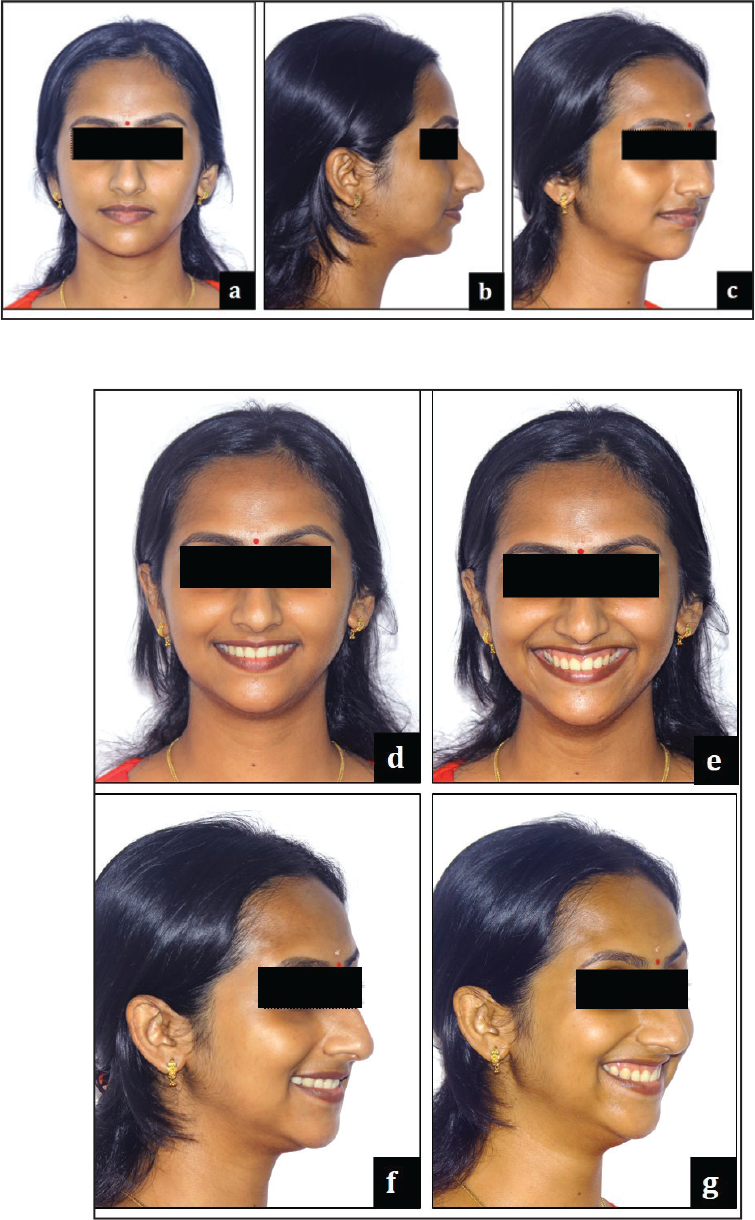
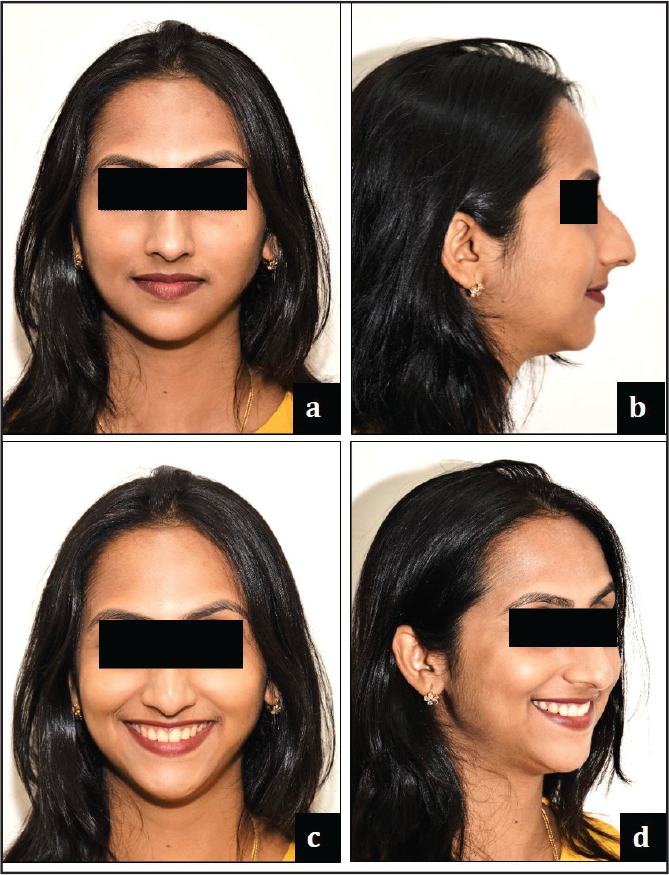
February 25, 2016: Debonded upper and lower arches. Bonded lingual retainers placed in relation to upper (2-2) and lower (3-3). Gingivectomy was performed for microesthetics (Figure 12), and post-treatment photo records were taken on March 21, 2016 (Figures 13 and 14).



Presurgical Cephalometric Findings and Their Interpretation
Various cephalometric findings are described in Tables 1-3.
Skeletal
Skeletal Class II Base with retrognathic mandible along with Vertical Maxillary Excess, marked facial convexity and Retrogenia. The maxillary anterior dental height has reduced, along with improvement in incisal exposure at rest and smile. The Lower Anterior Facial Height was within the average.
Dental
The maxillary and mandibular incisor proclination was restored to within its normative inclination limits as observed from the linear and angular changes in its relation to the cranial base (U1-NA 1 mm/21o and L1-NB 6 mm/29o) and the respective skeletal bases (L1-APog-1 mm). There was a mild increase in the mandibular plane angle by 1°. The overbite reduced to 3 mm and the overjet increased to 7.5 mm from the decompensation.
Soft Tissue
There was favorable improvement in the nasolabial angle and lower lip protrusion. The lower face throat angle remained obtuse. The maxillary anteriors have favorably inclined, and there was reduction in the lower incisor proclination as well.
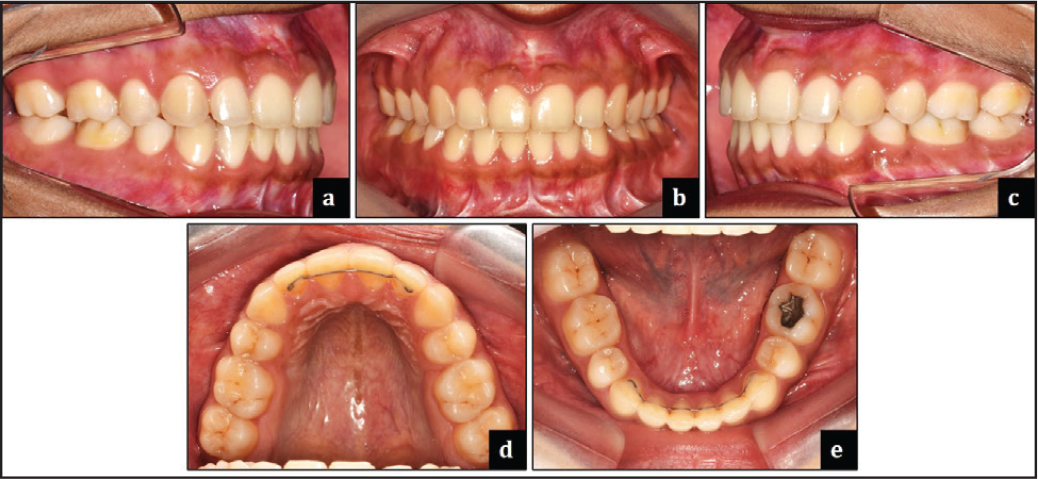
Section 3. Post-treatment Assessment Occlusal Features
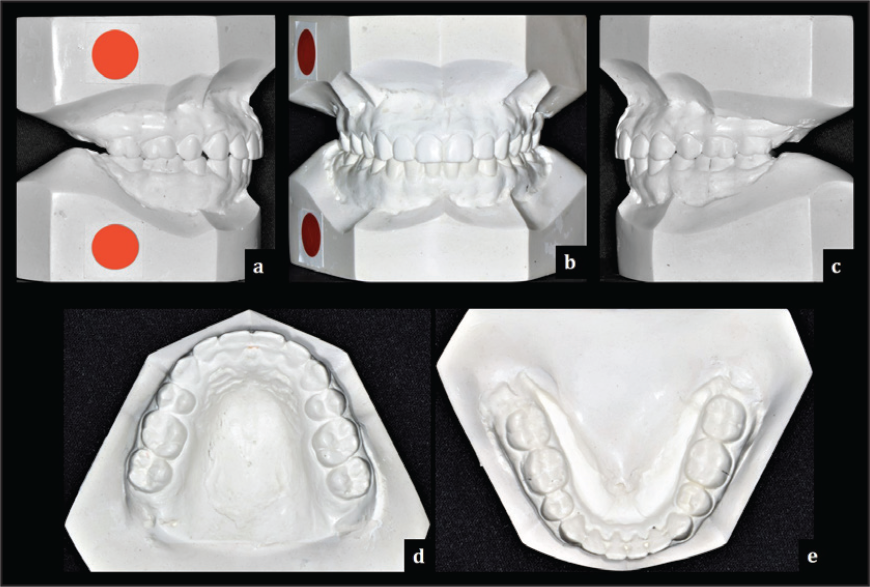
Various occlusal features at the end of orthodontic treatment are shown in Figure 15.
Incisor relationship: Class I
Overjet (mm): 2 mm
Overbite: 2.5 mm or 33%
Centrelines: Lower midline shift of 1 mm to the left
Left buccal segment relationship: Class I molar relation and Class I canine relation
Right buccal segment relationship: Class I Molar relation and Class I Canine (toward end on) relation
Crossbites: None
Displacements: None
Functional occlusal features: Mutually protected occlusion with optimal overjet and overbite. No premature occlusal contacts during mandibular movements.
Other occlusal features: Mild marginal ridge discrepancy present between 16-17 and 26-27.
Complications Encountered During Treatment
Occlusal Indices
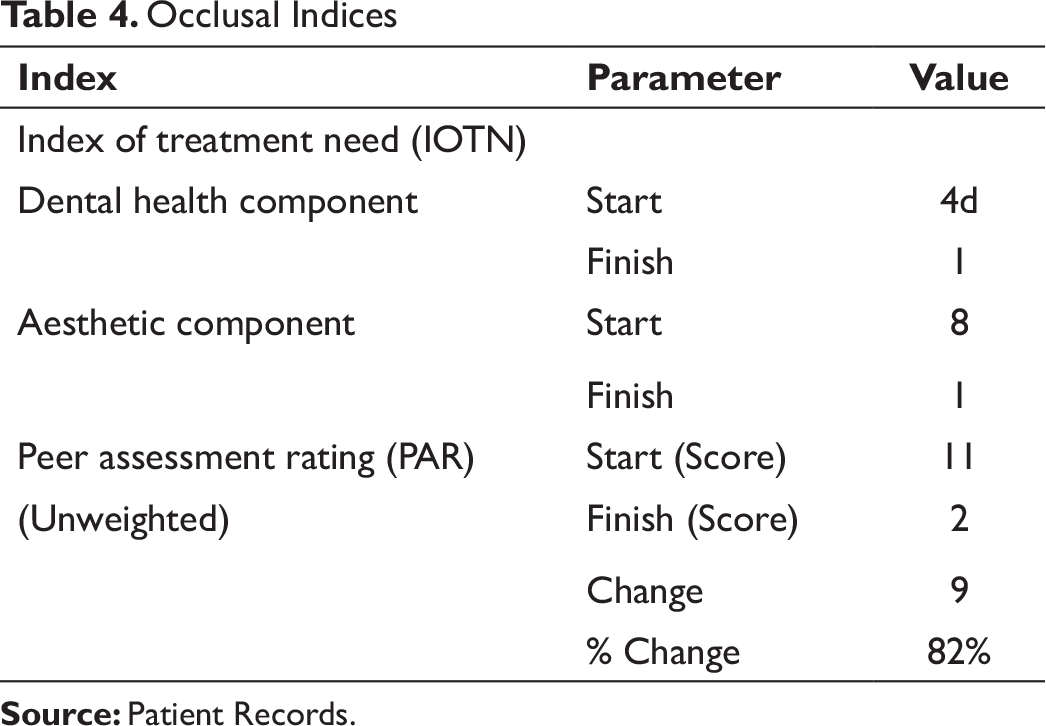
Occlusal Indices
The PAR index was reduced from 11 to 2 with a change of 82%.
The IOTN (DHC) and IOTN (AC) was 4d and 8 at the start of treatment, respectively, and 1 at the end of treatment for both components.
Radiographs Taken Toward/at End of Treatment
Radiographs taken:
Relevant radiographic findings:
Maxillary incisors root resorption was evident. As per the Levander and Malmgren classification,
9
score 3 represents root resorption apically, amounting from 2 mm to less than one-third of the original root length. The crown to root ratio has a good prognosis.
Post-treatment Cephalometric Findings and Their Interpretation
Various cephalometric findings are described in Tables 1-3.
Skeletal
The Class II skeletal base A-P discrepancy was improved surgically, with a reduction of 5° in the ANB value (from 12° to 7°) and Wits appraisal (from 7 to 4 mm). There was an increase in the mandibular body length (from 67 mm to an ideal of 74 mm) and in chin prominence (from 3 mm to an ideal of 8 mm). The position of the mandible in relation to the cranial base has shown significant improvement (N-B || Hp from −20 to −13 mm and N-Pg || Hp from −23 to −12 mm). The VME was camouflaged with a microimplant supported intrusion, resulting in an ideal maxillary anterior dental height (1û - NF from 32 to 27 mm). In the vertical plane, the vertical face height ratio was now ideal at 45:55%; the LAFH was within normal limits; and the mandibular plane angle has increased marginally.
Dental
Upper and lower anterior teeth inclination was favorably corrected (U1-NA 1 mm/20o and U1-SN 102o ), though the lower incisor inclination was still above average (L1-NB 6 mm/32o and IMPA 102o ), as well its position to the respective skeletal bases (L1-APog-1 mm). An ideal incisal exposure at rest (from 7 to 3 mm) has been achieved.
Soft Tissue
Comparison of pretreatment and post-treatment results showed a significant improvement in soft tissue esthetics by achieving the following: a reduction in the facial convexity (from 40° to 23°), lower face throat angle (from 143° to 111°), and nasolabial angle (from 125° to 117°); ideal vertical height ratio (1); ideal lower vertical height depth ratio (1.2); ideal upper and lower lip position in reference to Ricketts’ E-plane. The upper and lower airway dimensions, as measured by McNamara analysis, improved at 14 mm and 11 mm, respectively.
Results Achieved Include
Class II skeletal base discrepancy was addressed favorably with improvement in facial profile and aesthetics.
In the vertical skeletal relation, the maxillary excess was successfully camouflaged.
Upper and lower anterior teeth crowding and proclination were resolved.
A stable buccal occlusion was achieved with Class I molar and canine relation (right canine toward end on by 1.5 mm).
A Class I incisor relation with an optimal overjet and overbite was established.
Adequate functional occlusion with canine guidance on left and right lateral excursions; incisal guidance on protrusion with posterior disclusion and no premature occlusal contacts during mandibular movements.
The upper dental midline was coincident to the facial midline, whereas the lower midline was shifted to the left by 1 mm.
Ideal maxillary incisor exposure at smile with a consonant smile arc.
Adequate results were obtained in regard to esthetic harmony, structural balance, and functional stability (Tables 4 and 5).
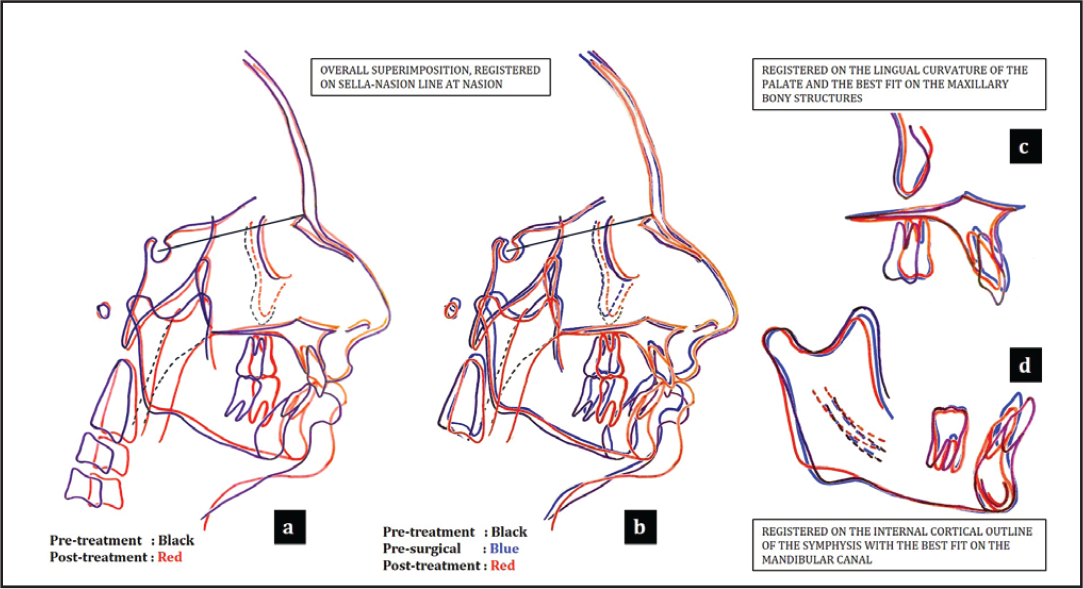
The pretreatment, presurgical, and post-treatment cephalometric superimpositions are shown in Figure 16.
Postretention stability along with the ideal crown to root ratio was maintained on long-term follow-up after 2 years and 6 months (Figures 17-19)
Dental arch changes
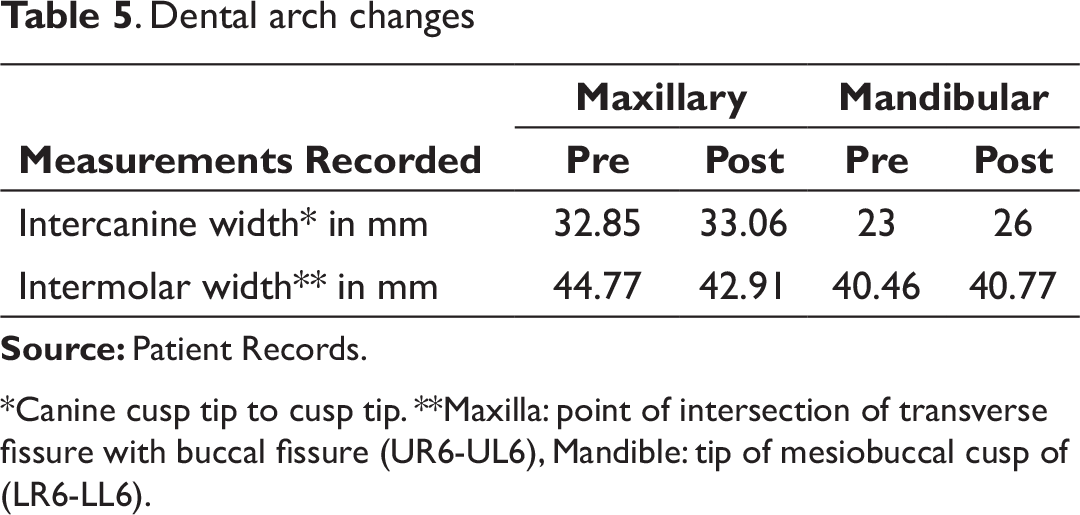
*Canine cusp tip to cusp tip. **Maxilla: point of intersection of transverse fissure with buccal fissure (UR6-UL6), Mandible: tip of mesiobuccal cusp of (LR6-LL6).
Section 4. Critical Appraisal
MS was successfully treated by orthodontic camouflage over 48 months. The aims of treatment were accomplished and the patient’s concerns were addressed addressed. MS was notably pleased with the treatment outcome. Good occlusal and aesthetic result was achieved, and this was reflected in the PAR and IOTN scores.
Skeletal: It was decided against a surgical intervention for addressing the VME due to the clinically reduced LAFH. Otherwise, a bi-jaw surgery with differential impaction of the maxilla, along with BSSO mandibular advancement, would have been an ideal choice. Though mandibular advancement is considered a stable procedure,
10
the tendency for relapse was considered due to the 6.5-mm mandibular advancement. However, with the overall arch form being maintained along with good intercuspation, the long-term stability is considered good. The patient will be kept on regular follow-up to evaluate for any TMJ (Tempero-Mandibular Joint) concerns. Dental: After the leveling phase of the upper arch, the anteriors were proclined, resulting in a need for retraction correction. This could have been prevented if adequate anchorage preparations were taken to avoid the flaring of the upper anteriors. During microimplant-assisted intrusion, the maxillary anteriors undergo a Grade 3 root resorption as per the Levander and Malmgren classification,
9
in spite of the ideal crown to root height ratio being maintained. This external apical root resorption amounting from 2 mm to less than one-third of the original root length could have been reduced if lighter and continuous force levels and/or segmental mechanics were used. Here for en masse anterior intrusion about 100 gm of force was used. There was an axial error in 12 bracket positioning, which was corrected during the finishing and detailing phase. An MBT prescription would have achieved an increased palatal root torque in the upper incisor brackets, thus controlling the flaring of the anteriors. Dental midline shift of 1 mm was present in the lower arch, which is within the acceptable limit with regard to facial esthetics.
11
The right canine relation was toward end on, in spite of a stable functional occlusion. Soft Tissues: Harmonious soft tissue esthetics were achieved. The lips were competent toward the end of the treatment, with an ideal incisal exposure at posed smile. The changes in lip length with age could potentially influence the current smile esthetics. Rhinoplasty would be supportive to reduce the prominence of the nose. Overall, the treatment duration was prolonged due to the delay in undergoing extractions of the upper second premolars and the discontinuity between subsequent appointments.
Declaration of Patient Consent
The author certifies that he has obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Acknowledgment
The author would like to thank Dr Oommen Aju Jacob MDS, FDS RCS (Eng), FFD RCS (Ire), DNB for the orthognathic surgical management.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.