
Abstract
Abstract
NK, a 12-year-old male patient, presented with a Class II division 1 incisor relation on a Class II skeletal base with a decreased maxillomandibular plane angle and decreased face-height ratio. He had a convex profile, incompetent lips, lip trap, deep mentolabial sulcus, everted lower lip and a positive VTO (Visual Treatment Objective). Intraorally, he presented with bilaterally Angle’s Class II molar relation and canine relation, scissor bite in the region of first premolars bilaterally, a closed bite and a 13 mm overjet. He presented with mild spacing in the upper arch and mild crowding in the lower arch with a pronounced curve of Spee. This was further complicated as the LR6 was endodontically treated and temporarily restored; also, enamel hypoplasia was seen in all permanent first molar region. The treatment was carried out in two phases, Phase I involved growth modulation done with a twin block appliance, and Phase II was the postfunctional orthodontic phase for dental corrections and finishing and detailing of occlusion, which was done with a preadjusted edgewise appliance (0.022 × 0.028˝ slot) with MBT (McLaughlin, Bennett, Trevisi) prescription. The posttreatment results were highly satisfactory, showing improvement in facial esthetics and occlusal traits as well as good long-term stability as was evident in the 3-year retention records.
Keywords
Introduction
The most common skeletal problem in orthodontics is the Class II malocclusion characterized by mandibular deficiency.1-5 Many methods for the orthodontic management of skeletal Class II malocclusion are published in literature. However, when conducive growth is available, with respect to the timing of treatment and growth vector, growth modulation is the most favored modality of treatment. Out of the array of the removable functional appliances available, “the Standard Twin Block appliance” is preferred by many clinicians due to the ease of use by the patient and ease of management of the appliance. It was first introduced by Clark in 1988 6 and consists of two separate, upper and lower, removable plates with acrylic blocks trimmed to an angle of 70°. These separate plates make the twin block appliance different in comparison with other removable functional appliances, which are basically monoblocks. Theoretically, this plus a less bulky appearance would increase patient acceptance of the appliance. Patients would also have more freedom in their mandibular movements. All these considerations could conceptually produce different treatment results compared with the removable functional monoblocks. 7 The following case report illustrates the use of a standard twin block appliance for skeletal correction of a Class II division 1 malocclusion in a 12-year-old male patient.
Case Report
Section I
Pretreatment assessment: History and clinical examination
NK, a 12-year-old boy, came with a chief complaint of forwardly placed upper front teeth and presented with a Class II division 1 incisor relation on a Class II skeletal base with a decreased maxillomandibular plane angle and decreased face-height ratio. He had a convex profile, incompetent lips, lip trap, deep mentolabial sulcus, everted lower lip and a positive VTO (Visual Treatment Objective).
Relevant Dental History
The patient had a history of root canal treatment of the lower right first molar.
He also had a history of orthodontic consultation.
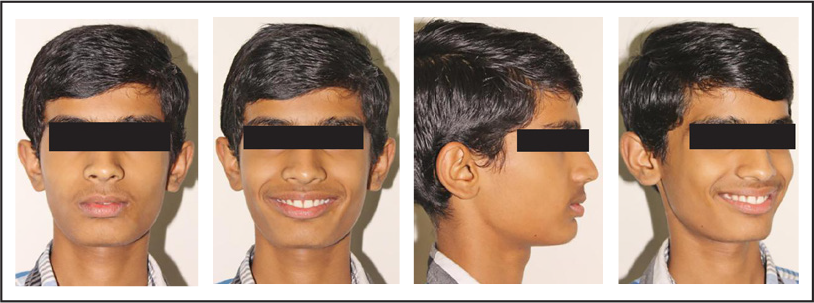
Clinical examination: Extraoral features (Figure 1).
Pretreatment Extraoral Photos

Pretreatment Intraoral Photos

Skeletal Assessment
The patient shows an acceptable facial symmetry and balance on frontal examination. He shows convex profile due to Class II skeletal pattern, progenia due to prominence of chin button, low clinical FMA and reduced lower anterior facial height proportion.
Soft Tissues
Upper and lower lips are incompetent at rest, showing severe lip strain observed with oral seal. Lower lip is everted with lip trap and a deep mentolabial sulcus and a decreased nasolabial angle.
General Dental Condition
The general dental condition showed an occlusal composite resin restoration on lower left first molar. History of endodontically treated lower right first molar with a blue colored composite resin temporary restoration. Non-fluoride enamel opacities resembling enamel hypoplasia was seen on all the first molars. Improper contact (post-restoration) was noted between lower right second premolar and lower right first molar.
Maxillary arch:
- Ovoid arch form
- Mild spacing in the upper anterior region
- Proclined upper anteriors
- Mesial out rotations of all premolars and distal in rotations of canine
Mandibular arch:
- Ovoid arch form
- Mild crowding in the anterior with a pronounced curve of Spee
Other features:
- lingually tipped lower right canine, distal out rotation of lower left first premolar and second premolar, and mesial out rotation of lower right second premolar
- Improper contact of restored lower right first molar and the rotated second premolar
Occlusal Features
Incisor relationship: Class II
Overjet: 13 mm
Overbite: Closed bite with upper anterior covering more than 100% of lower incisors.
Left buccal segment relationship: Full unit Class II
Pretreatment Radiographs
Right buccal segment relationship: Full unit Class II
Other occlusal features: Scissor bite (buccal non-occlusion) seen with upper first premolars with respect to the lower canines and premolars bilaterally and a deep curve of Spee on both sides.
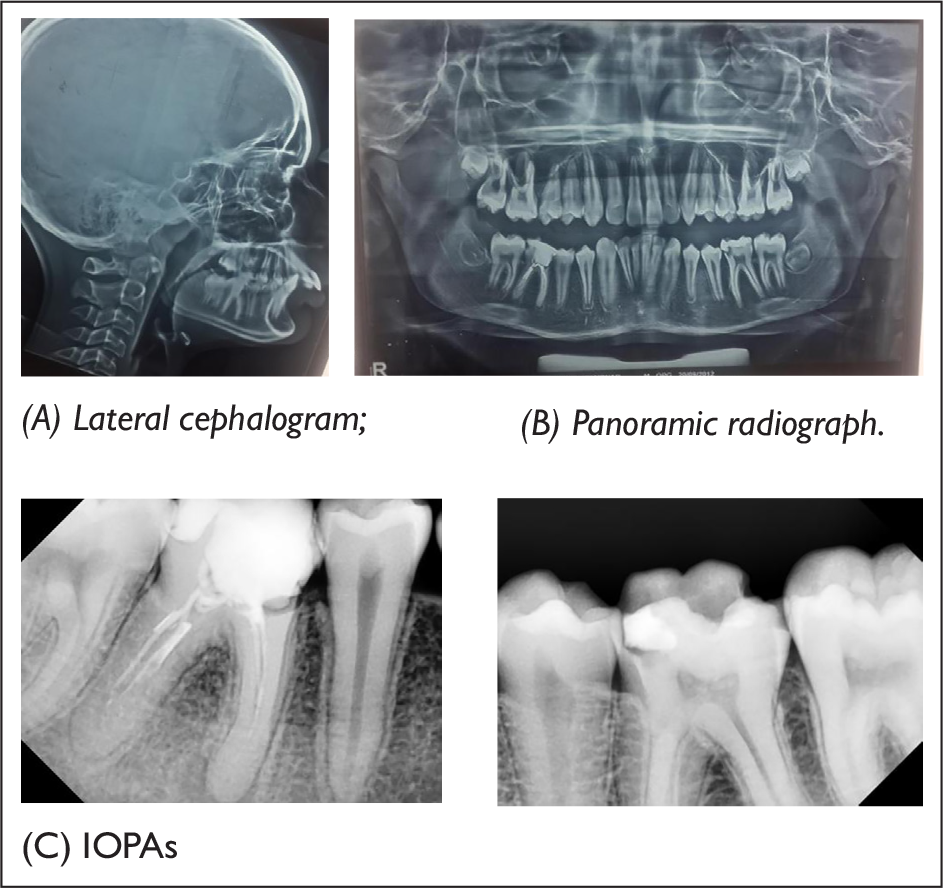
General radiographic examination (Figure 3)
Pretreatment radiographs taken were panoramic radiograph, a lateral cephalogram along with IOPAs (Intra Oral Periapical) of the lower first molars. Panaromic radiographic examination revealed the presence of unerupted second and third molars in all the four quadrants. The alveolar bone levels and root morphologies of the teeth were normal. Temporomandibular joint space appeared optimal with normal size, shape, and position of condyle heads. The IOPAs and the panoramic radiograph also showed endodontically treated lower right first molar (obturation filling short of apex in both the roots) and recurrent caries with lower left first molar.
Cephalometric evaluation revealed skeletal Class II jaw bases, horizontal growth pattern, decreased lower anterior facial height and facial height ratio, mild proclination of the maxillary incisors, increased overjet and overbite, convex profile and acute nasolabial angle. Skeletal maturity was assessed using the cervical vertebral maturation index (CVMI) staging, which showed Stage 2 of skeletal maturation (acceleration stage, with more than 65%–80% pubertal growth still remaining). The timing of peak mandibular growth was assessed by using the cervical vertebral maturation staging. The findings indicate the CS3, that is, peak in the mandibular growth, can occur during the year after this stage.
Model Analysis
Ashley Howe’s analysis indicated that this is a borderline case, and Pont’s analysis indicated the need for expansion. The Bolton’s analysis showed overall mandibular excess by 1.42 mm and anterior maxillary excess by 0.16 mm.
Diagnostic Summary
NK a 12-year-old boy presented with a Class II division 1 incisor relation on a Class II skeletal base with a decreased maxillomandibular plane angle and decreased facial height ratio. He presented with a convex profile, incompetent lips and a clinically retrusive mandible and showed a positive VTO. This was complicated with an endodontically treated lower right first molar with improper proximal contact due to temporary restoration. Intraorally, he presented with a bilateral Angle’s Class II molar and Class II canine relation with a 13 mm overjet and a closed bite. Cephalometrically, he presented with Class II skeletal pattern, proclined upper anteriors and decreased vertical proportions.
Aims and Objectives of Treatment
To match the skeletal bases
To achieve normal incisor axial inclination
To achieve lip competency at rest
To achieve Class I incisor relation
To achieve Class I molar and canine relation
To increase the lower anterior facial height
To unravel crowding and close the spaces
To achieve a pleasing esthetic profile
To achieve ideal overjet and overbite
To review prognosis with lower right first molar repeat root canal therapy and permanent coronal coverage
Treatment Plan
The treatment was carried out in two phases:
Phase I—Orthopedic correction with a removable functional appliance, that is, a standard twin block.
Phase II—Orthodontic correction and finishing and detailing with MBT prescription.
The preorthodontic phase included the following:
- Re-root canal for lower right first molar and re-restoration for lower left first molar. - Orthopedic correction with a removable functional appliance, that is, a standard twin block.
The orthodontic phase included bonding the patient with a preadjusted edgewise appliance with a MBT (0.022 × 0.028 slot) prescription. The anchorage was not a critical consideration during the fixed mechanotherapy as only minor dental corrections were desired. Hence, simple anchorage was used. It was later reinforced by bonding the second molar as well.
Additional Dental Treatments
Oral prophylaxis
Re-root canal treatment with 46 followed by coronal coverage.
Re-restoration with lower left first molar.
Proposed retention strategy:
For Phase I:
Anterior inclined plane to retain the mandibular advancement achieved.
For Phase II:
Upper arch—Upper removable retainer, a Begg’s wrap around bow to be worn full time for 6–8 months followed by a palatally bonded fixed retainer.
Lower arch—Lingually bonded fixed retainer.
Section II: Treatment
After thorough discussion with the patient about the proposed treatment plan, Phase I of the treatment was started. A standard twin block appliance (Figure 4) was delivered to the patient with a construction bite recorded with initial 9 mm of advancement of the mandible. Once the patient stated using the appliance full time, subsequently, the trimming of the appliance was started. The appliance was continued for 7 months, following which a re-advancement of 4 mm was done (Figures 5–7).
Twin Block Appliance Delivered

Five Months of Twin Block Use

Nine Months of Twin Block Use—Extraoral Photos
Nine Months of Twin Block Use—Intraoral Photos

At the end of Phase I (Figures 8 and 9), a preadjusted edgewise appliance (using a MBT 0.022″ slot prescription) was bonded on the upper and lower arches and a 0.014″ NiTi was placed. After 3 months into the fixed appliance treatment, the anterior inclined plane was removed and a 0.016″ NiTi was placed. Later in the treatment after the eruption of the second molars, they were bonded and a 0.017 × 0.025″ Cu NiTi archwire was placed. After the second molars were aligned and leveled, the settling of the occlusion was carried out with vertical settling elastics. The Phase II lasted for 17 months after which the fixed appliance was debonded and the patient was given lingually and palatally bonded fixed retainers made from 0.0175″ co-axial wire.
End of Phase I—Extraoral Photos

End of Phase I—Intraoral Photos

Complications Encountered During the Treatment
Compliance of the patient to wear the twin block initially was the major complication encountered during the treatment. Initially, the patient wore the twin block for a limited period. On follow up visits, he was advised to wear it for 24 hours, but he was non-compliant and did not use it for more than 4–6 hours a day. Positive reinforcement methods were used to make him compliant with the appliance. After 5–6 months, he started to use the appliance full time.
The lower twin block was once fractured in midline and hence had to be repaired.
Results Achieved
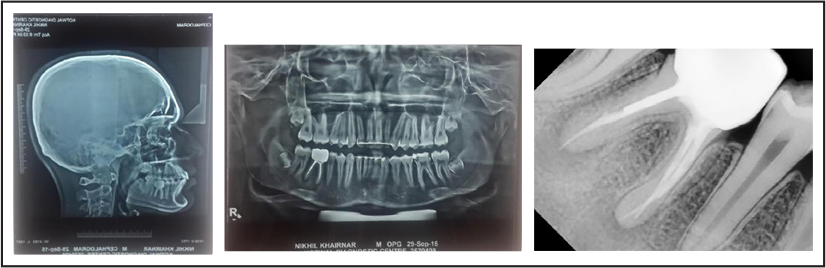
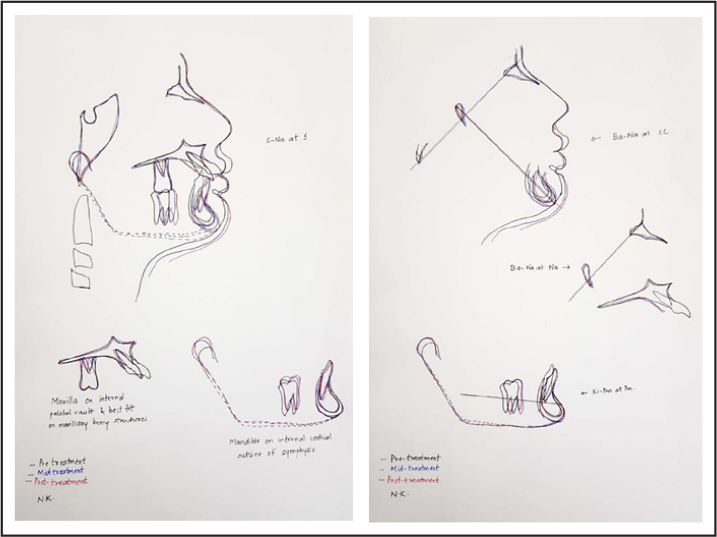
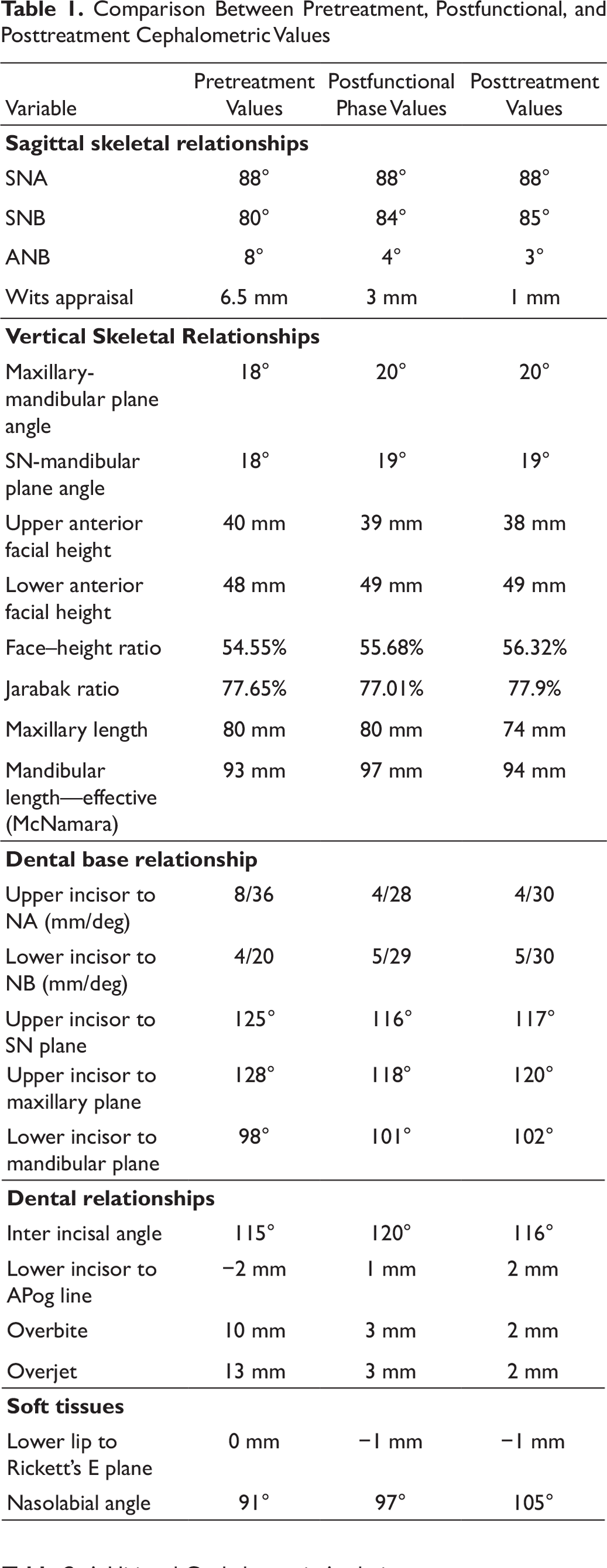
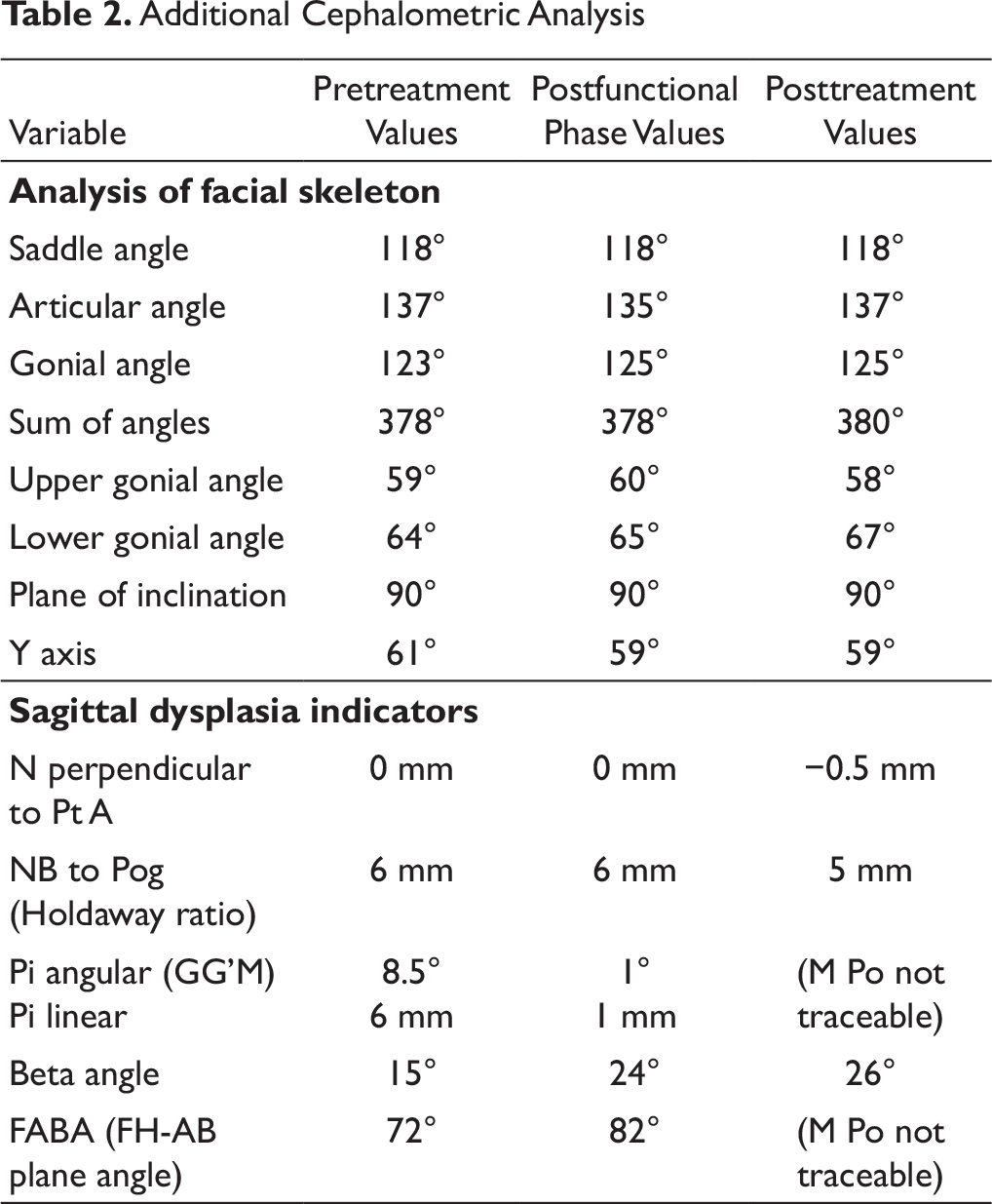
Skeletal correction of the retrognathic mandible was achieved with a drastic improvement in the soft tissues, and increase in the lower anterior facial height was seen cephalometrically in both the postfunctional and posttreatment lateral cephalograms (Figures 10 and 11). There was also good improvement in the macro and micro smile characteristics of the patient (Figure 12). An ideal overjet and overbite was established with a Class I incisal, canine and molar relationship with good buccal intercuspation (Figure 19). The upper and lower dental midlines matched each other and the facial midline (Figure 13). Evaluation of posttreatment panoramic radiograph showed acceptable root parallelism along with normal alveolar bone levels; mutually protected occlusion; and canine guidance on left and right lateral excursions with no working or non-working side interference. The cephalometric changes and comparison between the pretreatment, postfunctional, and posttreatment values are evident in Tables 1 and 2, and the changes in superimposition are seen in Figure 16. The cephalometric values show a remarkable change of 5° in the ANB value. The pretreatment value of the ANB was 8°, and after the growth modulation phase, the ANB value was decreased to 4° and the final post treatment ANB value is 3°. This shows a good amount of correction of the ANB brought about by growth modulation therapy.
End of Phase I—Lateral Cephalogram

Posttreatment Radiographs
Posttreatment Extraoral Photos

Posttreatment Intraoral Photos

Three Years Postretention—Extraoral Photos

Three Years Postretention—Intraoral Photos

Superimpositions
Re-root Canal Done for 36

Pretreatment Models
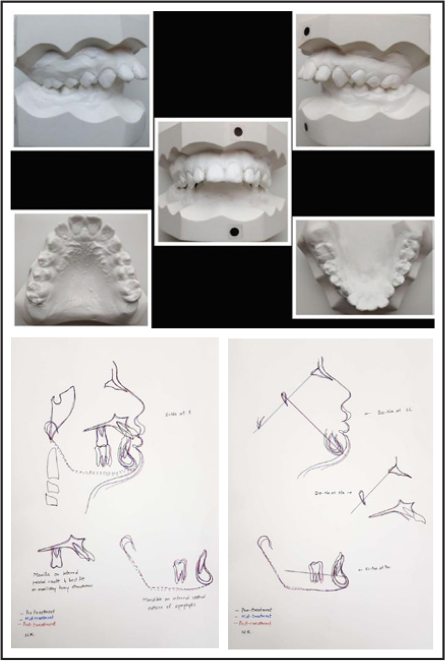
Posttreatment Models

Comparison Between Pretreatment, Postfunctional, and Posttreatment Cephalometric Values
Additional Cephalometric Analysis
Critical Appraisal
NK was successfully treated with two-phase orthodontic therapy over 36 months of active treatment. The original treatment aims were accomplished, and the patient’s chief complaint was addressed. NK was notably pleased with the treatment outcome. A good occlusal and aesthetic result was achieved, and this was reflected in the PAR and IOTN scores. The results were maintained as seen from the 3-year postretention records (Figures 14 and 15).
Records
In all the lateral cephalograms, the orientation of the patient’s head should have been better with respect to the FH plane being parallel to the true horizontal.
Skeletal
As the patient was within the growth potential (CVMI Phase II—acceleration and CS3), the timing of starting the treatment was correct and so skeletal changes were expected. Improvement in the convex profile is observed. There has been a notable improvement in ANB angle by 50° and Wits by 5.5 mm. The treatment duration was increased because the patient took a long time to start the full-time wear of the functional appliance. Also, there was an increase in the lower anterior facial height.
Dental
A good settling of occlusion is seen, and it has remained stable after 3 years posttreatment. However, the following areas could have been improved:
Better root parallelism especially in the upper second premolars and the upper left canine region.
The permanent retainer in the upper arch showed repeated breakages in the region of canines, and hence, it was maintained between the lateral incisors only, after 2.5 years of debonding. This lead to a mild space opening (1 mm) between the upper right lateral incisor and canines. As the patient was reluctant to wear any kind of a removable appliance, composite was used to fill up the 1 mm space between the upper lateral incisor and canine.
The patient was informed about the recurrent caries with the restored lower left first molar and an incompletely obturated root canal on the lower right first molar. However, the patient was adamant that he wanted to get the teeth re-restored only if they turn symptomatic at all. After the root canal-treated tooth turned symptomatic, a re-root canal was done for the same. However, the lower left first molar did not turn symptomatic till 2 years after debonding, and hence, it was restored at that time. The mandibular occlusal photograph does show the restoration being repeated (Figure 17).
LL6 restoration not replaced LL6 re-restoration Root canal done for 36 (At debonding) and coronal coverage done (2 years postretention)
Apart from the abovementioned things, almost all of the Andrews’ six keys to normal occlusion were satisfied in the posttreatment and postretention occlusion.
Soft Tissue
Facial profile was improved and well-balanced at the end of the treatment. Reduction of in-depth mentolabial sulcus is seen.
Three Years Postretention Models

Appliance Design
Adam’s clasps are used instead of Delta clasps as the retentive component of the appliance.
Lower incisal capping could have prevented the lower anterior proclination seen in the postfunctional phase.
Iatrogenic
No change in the interdental bone height or gingival margins was observed. All teeth remained vital at the end of the treatment. Although some amount of attrition of the upper canine cusps is observed in the 3 years postretention records, it can be attributed to the unusually long cuspal contours that the canines had anatomically. This may have led to the attrition despite achieving a harmonious Class I canine relationship.
Conclusion
Considering the severity of the case to begin with, desired result was attained. Harmonious skeletal, dental, and soft-tissue balance was achieved.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.