
Abstract
A 4-year and 10-month old female Pembroke Welsh Corgi presented with an enlarged right popliteal lymph node, and a histopathological diagnosis of nodal marginal zone lymphoma (nMZL) was made. After resection of the lymph node, follow-up observation was continued without chemotherapy. At 22 months after initial presentation, the dog developed enlargement of peripheral lymph nodes, and the histopathological diagnosis was late-stage nMZL. Multidrug chemotherapy induced clinical complete remission, but the tumor relapsed with enlargement of peripheral and abdominal lymph nodes 42 months after initial presentation. Second-round multidrug chemotherapy induced complete clinical remission again; however, the tumor relapsed with lymphadenopathy 47 months after initial presentation. The dog died 59 months after initial presentation, and postmortem examination revealed generalized lymphadenopathy; the histopathological diagnosis was diffuse large B-cell lymphoma (DLBCL). Polymerase chain reaction for antigen receptor gene rearrangements revealed that the nMZL and DLBCL samples were derived from the same B-lymphocyte clone.
Canine nodal marginal zone lymphoma (nMZL) is a type of B-cell lymphoma that originates from the marginal zone of follicles in the lymph nodes. The biological behavior of nMZL is considered indolent or slowly progressive, 16,17 but some cases show aggressive disease courses. 1,4,10,15 Follicular lymphoma (FL) is an uncommon follicle-derived lymphoma that has been reported in lymph nodes of dogs. 16 There is no information on the prognosis or outcome of FL in domestic animals and grading of FL is not routinely performed. 16 Diffuse large B-cell lymphoma (DLBCL) is a high-grade B-cell lymphoma that represents the most common form of nodal lymphoma in dogs. 15,16
In humans, a proportion of nMZL has an unfavorable prognosis, 7,13 and histologic transformation of nMZL to more aggressive lymphoma such as DLBCL is an important risk factor for poor overall survival. 3,11 FL is the most common indolent lymphoma, but transformation of FL to DLBCL is a well-known evolution associated with poor prognosis. 9 In animals, there is a single report of histologic transformation of canine nMZL or FL to DLBCL, 2 while pathological findings have not been documented in detail and clonality analysis was not performed. Here, we report a case of a dog with nMZL that subsequently developed DLBCL. Furthermore, polymerase chain reaction (PCR) for antigen receptor gene rearrangement (PARR) was performed for the clonality analysis of the lymph node tissues at different time points and with different histological features. The aim of this study is to describe the histopathological and immunohistochemical features of a canine case of lymphoma that progressed from nMZL to DLBCL and to elucidate the relatedness of these tumors using PARR.
A 4-year and 10-month old female Pembroke Welsh Corgi was presented with enlarged right popliteal lymph node (World Health Organization [WHO] clinical stage I). 15 The enlarged lymph node was surgically removed and submitted for histopathological examination. The tissue was fixed in 10% neutral-buffered formalin, processed routinely, and 2-μm-thick tissue sections were stained with hematoxylin and eosin. Microscopically, diffuse enlargement of follicular marginal zones with regression of germinal centers was observed in the lymph node (Fig. 1). Enlarged marginal zones comprised intermediate-sized cells with round nuclei (1.5–2 times the diameter of a red blood cell [RBC]), with parachromatin clearing and prominent central nucleoli (Fig. 2). The lesion was diagnosed as nMZL. After resection of the lymph node, follow-up observation was continued without chemotherapy.
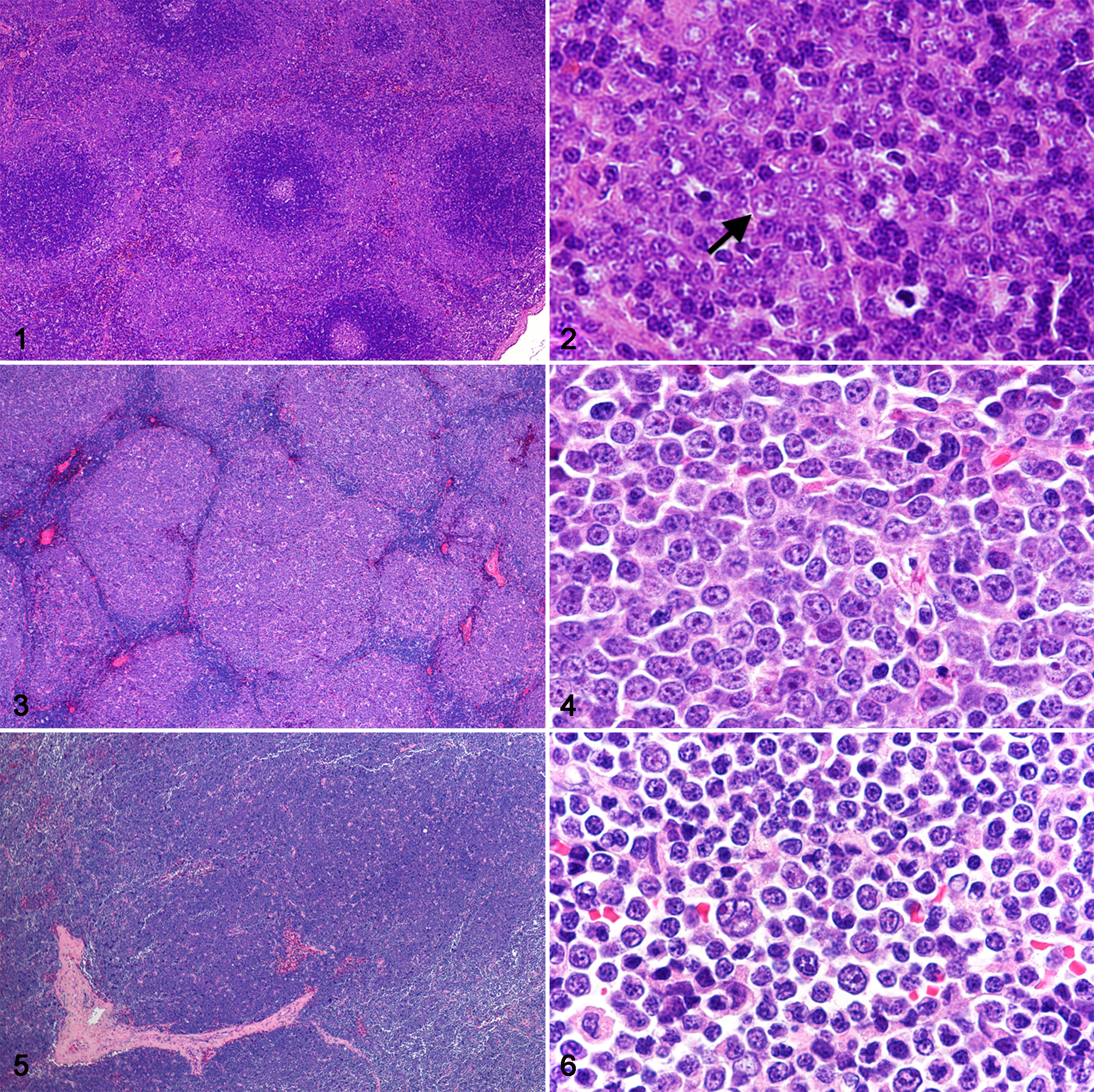
Twenty-two months after initial presentation (6-year 8-month old), the dog was presented with enlargement of the right mandibular, right inguinal and left popliteal lymph nodes (WHO clinical stage II). 15 Fine-needle aspiration of the enlarged lymph nodes revealed increased immature-appearing lymphocytes with a large nucleus with fine chromatin pattern, indicating the relapse of lymphoma. Histologically, the surgically removed right mandibular lymph node was effaced with numerous nodular expansions (Fig. 3). Mantle zones and paracortical zones were compressed between nodules. The nodules were mainly composed of intermediate-sized cells with round nuclei (2 times the diameter of a RBC), with prominent central nucleoli or multiple peripheral nucleoli, and were accompanied by few centrocytes (Fig. 4). The lesion was diagnosed as late-stage nMZL with nodular patterns, but the differential diagnosis included FL. L-CHOP-based multidrug chemotherapy (L-asparaginase, cyclophosphamide, doxorubicin [hydroxydaunorubichin], vincristine [oncovin], and prednisolone) 6 induced clinical complete remission. However, the tumor relapsed with enlargement of hepatic portal, mesenteric, and right inguinal lymph nodes on clinical examination 42 months after initial presentation. Second-round CHOP-based chemotherapy (doxorubicin was replaced with mitoxantrone after 5 doses of doxorubicin) induced complete clinical remission; however, the tumor relapsed again with systemic lymphadenopathy 47 months after initial presentation. By ultrasonography, many nodules were detected in the liver and spleen 55 months after initial presentation. Thereafter, the dog responded to several rescue chemotherapies such as lomustine + L-asparaginase protocol 14 and temozolomide + dactinomycin protocol, 5 but gradually became resistant to all chemotherapeutic agents used.
The dog died 59 months after initial presentation (9-year 9-month old). Gross postmortem examination revealed generalized lymphadenopathy including retropharyngeal, superficial cervical, axillary, mediastinal, gastric, hepatic, pancreaticoduodenal, and lumbar aortic lymph nodes. Small dark red nodules were observed in the spleen, and small white spots were scattered in the lung and the liver. A thrombus was present in the right ventricle of the heart. There were no significant gross lesions in other visceral organs. Tissues from visceral organs and lymph nodes were fixed in 10% neutral-buffered formalin and processed routinely.
In sections of all lymph nodes, diffuse expansion of neoplastic lymphoid cells replaced the tissue (Fig. 5). Neoplastic lymphoid cells were variably sized with irregular large nuclei (2–4 times the diameter of an RBC) and multiple nucleoli or single central nucleoli (Fig. 6). Apoptotic figures were frequent and atypical mitotic figures were occasionally found. The mitotic count was 8 per 10 high-power fields. Tumor cells was also found in spleen, bone marrow, liver, and kidney. In the heart, fibrinoid necrosis of the vascular walls and multifocal myocardial necrosis were observed. Based on the aforementioned findings, a diagnosis of disseminated DLBCL (WHO clinical stage V) 15 was made.
Immunohistochemistry was performed using the Dako Envision+ System (Dako, Tokyo, Japan) as summarized in Supplemental Table S1. The tumor cells of the initial biopsy (right popliteal lymph node, nMZL) were immunopositive for CD20 and immunonegative for CD3. Other immunohistochemical staining of the initial biopsy was not performed. The tumor cells of the second biopsy (right mandibular lymph node, late-stage nMZL) were immunopositive for CD20, CD79a, and Bcl-2(Fig. 7a and b), and immunonegative for CD3. Nuclear labeling for p53 was present in 1 per 100 cells (1%; Supplemental Figure S1). The percentage of Ki67-positive cells was 27% (27 per 100 cells). The tumor cells of the necropsy sample (hepatic lymph node, DLBCL) were immunopositive for CD20, CD79a, and Bcl-2 and immunonegative for CD3. The nuclear labeling for p53 was present in 30 per 100 cells (30%; Supplemental Figure S2). The percentage of Ki67-positive cells was 39% (39 per 100 cells).
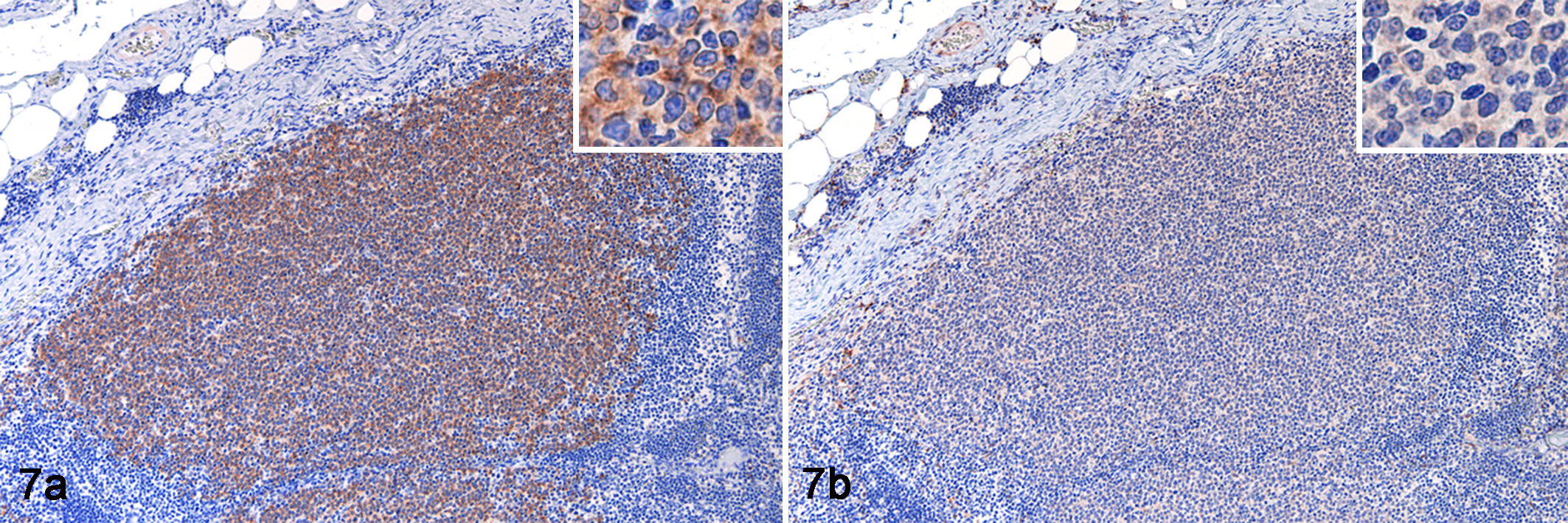
Late-stage nodal marginal zone lymphoma, right mandibular lymph node, dog. Immunohistochemistry for CD79a (a) and Bcl-2 (b).
For clonality analysis, DNA was extracted from the paraffin sections of the initial biopsy (right popliteal lymph node, nMZL), the second biopsy (right mandibular lymph node, late-stage nMZL), and the necropsy sample (superficial cervical and hepatic lymph node, DLBCL; QIAamp DNA FFPE tissue kit, Qiagen, Valencia, CA). PARR assay was performed to detect immunoglobulin heavy chain gene and T-cell receptor gene rearrangement as described previously. 8 PCR was performed in duplicate. In all 4 lymph node samples, the PARR assay showed a single peak with immunoglobulin heavy chain primers, but not with T-cell receptor gamma chain primers. On electrophoresis to visualize the results of PARR, monoclonal cell populations in the lymph nodes were characterized by an identical distinct peak at 86 base pairs of the immunoglobulin heavy chain gene. Sequence analysis of DNA extracted from each band revealed an identical sequence of the complementarity determining region-3 (CDR3) in all the tumors (nMZL, late-stage nMZL, and DLBCL; Supplemental Figure S3).
Our results of histopathologic and genetic examinations indicate the progression of nMZL to DLBCL from a single clone. Two different scenarios are conceivable during progression of an indolent B-cell lymphoma to an aggressive lymphoma. A specific neoplastic clone may undergo multiple and sequential mutations, leading to less differentiated neoplastic cells with a more aggressive behavior. Another possibility is that a different clone from the original tumor may develop another tumor and replace the original tumor. 12 Hence, clonality assessment is required for distinguishing tumors arising from the same clone and tumors arising from different clones. 9 The present study provided genetic evidence for evolution of morphologically distinct B-cell lymphomas from the same clone.
Canine nMZL has been classically considered an indolent disease that often occurs in a single enlarged lymph node and has a distinctive cytological appearance characterized by nuclei of intermediate size with prominent single central nucleoli. 16,17 However, generalized lymphadenopathy at initial presentation, diffuse growth pattern and the presence of centroblasts and immunoblasts in neoplastic tissues, and poor clinical outcome have recently been reported in dogs with late-stage nMZL. 4 In the present case, generalized lymphadenopathy at initial presentation and diffuse growth pattern were not observed, and the neoplastic tissues were mainly composed of intermediate-sized tumor cells. In canine splenic MZL, the spleen is usually the only site involved and splenic MZL holds a good prognosis by splenectomy. 17,20 The present dog survived 59 months (nearly 5 years) after initial diagnosis and resection of affected lymph node, and this was significantly longer than the median survival previously reported in dogs diagnosed with nodal or splenic MZL. 15 Collectively, the present case showed a slow progression from nMZL (WHO clinical stage I) into DLBCL (WHO clinical stage V).
The late-stage nMZL (second biopsy) of the present case showed a nodular growth pattern of tumor cells resembling FL. However, to our knowledge, the progression of nMZL into FL has not been reported in humans and animals. In human patients, some FLs grow in a marginal zone pattern resembling nMZL and some nMZLs show follicular colonization that can resemble FL. 19 In the present study, the late-stage nMZL retained the same cellular characteristics as the earlier stage nMZL, and both tumors were composed of intermediate-sized cells, whereas FL has variable proportions of centroblasts and centrocytes. 16 The late-stage nMZL cells of the present case were immunopositive for pan-B cell markers including CD20 and CD79a, and also Bcl-2 positive, which is consistent with the immunophenotype of human nMZL. 19 Based on these results, the diagnosis of FL was excluded in the present case. Also, the tumor cells of DLBCL (at necropsy) had the same immunophenotype of the late-stage nMZL. The immunophenotype of the tumor cells and the results of DNA sequence analysis indicate that nMZL and DLBCL in the present study were derived from the same clone.
Transformation to DLBCL is associated with a significantly worse survival in both nMZL and FL in humans, but nMZL less frequently shows transformation to DLBCL in comparison to FL. 18 Genetic mutations underlying histologic transformation of nMZL to DLBCL have not been well documented. The present case had increased nuclear Ki67 and p53 immunolabeling in the DLBCL compared to the late-stage nMZL, which may be associated with the multidrug chemotherapy. There are 2 possibilities about this evolution of the neoplastic clone: (1) a resistant subclone with p53 mutation survived the chemotherapy and showed high positivity of Ki67; (2) a specific subclone survived the chemotherapy and subsequently gained p53 mutation. Further studies including the identification of mutations contributing to chemotherapy resistance are needed.
In animals, progression from low-grade B-cell lymphoma to high-grade B-cell lymphoma has been suspected but rarely confirmed. This case confirms that nMZL may progress to DLBCL in the dog, with clonal identity in this instance indicating progression of the same clone. Moreover, the present study shows the morphologic diversity of nMZL. Further molecular studies are needed in order to elucidate the different pathomechanisms of these B-cell lymphomas.
Supplemental Material
Supplemental Material, Combined_supplemental_materials-Shiga_et_al - Long-Term Observation of the Progression From Nodal Marginal Zone Lymphoma to Diffuse Large B-Cell Lymphoma in a Dog
Supplemental Material, Combined_supplemental_materials-Shiga_et_al for Long-Term Observation of the Progression From Nodal Marginal Zone Lymphoma to Diffuse Large B-Cell Lymphoma in a Dog by Takanori Shiga, James K. Chambers, Mei Sugawara, Yuko Goto-Koshino, Hajime Tsujimoto, Hiroyuki Nakayama and Kazuyuki Uchida in Veterinary Pathology
Footnotes
Acknowledgement
We thank Dr. Kenmi Morita (Morita Animal Medical Center) for taking lymph node biopsy samples and monitoring of the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.