
Abstract
Hemangiosarcoma is a common neoplasm of the spleen in older dogs. However, diagnosis is complicated by necrosis and hemorrhage, which can mimic a number of benign processes. Currently, there is no consensus about the number of sections pathologists should examine to rule out hemangiosarcoma. To answer this question, we examined 413 histopathologic sections from 50 cases of canine hemangiosarcoma (mean: 8.1 sections per case; range, 5–14). Each section had the presence or absence of hemangiosarcoma determined by 2 board-certified anatomic pathologists. Then, 100 Monte Carlo simulations were performed, randomly selecting sections from each case 10 000 times and the results averaged. These simulations suggest that examination of 5 sections from a spleen with hemangiosarcoma yields a 95.02% chance of diagnosing hemangiosarcoma, while examination of 10 sections yields a 98.59% chance of diagnosis when hemangiosarcoma is in fact present. The data emphasize the need to submit the entire spleen for histopathologic examination in suspected cases of hemangiosarcoma and suggest that 5 sections obtained by a trained individual are likely sufficient for diagnosis.
Hemangiosarcoma (HSA) is the most common splenic neoplasm of dogs. 4,5,9 Frequently, HSA presents as a large, cavitated, ruptured mass with secondary hemoabdomen and carries a relatively short median survival time. These characteristics differentiate HSA ultrasonographically and visually from other neoplasms, including lymphosarcoma and histiocytic sarcoma. However, several benign splenic conditions, including splenic rupture, hemangioma, and hematoma, can have similar clinical presentations. Differentiating these diagnoses is of primary clinical importance, as HSA has a dramatically different prognosis than the benign conditions. Rupture, hematoma, and hemangioma can be cured by surgical excision, while HSA has a median survival time of 1 to 3 months after treatment with splenectomy alone. 1,10,11
The reported incidence of HSA in dogs with splenic masses is highly variable, depending on the study population examined. For example, a study examining insurance claims from the United Kingdom found 24 of 100 000 dogs per year were diagnosed with HSA. 3 One survey of all splenic masses in dogs found 30 of 65 (46%) with hemangiosarcoma, 7 while another study examining nonruptured incidental splenic masses found 18 of 105 (17%). 2 Finally, a study examining dogs presenting with anemia and hemoabdomen that required transfusion with a concurrent splenic mass found that 54 of 71 (76%) had malignant neoplasms, and 50 of 54 (92%) were HSA. 5
Due to the relatively narrow criteria of some of the studies that resulted in high incidences, many clinicians expect a malignant diagnosis with splenic tumors, especially when masses have ruptured or with concurrent hemoabdomen. When the diagnosis reported is benign, the question of a false-negative diagnosis arises. One study found that 13% of animals diagnosed with benign splenic masses go on to develop subsequent HSA. 8 One possible explanation for the misdiagnoses is that overlying many malignant tumors is a large, often ruptured, hematoma. If the splenic tissue is not properly sampled, the malignancy may be missed and hematoma diagnosed. The expectation of relatively high misdiagnosis often leads to requests for examination of additional sections to increase the diagnostic confidence in guiding owners with further treatment. This uncertainty of the clinician is compounded by the fact that there is no consensus number of sections required by the pathology community to feel confident in the absence of a malignancy and for a confident diagnosis of a benign entity. With no standard, the level of comfort with the number of examined sections between clinicians and pathologists can vary markedly, leading to additional section requests. The uncertainty of how many sections are necessary to rule out malignancy may cause anxiety for both the clinician and the pathologist. Are more sections always better? There must be some limit to the time and expense in ruling out a malignancy and confirmation of a benign diagnosis.
To determine the number of sections of spleen necessary to diagnose HSA with 95% confidence, we looked at a number of archival cases and evaluated the chance of diagnosing HSA, when present, by examining a variable number of sections. Specifically, Monte Carlo simulations 6 were used to generate a probability distribution from the limited case set. These data will ultimately provide better guidance to pathologists in diagnosis and allow for increased confidence in diagnoses for clinicians.
Materials and Methods
Fifty cases were selected from the University of Florida College of Veterinary Medicine Anatomic Pathology archive by searching case records for dogs diagnosed with splenic HSA. Only cases with whole spleens that were sampled by trained personnel (residents and pathologists) were included in this study. Residents were trained to trim sections from the interface of the mass and normal tissue first, then take representative sections of the rest of the spleen. Cases with fewer than 5 slides were excluded to avoid cases that would not meet the criterion listed above. All slides were routinely processed, sectioned, and stained with hematoxylin and eosin. Sections were numbered starting with the first slide and increasing sequentially; if a slide contained multiple sections, the sections were numbered from left to right, with the label oriented to the left. All slides were reviewed by 2 board-certified anatomic pathologists (A.W.S. and M.J.D.), first individually and then in tandem, and scored for the presence (1) or absence (0) of HSA. Specifically, samples were only scored as positive for HSA when both pathologists agreed they would make a definitive diagnosis of HSA from that individual section; sections that were only suspicious for HSA were scored as negative (to be as conservative as possible). These data were entered into an Excel spreadsheet (Excel version 15.35; Microsoft Corporation, Redmond, WA). A custom Visual Basic for Applications program was used to perform the Monte Carlo simulation. Briefly, for each round of the simulation, sections were randomly selected from each case until a section containing HSA was selected. Sections could be chosen more than once with no upper limit during each round to allow for all possibilities associated with analyzing randomly selected sections from a spleen having a specific probability of yielding a positive section. The individual probabilities were the fractions of positive slides obtained from the corresponding spleens. The number of sections selected during the simulation was then recorded as the result. For each simulation, 10 000 rounds were performed. A total of 100 simulations were performed to verify consistency within the model, simulating a total of 50 000 000 cases. The mean, minimum, maximum, and standard deviation of cases where a diagnosis was missed for the 100 simulations were calculated in Excel. Data were graphed using gnuplot (version 5, patchlevel 6).
Results
Medical records review and initial slide screening yielded 50 cases from dogs with a diagnosis of splenic HSA that had at least 5 histologic sections per case. The total number of sections per case ranged from 5 to 14 (mean, 8.12). There were 413 total sections and 279 sections containing HSA (67.55%). The percentage of sections in each case that were positive for HSA ranged from 11.1% to 100%. Twelve of the 50 cases contained HSA in all of the sections evaluated. All simulations for these cases produced a positive result on the first section as the assumed underlying probability of obtaining a positive section is 1.0.
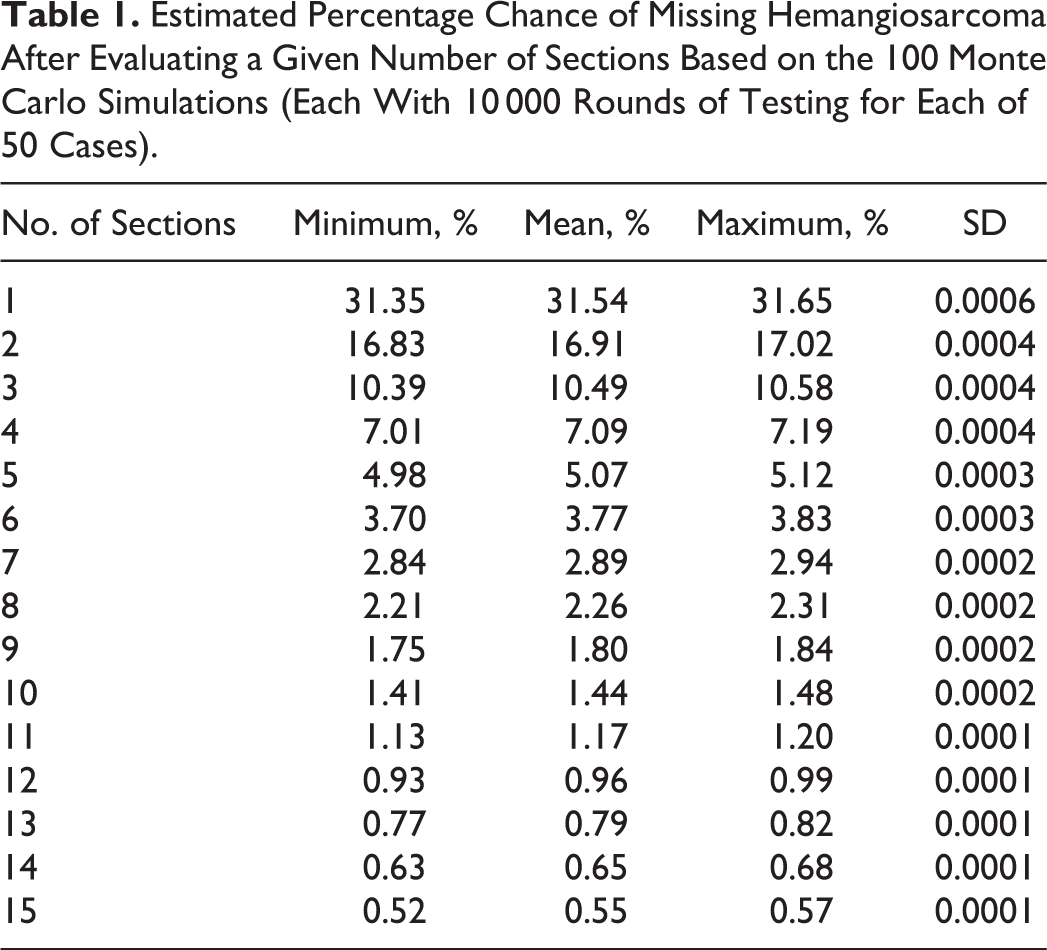
Table 1 shows the results for the calculated probability of missing HSA given the number of sections examined for the 100 simulation runs. Of interest, examination of 5 sections in any given case resulted in a greater than 95% chance of diagnosing HSA, while 10 sections gave a greater than 98% chance. Figure 1 compares the percentage of HSA diagnoses missed by number of sections in the actual cases compared to the simulated cases. Actual cases are defined by the pathologists’ examination of the actual sections, beginning with section 1 and reading through sections sequentially until all sections are evaluated. Actual cases are more efficient in diagnosing HSA, as the simulation results slightly overestimate the number of sections needed for diagnosis (analyzed in the Discussion below). Table 2 shows the number of positive sections out of the total number of sections in the actual cases.
Estimated Percentage Chance of Missing Hemangiosarcoma After Evaluating a Given Number of Sections Based on the 100 Monte Carlo Simulations (Each With 10 000 Rounds of Testing for Each of 50 Cases).
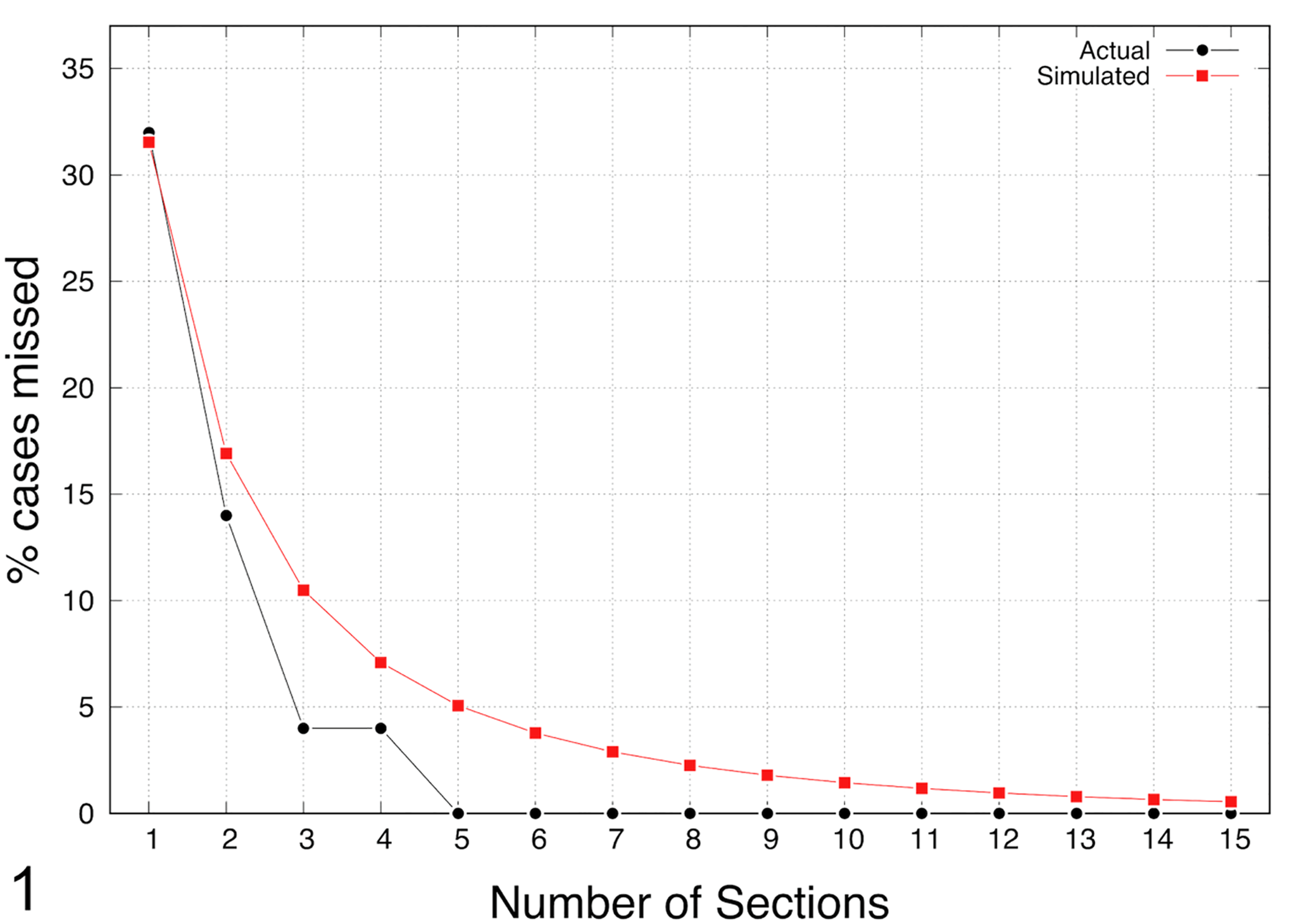
Percentage of simulated or actual cases with false-negative diagnoses based on the number of sections examined. In the simulation, for each test, sections were randomly selected from a case until a section containing hemangiosarcoma was selected (sections could be chosen more than once with no upper limit during each test). The result is the number of sections needed for a diagnosis. The average across 100 simulations of 10 000 runs of 50 cases is presented. Actual cases are the diagnoses on each slide by the pathologists, beginning with section 1 and reading through the sections sequentially until all sections were evaluated.
Case Set Data Showing the Percentage of Cases Diagnosed With Hemangiosarcoma (HSA) in Each Given Section.a
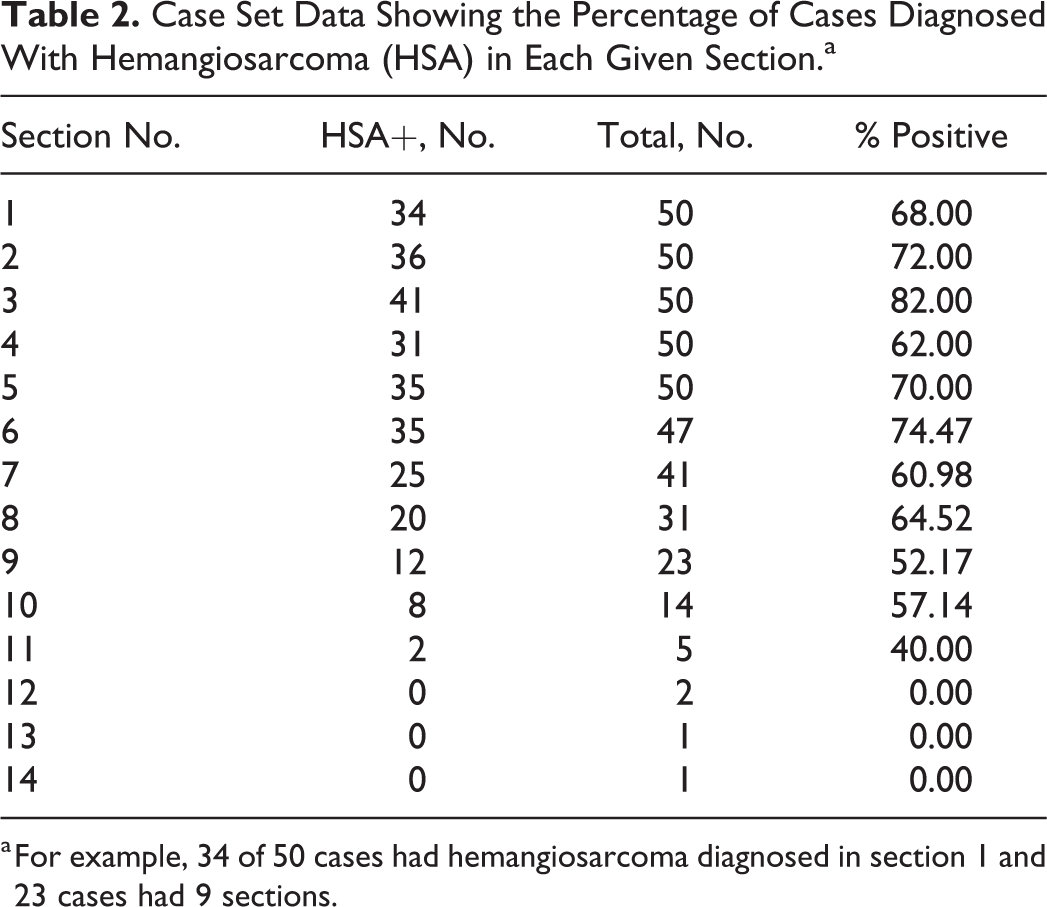
a For example, 34 of 50 cases had hemangiosarcoma diagnosed in section 1 and 23 cases had 9 sections.
Discussion
At the outset of the discussion, it is important to note the limitations of this study. First, all cases in this study, by necessity, were diagnosed with HSA. By definition, cases with diagnoses other than HSA would never be positive. A huge number of sections could be sampled from any spleen, either with or without HSA, that could result in a negative diagnosis; however, the cases included in this study were sectioned by individuals trained to select sections most likely to contain tumor. This study cannot, therefore, determine the number of sections needed to prevent putative false negatives as discussed in the study by Patten et al. 8
Second, our method of testing uses random selection from the entire pool of sections for a case. This presumes that each section is equally likely to contain HSA. In practice, this is not always true. As noted above, when trimming tissues, pathologists attempt to select sections that are most likely to yield evidence of neoplasia first, usually reserving sections of more normal tissue to the end. This trend is borne out by our data in that the first sections from the cases were most likely to be positive for HSA (68% for section 1, 70% for section 2, and 82% for section 3). To be conservative, the simulation assumes all sections have the average rate of 69.45%, as the rate for each case is determined by the associated fraction of positive sections. Hence, the simulation results are conservative and tend to overstate the probability of requiring more than a specific number of sections to detect HSA.
Even with these limitations, this study suggests a number of interesting findings. First, it suggests that examination of 5 sections is likely sufficient to diagnose HSA in a spleen, while increasing the number of sections to 10 only increases the likelihood of diagnosis by a small margin. It also indicates that the likelihood of making a diagnosis in HSA-positive cases decreases with each additional section examined. This seems logical, as the longer you have to look for the tumor, the less likely it is to be present.
This study also highlights the desirability of sending the entire spleen for pathology review after a splenectomy. Given that this study suggests that 5 representative sections sampled by a trained individual are needed to have a 95% confidence level that additional sections will not yield a positive diagnosis, sufficient spleen must be sent to allow these sections to be obtained.
This study also emphasizes the utility of Monte Carlo simulations for relatively limited data sets, as are common in veterinary medicine. While this study, as for any study, would be more robust with a larger number of actual cases, the computer is able to extrapolate our data set to simulate a group of 50 million cases in 100 replicates of 500 000 in less than an hour. While these data reflect the binomial distribution [(1 – p) k ] (where p is the probability of a given outcome and k is the binomial coefficient, the number of successes), the simulation approach is preferred to verify the applicability of the distribution as it is based on actual data.
Finally, while this study provides useful data, a follow-up study would be useful to examine spleens from cases diagnosed as benign that went on to develop HSA and determine the number of sections needed to find the neoplasm in the spleen. This would both confirm that HSA was, in fact, present in the spleen (rather than a de novo mass or metastasis from another site) and determine the number of sections needed to discover this fact. However, to our knowledge, none of the patients in our study set developed further HSA lesions, preventing the comparison with this data set.
Based on these data, we advise submitting the entire spleen for histopathology and obtaining a minimum of 5 representative sections to rule out HSA. These data also suggest that clinicians should have a high degree of confidence in benign diagnoses; out of the 50 actual cases we examined, none would have been falsely diagnosed as benign if 5 or more sections were examined.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.