
Abstract
Intravascular lymphoma (IVL) is a rare angiotropic large-cell lymphoma in which neoplastic lymphocytes proliferate within the lumina of small blood vessels in the absence of a primary extravascular mass or leukemia. This study included 10 cases of canine IVL restricted to the CNS. Dogs had an average age of 8 years and neurological signs mainly referred to brain involvement such as depression, seizures, and ambulatory deficits. Gross examination at necropsy showed focal extensive or multiple hemorrhagic areas mainly distributed in the telencephalon and diencephalon. Histopathologically, numerous veins and capillaries were filled with neoplastic lymphoid cells, accompanied by edema, hemorrhage, and thrombosis. Immunohistochemistry (IHC) for CD3, CD20, and PAX5 was performed to phenotype the neoplastic lymphocytes. IHC for CD44 and CD29 were used to investigate the pathogenetic mechanism leading to the intravascular aggregation of the neoplastic lymphocytes. The same IHC panel was applied to 8 cases of primary and metastatic canine CNS lymphoma in order to compare IVL immunoreactivity. Three IVLs were typified as T-cell, 3 as B-cell, and 4 as non-T non-B. Neoplastic lymphocytes showed marked expression of CD44 in all IVL cases, and CD29-immunolabeled cells were observed in 4 IVLs. CD44 immunoreactivity was consistent with the findings reported in human IVL, suggesting a predisposition to the formation of lymphocyte aggregates. CD29 was inconsistently immunonegative in canine IVL, confirming only partially the pathogenetic mechanism suggested for the human counterpart.
Intravascular lymphoma (IVL) is a rare angiotropic large-cell lymphoma characterized by the proliferation of neoplastic lymphocytes within the lumina of small blood vessels. 11 In dogs, clinical signs are usually not specific, but CNS dysfunction is often the presenting problem due to primary brain or spinal cord involvement. 3,9 The pathogenesis of human IVL is still not completely understood. 2 Abnormalities in molecules known to be involved in lymphocyte and endothelial adhesion have been proposed as directly involved in the predilection for intravascular proliferation of neoplastic cells. 13
The purpose of this study was to describe and characterize the neuropathological features of 10 cases of canine IVL involving the CNS. The immunophenotype and pathogenetic mechanism leading to the intravascular distribution pattern in canine cerebral IVL were also investigated.
A search of the histopathological records and formalin-fixed paraffin wax-embedded tissue archive of the last 10 years was performed. Ten cases of canine cerebral IVL were included on the histological evidence of intravascular proliferation of neoplastic lymphocytes combined with the absence of a primary extravascular mass. In one case the histopathological record also reported involvement of the lungs.
All dogs had undergone a brain magnetic resonance imaging (MRI) at the time of the onset of neurological signs using a 0.25 Tesla magnet (VetMR Grande®, Esaote, Genoa, Italy) before and after contrast administration of gadolinium (Magnevist; 0.15 mmol/kg). All MRI results were collected. Two dogs died spontaneously, and for all the other dogs, owners elected euthanasia because of poor prognosis and progressive worsening of the neurological condition.
A complete necropsy was performed in all dogs and the whole CNS and representative samples of major organs were fixed in phosphate-buffered 10% formalin solution. Transverse sections of the brain and other tissue samples were routinely processed for histology and 4 µm sections were stained with hematoxylin and eosin (HE), Luxol fast blue (LFB), and Perls’s iron stain method and examined by light microscopy. Selected brain sections were also immunolabeled with antibodies against CD3, CD20, PAX5, CD44, CD29, CD68, and S100. The primary antibodies, antigen retrieval methods and the specificity of each antibody are summarized in Supplemental Table S1. The immunoreactivity was detected by the streptavidin-biotin peroxidase method (Streptavidin Peroxidase, ThermoFisher Scientific, Fremont, CA), using 3,3’-diaminobenzidine as chromogen. Eight selected cases of primary and metastatic canine CNS lymphoma were immunolabeled with the same IHC panel to compare IVL immunoreactivity. Negative controls were obtained by omitting the primary antibody. Canine lymph node samples were used as positive controls.
Signalment and neurological signs of the dogs included in our study are summarized in Table 1. Neurolocalization was consistent with intracranial multifocal or diffuse lesions in all dogs. MRI findings consisted of multiple areas of hyperintensity in T2 and FLAIR images mainly located in the telencephalon and in the diencephalon, with almost no significant enhancement after contrast administration. In dog 2, MRI revealed a single ill-defined lesion in the left frontal lobe, mildly hyperintense in T2 and isointense in T1-weighted images and FLAIR sequence, accompanied by leptomeningeal hyperintensity and severe perilesional edema. In dog 3, hyperintense bilateral lesions at the level of the basal nuclei were detected on T2-weighted and FLAIR images (Fig. 1). In dog 4, 2 intraparenchymal lesions involving the left thalamus and the temporo-occipital cortex were evident in the T2-weighted images and FLAIR sequence, characterized by a blurred hyperintensity and no mass effect.
Cases of Canine Cerebral Intravascular Lymphoma.
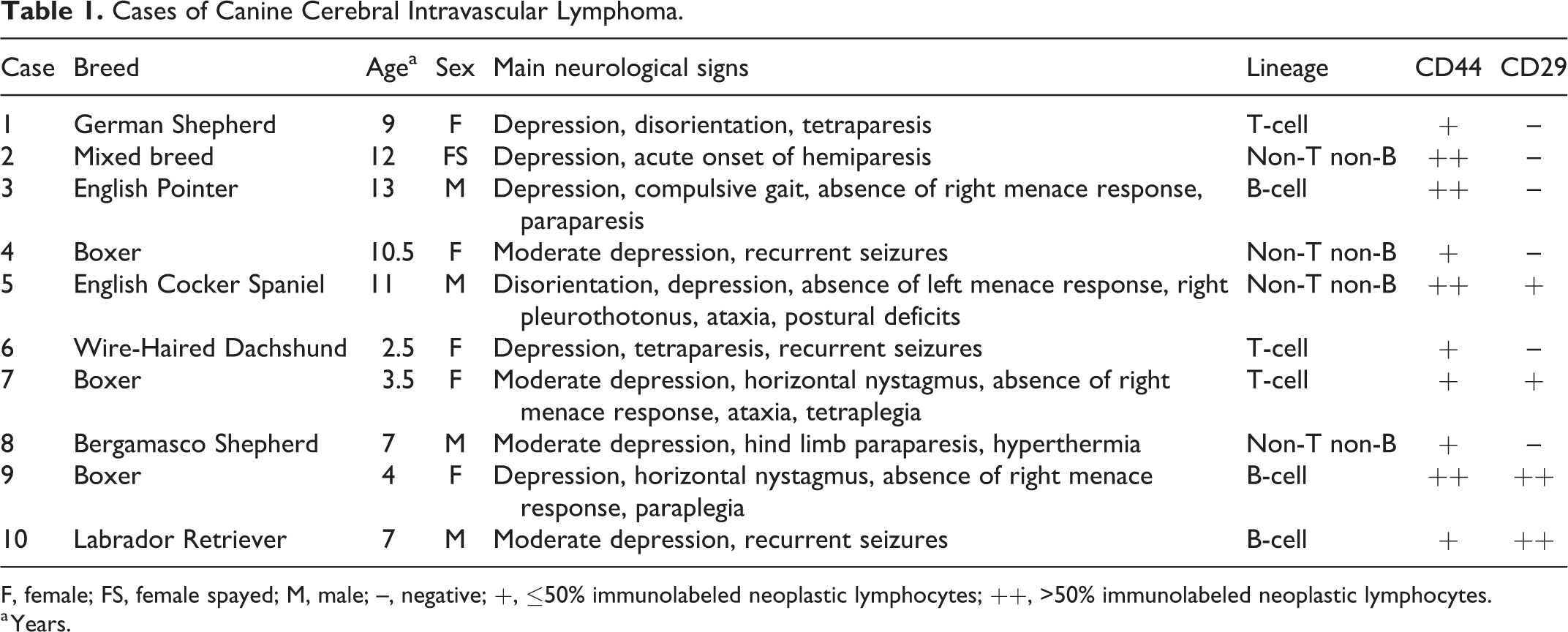
F, female; FS, female spayed; M, male; –, negative; +, ≤50% immunolabeled neoplastic lymphocytes; ++, >50% immunolabeled neoplastic lymphocytes.
a Years.
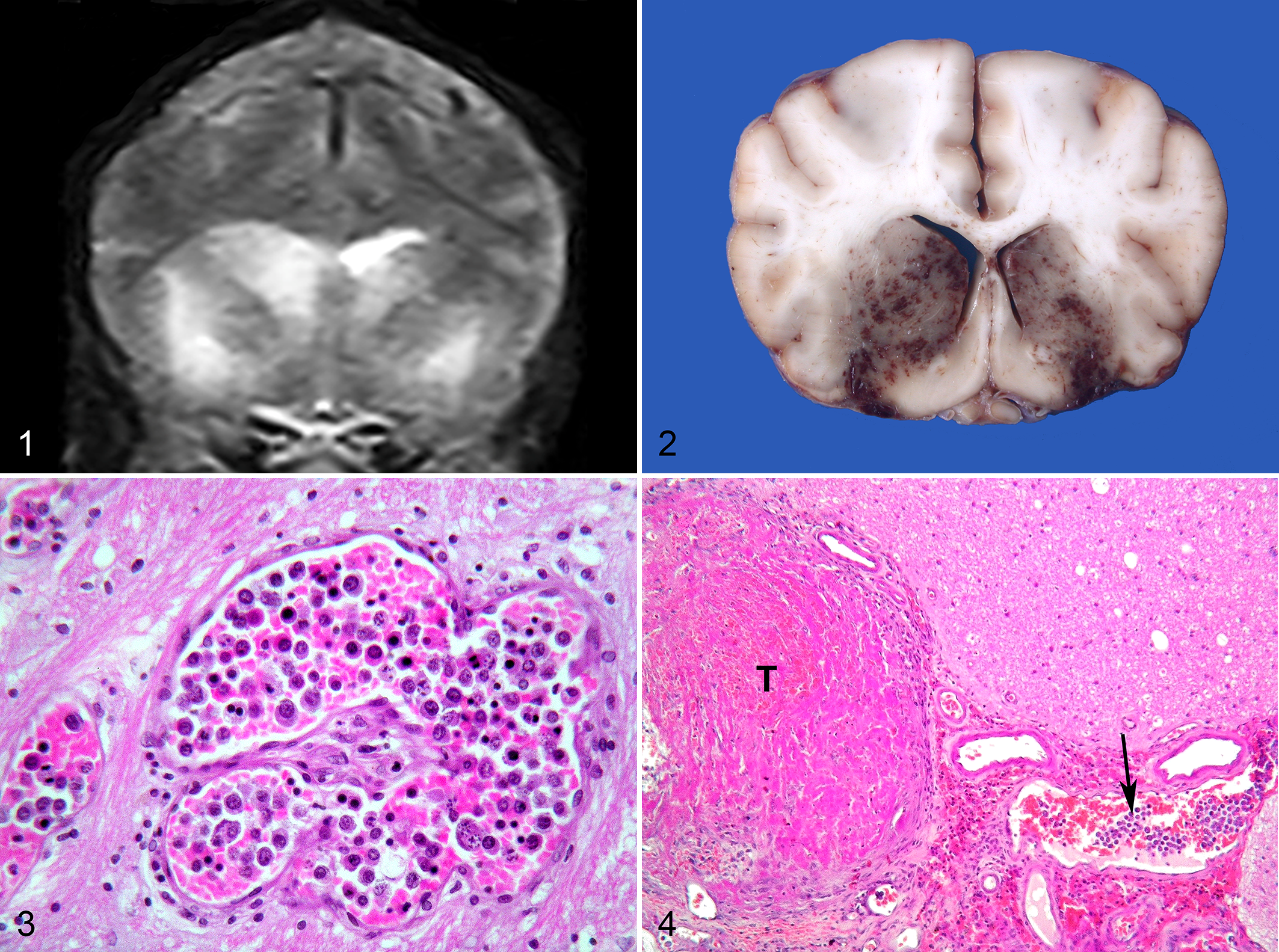
Postmortem examination revealed gross lesions restricted to the CNS in 6 dogs. In 4 dogs (Nos. 2, 3, 4, and 6), macroscopic findings were consistent with multifocal hemorrhagic areas, mainly distributed in the forebrain, sometimes with a bilateral and symmetrical distribution. In dog 2, a locally extensive malacic and hemorrhagic lesion of the left parietal lobe was evident, accompanied by marked perilesional edema and shifting of the midline structures. In dog 3, bilateral and almost symmetrical hemorrhagic necrosis and edema involved the region of basal nuclei (Fig. 2). In dog 4, thalamic and temporo-occipital hemorrhages with mild compression of the mesencephalon were observed. In the other dogs, gross examination of the brain was unremarkable.
Histologically, numerous neuroparenchymal and meningeal vessels appeared filled with neoplastic lymphocytes. Small and medium-sized venules were predominantly involved, while some meningeal arterioles contained fewer neoplastic cells. Neoplastic aggregates tended to entirely occupy the lumen of veins and capillaries, usually centrally with no apparent cohesion with the endothelium. Neoplastic cells were markedly pleomorphic, round to polyhedral, with distinct cell borders and variable nucleus/cytoplasm ratios. Nuclei were voluminous, round to oval, with coarsely clumped chromatin and sometimes indistinct nucleoli. Binucleated cells were occasionally present. Anisocytosis and anisokaryosis were marked and several atypical mitotic figures were evident. Frequently, the neoplastic lymphocytes showed degenerative changes with nuclear pyknosis and karyorrhexis (Fig. 3). Secondary changes included hemorrhagic infarcts due to multifocal partial to complete venous thrombosis comprised of fibrin, neoplastic lymphocytes and non-neoplastic red and white blood cells (Fig. 4). Perivascular hemorrhages and multifocal intraparenchymal hemorrhagic lesions were observed. The neuroparenchyma adjacent to the vessels involved by the intraluminal neoplastic proliferation and the hemorrhagic lesions often contained diffuse edema and, in the most severely affected areas, malacia with presence of foamy macrophages. Occasionally, small perivascular aggregates of small non-neoplastic lymphocytes were present, sometimes accompanied by degeneration and necrosis of the vessels wall. In dog 2, intravascular neoplastic lymphocytes were also found in the lungs. The pulmonary involvement was limited to small caliber pulmonary veins and interstitial capillaries, whereas arteries and larger caliber vessels were spared.
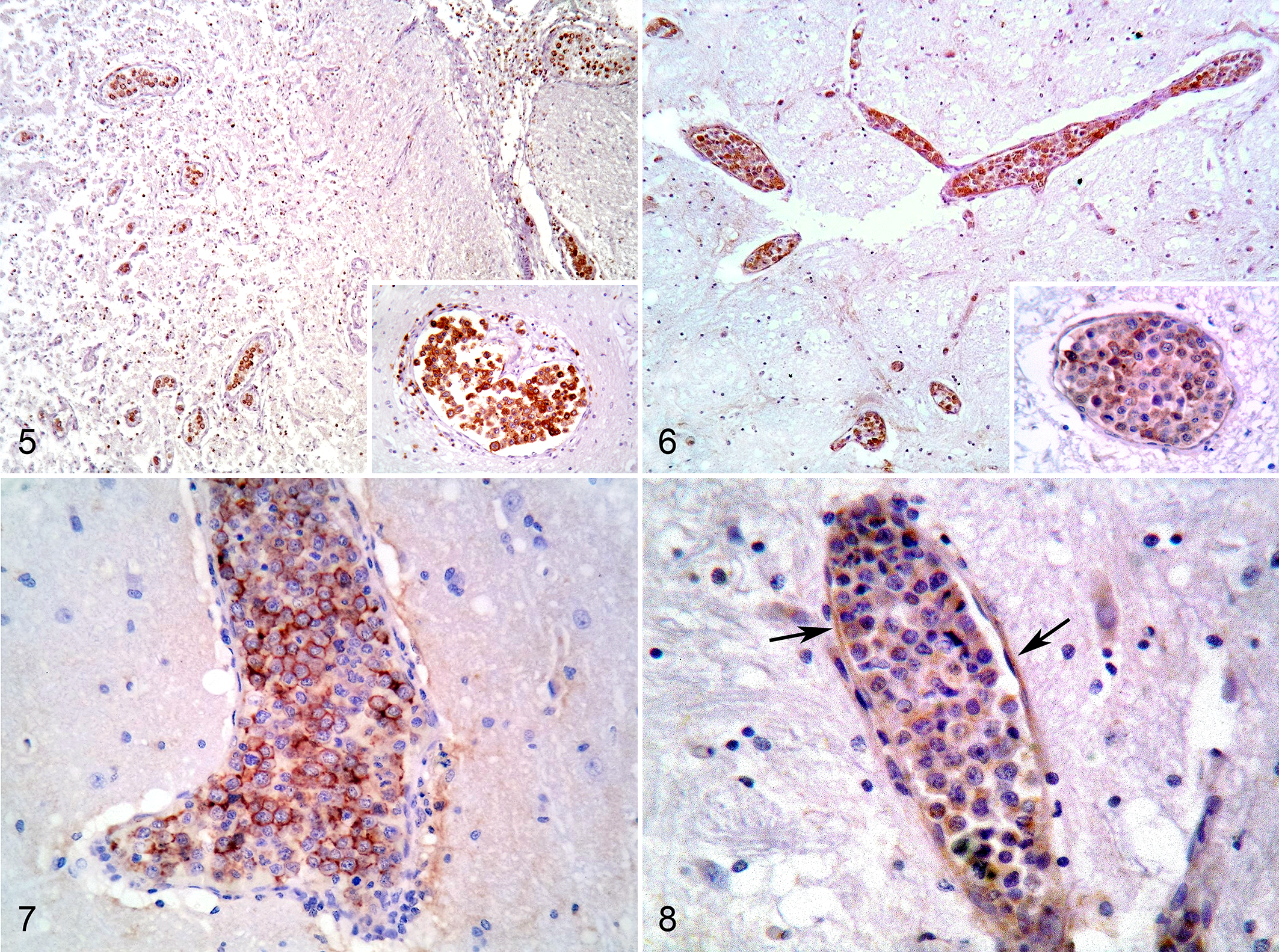
Immunohistochemistry was performed on serial sections to immunophenotype the intravascular neoplastic lymphocytes. In 3 of 10 cases the neoplastic cells were typified as T-cell (CD3+, CD20-, PAX5-), in 3 cases as B-cell (CD20+, PAX5+, CD3-), and in the remaining 4 as non-T non-B (CD3-, CD20-, PAX5-) (Table 1; Figs. 5, 6). CD68 and S100 expression was negative in all cases. In all cases, most intravascular neoplastic lymphocytes showed marked cytoplasmic membranous expression of CD44, whereas the endothelial layer was negative or occasionally very mildly immunolabeled. Immunolabeled cell aggregates were not adherent to the endothelial surface (Fig. 7). Although with different intensity, membranous CD29 expression was observed in 4 IVLs (Nos. 5, 7, 9, 10), accompanied in 2 cases by weak immunolabeling of the cytoplasm (Nos. 9, 10). The endothelium of vessels containing neoplastic lymphocytes was also immunolabeled (Fig. 8), as was the muscular layer of some arterioles.
Regarding the primary and metastatic CNS lymphoma cases, 4 were classified as T-cell, 3 as B-cell, and 1 as non-T non-B. Neoplastic cells expressing CD44 were detected in only 2 cases (Supplemental Fig. S1) and CD29-immunolabeled cells were observed in 1 primary CNS lymphoma (Supplemental Fig. S2). Control tissue samples showed cytoplasmic and membrane immunolabeling of lymphocytes (Supplemental Figs. S3, S4).
IVL is a rare tumor characterized by exclusive or predominant growth of neoplastic cells within the lumina of blood vessels, leading to progressive occlusion followed by thrombosis, hemorrhage, and infarction. 11,14 As in humans, the antemortem diagnosis of canine cerebral IVL is difficult and MR imaging and CSF analysis are inconsistently useful to achieve a definitive diagnosis, although they may suggest it. 3,5,7 MRI is often of limited use because, despite being highly sensitive, it has low specificity. Indeed, the most common appearance consisted of multifocal hyperintensities on T2-weighted and FLAIR images with none to mild and irregular contrast enhancement potentially referable to different conditions such as inflammation, vascular and/or neoplastic nonspecific infiltrative lesions. 3,7
To our knowledge, 24 cases of canine IVL have been reported up to date. When the immunophenotype was identified, T-cell IVL was most prevalent. 3,4,7,9,12 In the cases reported herein, we observed an equal distribution of T-cell and B-cell IVLs, and 4 cases were typified as non-T non-B IVLs. The prevalence of non-T non-B IVLs is similar to that reported in a previous case series. 9 The lineage of these IVLs is uncertain. Loss or rearrangement of cluster of differentiation molecule expression during neoplastic transformation, leading to unsuccessful immunophenotyping, has to be considered. Alternatively, neoplastic lymphocytes might have been natural killer (NK) cells. In dogs, IVLs of NK-cell origin has been reported only in a Labrador Retriever with peripheral blood involvement. 8 Further studies with complementary methods like PCR for antigen receptor rearrangement (PARR) on larger numbers of cases could be helpful to clarify the lineage of canine IVL.
The pathogenesis of IVL resulting in the distinctive proliferation of neoplastic lymphocytes within the vascular lumina is not completely understood. CD44 in human cases was invariably present on the surface of neoplastic cells, 6,10 presumably predisposing to the formation of lymphocyte aggregates. In our canine IVL cases, CD44-expressing neoplastic cells were found in all cases, whereas CD44 expression was detected only in 2 cases of CNS lymphoma. A predilection of cell to cell interactions and aggregation versus cell-matrix interaction could be speculated. Anyway, the functional properties of CD44 should be considered, since the immunohistochemical detection of this molecule does not indicate a proper function. The existence of multiple CD44 isoforms that appear to be differentially expressed on various cell types should be also considered, since these different isoforms might be important in the regulation of IVL growth and dissemination. 1
CD29-expressing neoplastic cells were detected in 4 cases with a weak cytoplasmic immunoreaction in 2 cases, different from the usual membranous localization of this integrin. CD29 immunoreactivity was observed in all lymphocyte lineages. Only 1 primary CNS lymphoma showed less than 50% of CD29-expressing neoplastic cells. The neoplastic transformation of lymphocytes could modulate the binding properties of CD29 or impair the ability of produce adhesion factors such as β1 integrin, although its presence on the cell membrane and cytoplasm was still evident. Different from the lack of CD29 reported in human IVL, 10 this molecule might not be primarily involved in the pathogenesis of canine IVL.
In conclusion, most clinical and biological features of canine IVL are largely unknown. The heterogeneity of the clinical picture and the lack of diagnostic algorithms may explain why definitive diagnosis is made postmortem in almost all cases. The possible contribution of neuroimaging to the in vivo discrimination of brain lesions, as well as the possibility to select regions for brain biopsy could be of help to the antemortem diagnosis and useful to obtain fresh tissue samples. CD44 immunoreactivity suggests a predisposition to the intravascular aggregation of lymphocytes, whereas CD29 expression only partially confirms the pathogenetic mechanism suggested for human IVL. Further studies of the expression of integrins and their ligands in a larger group of cases and with more specific markers may be helpful to define the importance of these molecules in the pathogenesis of canine IVL.
Supplemental Material
Supplemental Material, DS1_VET_10.1177_0300985818806059 - Canine Cerebral Intravascular Lymphoma: Neuropathological and Immunohistochemical Findings
Supplemental Material, DS1_VET_10.1177_0300985818806059 for Canine Cerebral Intravascular Lymphoma: Neuropathological and Immunohistochemical Findings by Sara Degl’Innocenti, Nicola Della Camera, Cristian Falzone, and Carlo Cantile in Veterinary Pathology
Footnotes
Acknowledgements
We thank Mrs Lisa Baroncini for expert technical assistance in histopathology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.