
Abstract
Parosteal osteosarcoma is a rare, slow-growing tumor most commonly arising from the surface of long bones. Tissue or histological sections from 5 dogs and 1 cat with zygomatic arch masses were examined. Clinical presentations varied from chronic sneezing to facial swelling. Imaging consistently demonstrated osseous proliferation in the area of the zygomatic arch. Histologically, the masses were characterized by well-differentiated fibro-osseous and chondroid components that radiated outward from the periosteum of the zygomatic bone. Cellular atypia and mitotic figures were uncommon. Parosteal osteosarcomas have previously been reported in the skulls of dogs and cats, but only 1 has been reported on the zygomatic arch. Initially, these tumors are of low histologic low grade, but with time, they can show more aggressive behavior and invade the underlying bone.
Osteosarcomas are a common malignant tumor in veterinary medicine, accounting for up to 85% of the malignant bone tumors in dogs and approximately 70% in cats. 16 Most osteosarcomas arise within bones, particularly at the metaphyseal region of long bones, and are referred to as central osteosarcoma. 3 A second and much less common type of osteosarcoma originates on the surface of bones, arising from either the osteogenic or fibrous layer of the periosteum, 3 and is referred to as peripheral osteosarcoma. This second group is subcategorized into periosteal osteosarcoma, which may show malignant biological behavior similar to central osteosarcoma, and parosteal osteosarcoma, which is slow growing and less prone to distant metastasis and carries an overall more favorable prognosis than central osteosarcoma. 1,3,11 In humans, the difference in biological activity is emphasized by the 80% 5-year survival time for parosteal osteosarcoma compared to 15% for intraosseous osteosarcoma. 19
Periosteal osteosarcoma originates from the undifferentiated cells of the periosteal osteogenic layer and will cause bony lysis, neoplastic bone formation, secondary reactive bone formation, and invasion into the medullary cavity. 3,11 Parosteal osteosarcoma originates from the fibrous layer of the periosteum. 16 Grossly, they are firm to hard masses with a smooth exterior connected to the surface of the cortex by a sessile or pedunculated base from which they grow outward. 16 Typically, they are well differentiated with irregularly fragmented osseous trabeculae present within a neoplastic spindle-cell stroma that runs in random directions. The cellularity of the spindle cells can vary, but they generally lack pleomorphism and have a low mitotic index and low metastatic potential. 3,13,18 The underlying cortex is generally intact; however, given enough time, they can transform to a more aggressive population with pleomorphism, cellular atypia, and extension into the cortex and medullary canal with metastasis as documented in both the veterinary and human literature. 3,10,11,14,16,18 The histologic appearance is key to differentiating these tumors from others that can also form on the surface of the skull and may have a similar gross appearance. An example is the multilobular tumor of bone, which has a characteristic pattern consisting of multiple circular, oval, or irregularly shaped nodules or islands of cartilaginous, osseous, or osteocartilagenous tissue separated by narrow anastomosing fibrous septae. 3 The fibrous septa create a lobulated pattern in the latter in contrast to the parosteal osteosarcoma, which has a more haphazard stromal alignment without forming discrete nodules. Another example is fibrous dysplasia, which is composed of well-differentiated fibrous tissue containing trabeculae of woven bone that are relatively regularly spaced and sized and lack osteoblasts on the trabecular surface. 11 The orderly arrangement is key for distinguishing it from a parosteal osteosarcoma. The trabeculae of a parosteal osteosarcoma are often covered by spindle cells; however, they can contain a single layer of osteoblasts, 18 as opposed to the trabeculae in fibrous dysplasia. First characterized in humans by Geschickter and Copeland 5 in 1951 as a “parosteal osteoma,” parosteal osteosarcoma has since been recognized in animals, but published reports are rare. 2,8,9,12,15,17,19,20 This report documents 6 cases of parosteal osteosarcoma of the zygomatic arch in 5 dogs and 1 cat.
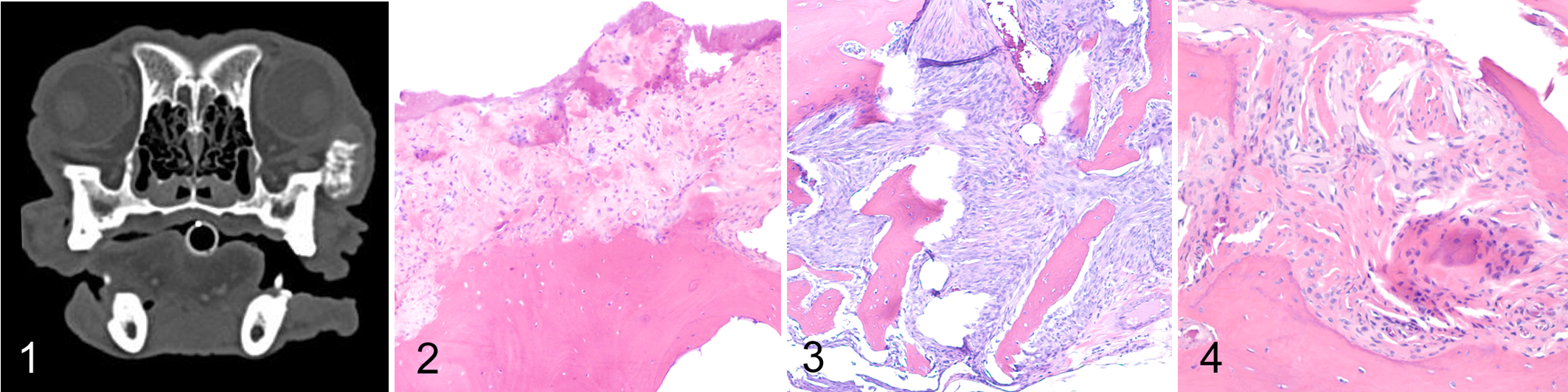
All cases were evaluated by the Osteopathology Service at the Texas A&M Veterinary Medical Teaching Hospital as outpatient sample submissions. The availability of historical and diagnostic imaging findings for certain cases was limited. Signalment and clinical information are listed in Table 1. Overall, the animals ranged from 8 to 14 years old with a mean age of 11; no breed or sex predilection was noted. The gross appearance in these cases consisted of contoured, sessile, osseous proliferations on the zygomatic arch, which corresponded to radiograph (2/6 cases) or computed tomography imaging findings (4/6 cases; Fig. 1). All cases shared similar features. The masses were centered on and appeared to arise from the surface of the zygomatic bone (Fig. 2). In most of these lesions, tumor cells had begun to invade the osteogenic layer and surface of the cortical compacta, similarly to documented cases of human parosteal osteosarcoma (Fig. 2). 10,14,18 The neoplasms were comprised of haphazardly arranged anastomotic trabecular systems of woven bone separated by a moderately cellular fibrovascular network (Figs. 3, 4). Neoplastic cells were spindle to polygonal with angular profiles and often entrapped within their fibrillar matrix (osteoid) (Fig. 4). Mitotic figures were not apparent. Multifocally were solid sheets of neoplastic fibro-osseous tissue having no distinctive pattern. A cartilage cap over the external surface was absent in these masses.
Signalment, Clinical Presentation, and Anatomic Location of Parosteal Osteosarcoma in 5 Dogs and 1 Cat.
Abbreviations: C, castrated; F, female; M, male; S, spayed; U, unknown.
Human parosteal osteosarcoma is largely confined to long bones, 1,4,6,9,13 but animal cases can occur in the skull. 8,9 Other published locations have included the cervical vertebrae in the dog, 15 scapula in the cat, 12 and appendicular skeleton in the dog 2 and the cat. 17,20 Bones of the skull differ from the long bones of the appendicular skeleton both in their embryology and resulting histological appearance. Flat bones of the skull are formed by intramembranous ossification while the long bones are formed by endochondral ossification. 7 The cases presented here were all confined to the zygomatic arch. To the authors’ knowledge, only a single parosteal osteosarcoma of the zygomatic arch has been reported. 19
The use of en bloc resection has only rarely been used for the treatment of intraosseous osteosarcoma because of late recognition of the tumor, local destruction, rates of metastasis, and lack of normal bone after resection. 19 However, parosteal osteosarcoma of the zygomatic arch is well suited for this technique due to the low grade of malignancy and ease of accessibility. In the aforementioned case report, early diagnosis followed by complete resection resulted in a cure. 19 In this case series, 1 of the biopsy specimens was from an animal presenting for regrowth of a previous zygomatic arch osteoma that was removed almost 2 years prior (case 4). It is possible the original mass was actually a parosteal osteosarcoma. This demonstrates that even if complete excision does not occur, slow growth of the mass and benign biological activity still allow for a successful outcome with extension of life.
Parosteal osteosarcoma is a slow-growing neoplasm that manifests as an osseous mass expanding the periosteum and generally sparing the medullary cavity. Many of the cases presented here had cortical invasion, demonstrating the chronicity of the lesions despite an otherwise benign histologic appearance. In humans, parosteal osteosarcoma is found primarily in the distal femur, followed by the proximal tibia and proximal humerus. 6 Animals appear unique in that the skull is also a preferred location. Interestingly, all 6 cases presented here were confined to the zygomatic arch. The reason is unknown, but given the predilection for domestic species to spend long period of time chewing, it may be a functional predisposition whereby localized repeat trauma increases cell turnover and induces cell mutagenesis, warranting further study. The prognosis of paraosteal osteosarcoma is more favorable than central osteosarcoma, as evident by slow growth and a decreased likelihood of metastasis. 2,8,19 As such, surgical intervention may be warranted and successful if early in the clinical course.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.