
Abstract
The authors previously investigated progressive glomerulonephropathy in 2- to 11-year-old common marmosets and characterized age-related changes of the renal glomeruli and development of tubulointerstitial lesions. In this study, immunoglobulin deposition and ultrastructural changes of the glomeruli were investigated in 5 young marmosets from 6 months to 3 years of age with pre-onset or early glomerulonephropathy. In all animals, the foot processes of podocytes were effaced, and IgM was deposited into the glomeruli. In glomeruli without glomerular basement membrane (GBM) alteration, IgM was the only immunoglobulin type deposited in the glomeruli. In cases with more advanced lesions of reticulation and thickening of GBM, IgA and IgG deposits were also observed. Therefore, the authors conclude that IgM may be the primary or earliest immunoglobulin deposited in this nephropathy, whereas IgA and IgG deposition may be connected to the progression of the glomerular lesions. IgM deposition and foot process effacement of podocytes occur early in the life of affected marmosets.
Keywords
The common marmoset (Callithrix jacchus) is a New World primate used for biochemical research, including reproductive, toxicologic, and physiologic studies. 6 Thus, it is important for researchers to be aware of spontaneous histopathologic changes as background lesions to accurately ascertain experimental results. 8 Spontaneous renal lesions of common marmosets are known as progressive or IgM nephropathy. 2 –4 The early stages of nephropathy typically show intratubular hyaline casts and tubular regeneration without histologically visible glomerular changes. 10 Subsequently, the first glomerular lesions occur as a focal increase of mesangial cells and mesangial matrix, particularly in the hilar/extraglomerular area. 4,10 Furthermore, the glomerular lesions expanded globally or segmentally and were accompanied by more severe tubulointerstitial lesions. 6 In a previous report, glomerular lesions were observed in 49 of 122 callitrichids age 4 years and younger, and 54 of 63 callitrichids older than 4 years. 2
We investigated progressive glomerular nephropathy in 2- to 11-year-old common marmosets (C. jacchus) and identified a primary glomerular change in the early stage, with progressive glomerular change in the advanced stage with age. 10 In the early stage of nephropathy in young marmosets, effacement of podocyte foot processes and partial thickening of the glomerular basement membrane (GBM) were observed ultrastructurally, even though no recognizable glomerular lesions were detected by light microscopy. 10 Although the first event of the glomerulonephropathy was thought to be in the podocytes and GBM, electron dense materials (indicating immunoglobulin) had not yet been deposited in the GBM. Some previous reports suggested that the marmoset nephropathy was caused by IgM and IgA deposition because the glomeruli showed IgM or IgA positive deposition, even in a 24-day-old baby marmoset. 2,3 If all marmosets are affected from a young age, characterizing the glomeruli at preonset glomerulonephropathy may clarify the pathogenesis. The objective of the study is to characterize the glomeruli at preonset glomerulonephropathy in young marmosets immunohistochemically and ultrastructurally.
This study was approved by the Institutional Animal Care and Use Committee of Central Institution for Experimental Animals (CIEA; Kawasaki, Japan) and was carried out in strict accordance with the Regulations for Animal Experimentation of the CIEA based on the Guidelines for Proper Conduct of Animal Experiments (Science Council of Japan, 2006). Five common marmosets (2 males and 3 females) from CLEA Japan Inc. (Tokyo, Japan) were evaluated. Ages ranged from 6 months to 3 years at the time of necropsy (Table 1). The animals were housed in cages in an animal room maintained at a temperature of 26 ± 3°C and a humidity of 55 ± 20%. They were provided with CMS-1M diet (CLEA Japan Inc.) and tap water. The animals were euthanized under anesthesia with pentobarbital sodium due to a hindlimb injury (case No. 1), weight loss (case Nos. 2 and 4), curvature of lumbar vertebrae (case No. 3), or mandibular joint dislocation (case No. 5). Urinalysis was not performed because the urine could not be sampled. The entire right kidney was perfused with saline, followed by 4% paraformaldehyde. For transmission electron microscope examination, a part of the cortex was fixed in 2.5% glutaraldehyde. The rest was fixed in 10% neutral-buffered formalin for light microscopic examination. Specimens were fixed in 10% neutral-buffered formalin, embedded in paraffin, sectioned at 5-μm thickness, and stained with hematoxylin and eosin, periodic acid-Schiff, periodic acid-methenamine-silver, and Masson’s trichrome. The lesions were classified by a score of glomerular, tubular, and interstitial lesions according to published templates (Supplemental Table 1). 10 The specimens fixed in 2.5% glutaraldehyde were postfixed in 1% osmium tetroxide for 2 hours, dehydrated, and embedded in Epon, using a conventional method. Ultrathin sections staining with uranyl acetate and lead citrate were prepared and examined under an electron microscope (H-7600; Hitachi High-Technologies, Tokyo, Japan). For immunohistochemistry, the entire left kidney was perfused with saline and then snap-frozen in liquid nitrogen with Tissue-Tek O.C.T. Compound (Sakura Finetek Japan, Tokyo, Japan). Immunohistochemical staining was performed on 5-μm-thick cryostat sections. The following primary antibodies were used: polyclonal rabbit antihuman IgM (1:300), polyclonal rabbit antihuman IgA (1:200), and polyclonal rabbit antihuman IgG (1:500) (DakoCytomation, Glostrup, Denmark). Detection of the immune complexes was performed using polyclonal swine antirabbit immunoglobulins/FITC (1:40) (DakoCytomation). Sections were photographed with a fluorescence microscope (BX51N-34-FL-1-D; Olympus, Tokyo, Japan). The deposition was graded by the criteria as follows: fine granular pattern as grade 1 (+) and coarse granular pattern and/or linear pattern as grade 2 (++).
Light Microscopic, Electron Microscopic, and Immunohistochemical Findings in 5 Young Marmosets in the Early Stages of Progressive Nephropathy.
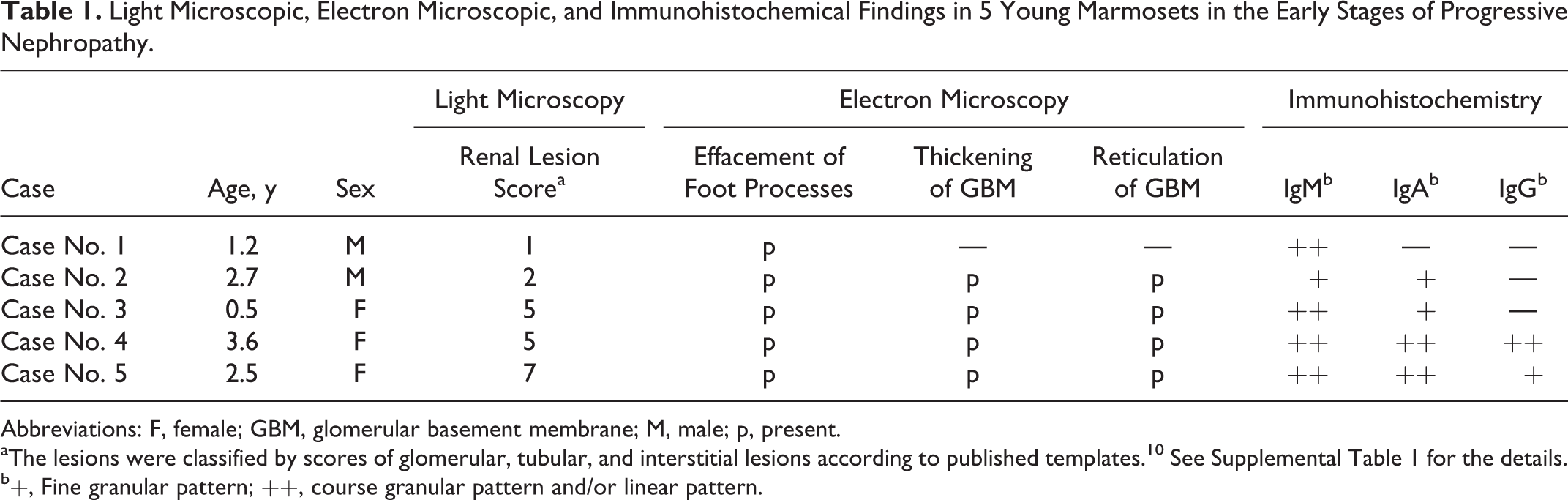
Abbreviations: F, female; GBM, glomerular basement membrane; M, male; p, present.
aThe lesions were classified by scores of glomerular, tubular, and interstitial lesions according to published templates. 10 See Supplemental Table 1 for the details.
b+, Fine granular pattern; ++, course granular pattern and/or linear pattern.
Light microscopic, electron microscopic, and immunohistochemical findings are shown in Table 1. Renal lesion scores are shown in Supplemental Table 1 and Supplemental Figs. 1–4. Male cases (case Nos. 1 and 2) were classified as score 1 and score 2, respectively, for light microscopic renal lesions, indicating the absence of glomerular lesions with or without interstitial inflammation. Two females (case Nos. 3 and 4) were classified as score 5 according to the light microscopic examination, including an increase in mesangial matrix in the hilar area or segmental mesangial proliferation in glomeruli with tubulointerstitial lesions (Fig. 1). Another female (case No. 5) was classified as score 7 due to prominent interstitial inflammatory cell infiltration. Hyaline casts, an indicator of protein leakage from glomeruli, were found in case Nos. 4 and 5. No changes of the glomerular capillary loops were detected using periodic acid-Schiff, periodic acid-methenamine-silver, or Masson’s trichrome stain in any of the cases.
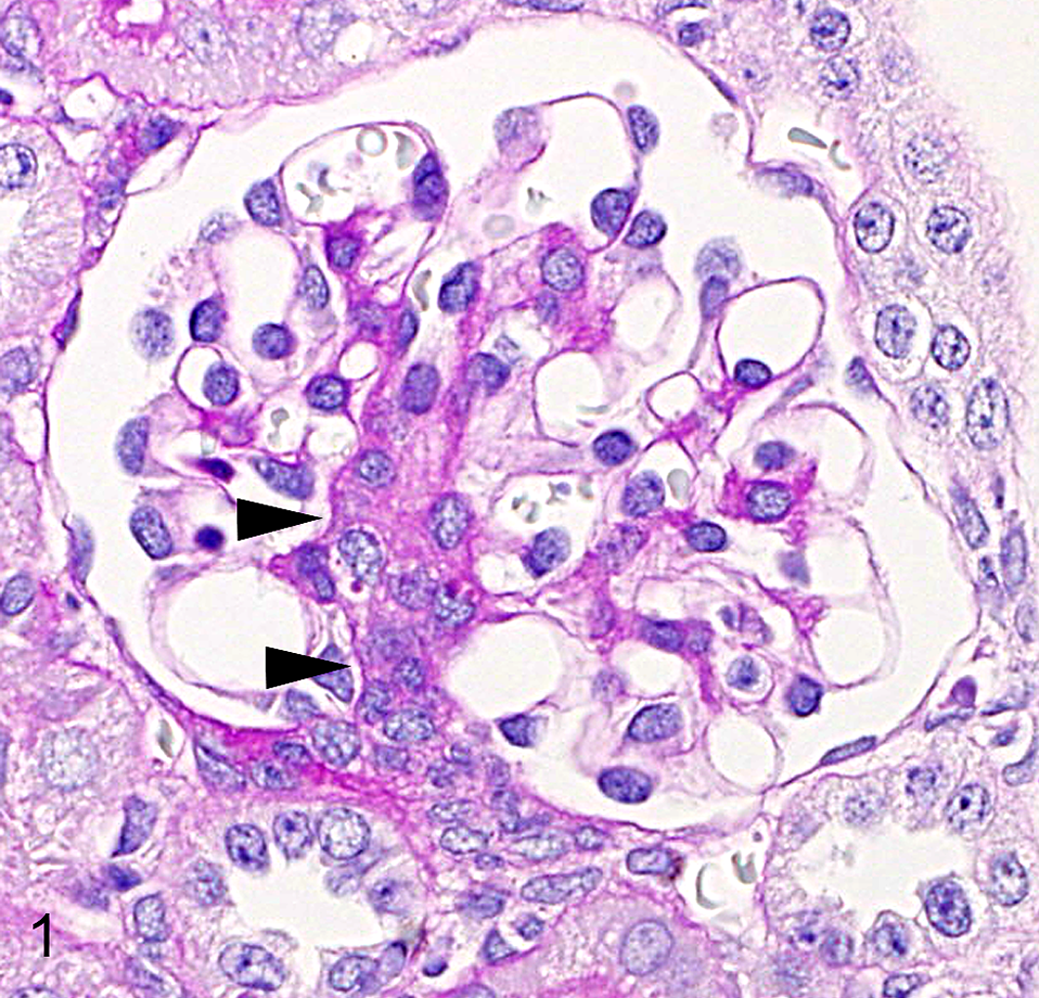
Progressive glomerulonephropathy, kidney, common marmoset, case No. 3 (renal lesion score 5). The mesangial cells and mesangial matrix at the glomerular hilum are slightly proliferated (arrowheads). Periodic acid-Schiff.
By electron microscopy, foot process effacement of epithelial cells (podocytes) accompanied by microvillus formation was observed in all animals, including a case of score 1 (without light microscopic lesions; Fig. 2). Thickening and reticulation (fraying and decreased density) of GBM were observed sporadically in the cases of score 2 and above (case Nos. 2–5; Fig. 2). In such cases, reticulation occurred on the endothelial side (lamina rara interna), and occasionally, small amounts of cytoplasm were present within the affected reticulated areas of GBM. Progression of thickening and reticulation was not detected in the cases of scores 2 (case No. 2) to 7 (case No. 5). Dense deposits within GBM were not observed in any case.
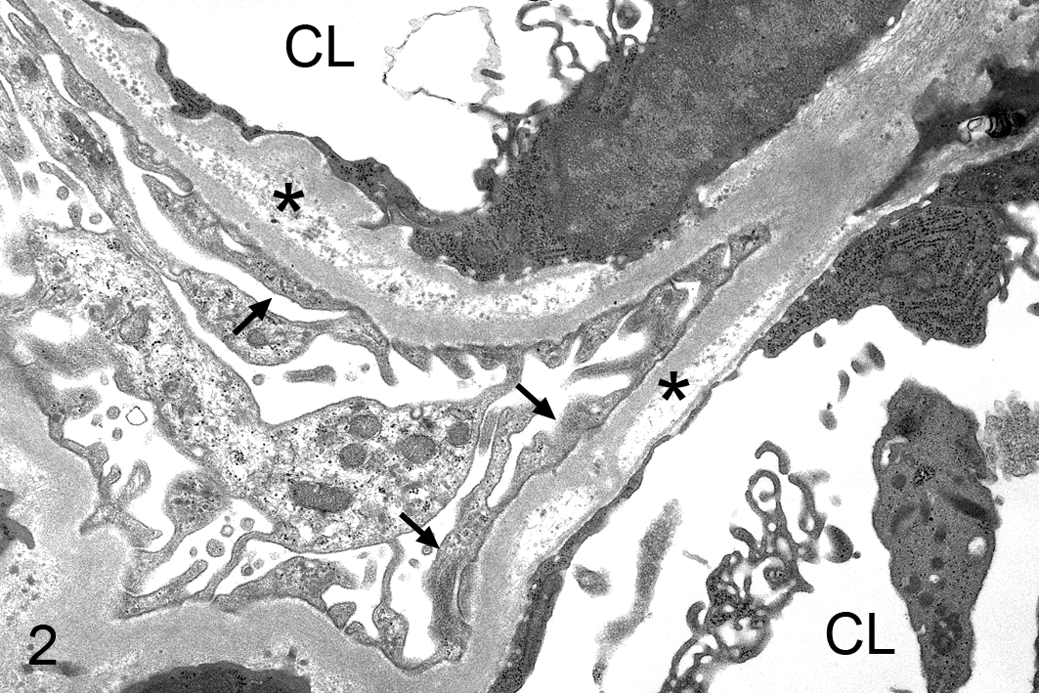
Progressive glomerulonephropathy, kidney, common marmoset, case No. 2 (renal lesion score 2 based on light microscopy). The foot processes of epithelial cells are effaced (arrows), accompanied by microvillus formation. Thickening and reticulation of glomerular basement membrane are observed (asterisk). CL, capillary lumen. Transmission electron microscopy.
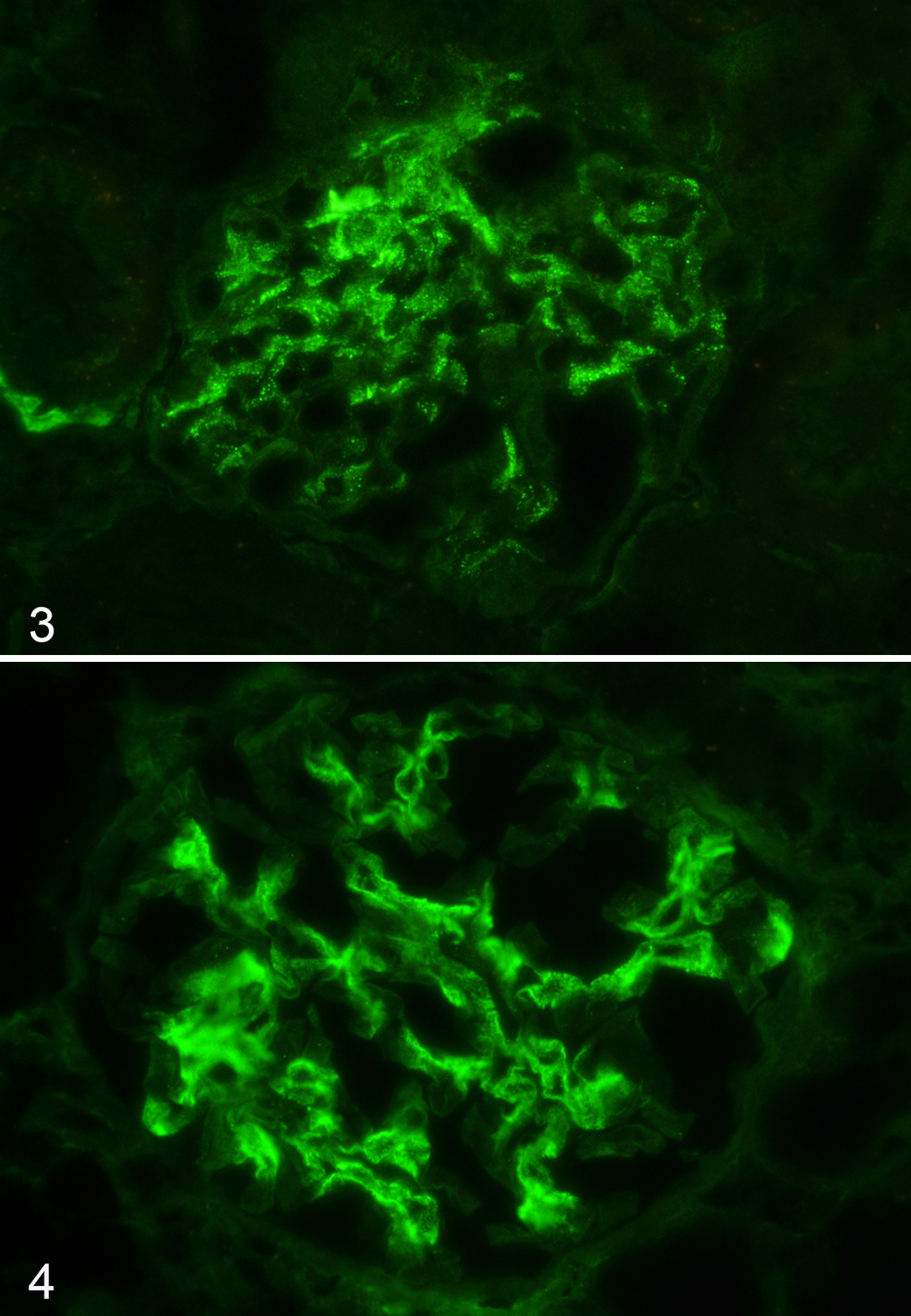
Immunohistochemical examination revealed positive reactions for IgM in the mesangial area, especially at the hilum in all animals (Supplemental Figs. 5–13). IgM deposition showed a fine granular pattern in case No. 2 (score 2) and coarse granular patterns in case No. 1 (score 1; Fig. 3), case No. 3 (score 5), and case No. 5 (score 7). IgA positive reactions were observed in the entire mesangial area in all animals except for case No. 1 (score 1). Positive reactions showed fine granular patterns in case No. 2 (score 2) and case No. 3 (score 5), and coarse granular or partial linear patterns in case No. 4 (score 5) and case No. 5 (score 7). IgG positive reactions were expressed in the mesangial area and the wall of the capillary loop in case No. 4 (score 5) and case No. 5 (score 7). Positive reaction showed a fine granular pattern in case No. 5 (score 7) and coarse granular pattern in case No. 4 (score 5; Fig. 4).
To estimate the relationship between the primary lesions and immunoglobulin deposition, we analyzed the glomeruli in the young marmosets by ultrastructural and immunohistochemical examinations. The summary of our findings is as follows: (1) Only immunoglobulin IgM was deposited in the mesangium in the stage showing only foot process effacement without GBM lesions by electron microscopy, (2) glomerular IgA and IgM deposits were also present in the stage showing reticulation and thickening of GBM by electron microscopy, and (3) IgG started to deposit in the glomeruli in the stage showing hyaline casts by light microscopy, which was an indicator of protein leakage from the glomeruli.
In callitrichid nephropathy, focal GBM reticulation and foot process effacement was previously reported; the glomerular lesion could already be detected in the mesangium area by light microscopy. 4 We showed that foot process effacement had occurred even though the glomerular lesions were not detected by light microscopy. Our results demonstrate earlier lesions than those previously reported. 4 Minimal change disease of the kidney is characterized by effacement of foot processes and IgM deposition at the glomerular mesangial area in young humans. 1 The causal relationship between foot process effacement and mesangial IgM deposition has not yet been studied in detail in either humans or marmosets. As the location of early IgM deposition was distant from the podocytes, cytokines mediate the podocyte injury similar to what occurs in IgA nephropathy with minimal change disease, where aberrantly glycosylated IgA1 is considered to be the cause of cytokine release from mesangial cells. 5 In addition, foods eliciting IgM responses may cause IgM deposition in both humans and marmosets. 5,9 In our marmosets, effacement of foot processes may be associated with IgM deposition similar to human minimal change disease of the kidney, and IgM may be the primary or earliest immunoglobulin type to be deposited in this nephropathy. 1
IgA and IgG deposition was also found in our study. IgA and IgG deposits increased with the increased progression of the renal lesions. Reticulation and thickening of GBM were observed by electron microscopy in renal lesions scored 2 and above. Hyaline casts were observed in 2 animals in which IgG was found in the glomeruli. Our findings suggest that IgA and IgG deposition plays an important role in the progression of the nephropathy. It is speculated that the later deposition of IgA and IgG compared with IgM represents isotype switching from IgM to IgA or IgG against antigens that elicit an immune response during the progression of the nephropathy, similar to that previously reported in immune responses to outer membrane antigens of Haemophilus parainfluenzae (a normal bacterial flora in the oral cavity) in human IgA nephropathy. 7 The serum levels of IgA associated with callitrichid nephropathy have been previously reported; however, it was not clear whether the progression of nephropathy involved IgA deposition in the glomeruli or not. 3
In conclusion, we have revealed that IgM deposition and foot process effacement of podocytes occur early in the life of marmosets affected with progressive or IgM nephropathy. The IgM deposition was considered primary, whereas IgA and IgG deposition occurred later with progression of the nephropathy in its preonset or early stage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.