
Abstract
A bilateral, locally invasive renal oncocytoma was diagnosed in a 10-year-old spayed female Greyhound dog. The diagnosis was based on positive staining of the tumor with the periodic acid-Schiff reaction prior to diastase treatment, on the immunohistochemical expression of cytoplasmic cytokeratin, and on the prominence of mitochondria in the tumor cells.
In the dog, tumors with granular cytoplasm staining brightly eosinophilic with hematoxylin and eosin (HE) include granular cell tumors, rhabdoid tumors, neuroendocrine tumors, and oncocytomas. Oncocytomas are rare, usually benign, tumors composed of oncocytes. Oncocytes are large polygonal cells characterized by brightly eosinophilic granular cytoplasm. Oncocytomas have been sporadically described in humans, dogs, cats, and rats. 1 , 2 , 5 , 8 , 10 , 15 In humans, such tumors have been identified in salivary glands, a variety of endocrine glands, liver, lung, and kidney. In the dog, oncocytomas have been reported originally in the larynx and recently in the thyroid gland. 7 , 9 , 15 There is one report of a chromophilic-eosinophilic (oncocyte-like) renal cell carcinoma in a dog. 18 The authors described two different oncocyte-like populations of tumor cells and concluded from their morphologic and immunohistochemical studies that the tumor in that dog resembled a renal oncocytoma more than a renal carcinoma. 18 Renal oncocytomas that occur in humans must be differentiated from granular cell carcinoma, carcinoid, and renal clear cell carcinoma. 11 Approximately 300 cases of human renal oncocytomas have been reported, of which the majority were benign and unilateral. 6 Approximately 6% of patients had bilateral oncocytomas. 6 This report deals with the microscopic, immunohistochemical, and ultrastructural features of a renal oncocytoma in a dog.
A 10-year-old spayed female Greyhound dog was presented with a history of anorexia and weight loss. A 8- × 5- × 2-cm growth associated with the right lumbar muscles was assessed as an abscess radiographically. Both kidneys had several circular growths; the largest was 2 cm in diameter. Tissue samples from lesions in the kidney and lumbar muscles were obtained through percutaneous keyhole biopsy, fixed in 10% buffered formalin, and evaluated by light microscopy. The clinical diagnosis was renal and muscle abscesses or neoplasia. Because the condition of the dog deteriorated due to renal failure, euthanasia was elected. A necropsy was not permitted.
Formalin-fixed, paraffin-embedded sections of kidney and muscle were stained with HE, periodic acid–Schiff (PAS), Fontana-Masson silver, Masson's trichrome, phosphotungstic acid–hematoxylin (PTAH), Luxol fast blue/PAS, Manuel's reticulin, Grocott's methenamine silver (GMS), and Alcian blue for light microscopic examination. The immunohistochemical profile of the tissue from the kidney included cytokeratin, desmin, vimentin, glial fibrillar acidic protein (GFAP), S-100 protein, lysozyme, alpha1-antichymotrypsin, and canine immunoglobulin subclasses G, A, and M. An avidin–biotin complex (ABC) method was used according to the manufacturer's specifications (Vector Laboratories, Burlingame, CA) with various primary polyclonal antibodies. Sections stained for vimentin were pretreated with 0.25% trypsin. Controls used normal serum in place of the specific primary antibody. Paraffin-embedded renal tissues were deparaffinized, postfixed in 1% osmium tetroxide, and processed routinely prior to examination in a Philips transmission electron microscope.
Microscopic evaluation revealed a neoplastic mass that effaced the architecture of the renal cortex and inner medulla and extended into the renal capsule. The neoplasm was composed of compact monomorphic sheets and clusters of closely packed 20–30 µm round to oval cells separated intermittently by fine collagenous stroma (Fig. 1). The cytoplasm of the neoplastic cells was eosinophilic and finely granular to feathery. Cell borders were indistinct. Nuclei were round to oval, central to paracentral to eccentric, and well defined and had euchromatic, coarsely stippled, regularly arranged chromatin. Nucleoli were prominent, deeply eosinophilic, single, and central to paracentral. Nucleus:cytoplasm ratio was 1:3. There was moderate anisokaryosis and anisocytosis, and occasional binucleate or multinucleate neoplastic cells were present. No vascular or lymphatic invasion was noted. At the periphery of the neoplasm, there were aggregates of lymphocytes and well-differentiated plasma cells. Similar neoplastic cells had infiltrated the lumbar muscles. The cells, however, were smaller, and there was considerable intraneoplastic necrosis and hemorrhage. The tumor-infiltrated muscle fibers also had multifocal degeneration, necrosis, atrophy, and fibrosis and in several areas were regenerative, as evidenced by proliferating satellite cells.
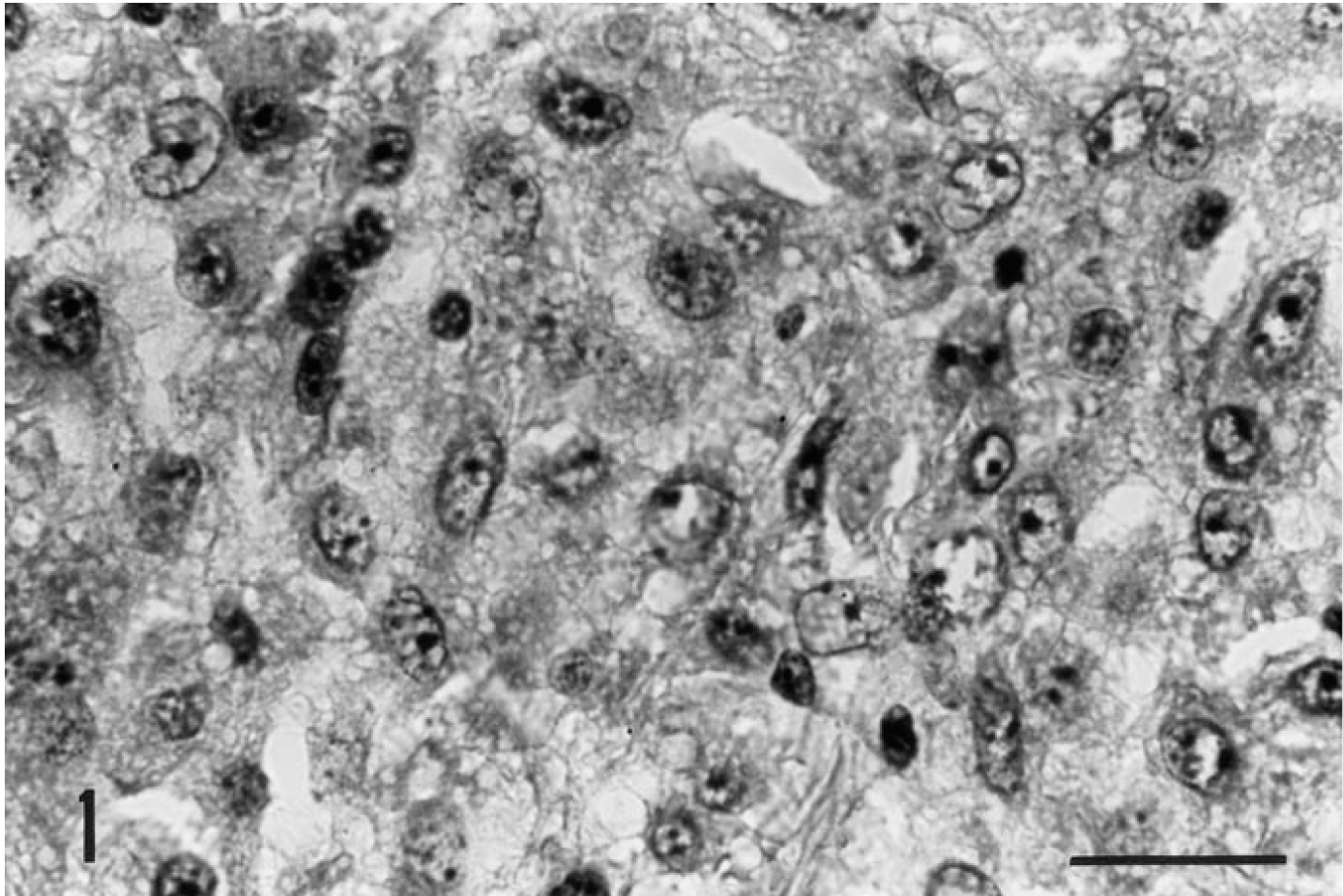
Kidney, oncocytoma; dog. A monotonous population of neoplastic round cells is characterized by granular cytoplasm and indistinct cell borders. Mitotic figures are absent. HE. Bar = 20 µm.
The cytoplasmic granules were moderately positive by PAS staining and stippled. After diastase treatment, the granules were rarely positive on PAS. After Luxol fast blue/PAS staining, the cytoplasm of the tumor cells was weakly PAS positive and Luxol fast blue negative. Masson's trichrome stained the cytoplasm diffusely red; it was weakly stippled with PTAH staining. The cytoplasm was negative for nonargentaffinic (Fontana - Masson) and nonargyrophilic (GMS) granules. A reticulin stain demonstrated delicate fibrils around individual tumor cells. The tumor cytoplasm did not stain with the reticulin and Alcian blue techniques.
The ABC immunohistochemical stains for cytokeratin revealed moderate to strong positive dots, granules, and clumps in individual tumor cells (Fig. 2). The cytoplasm of the plasma cells was negative for cytokeratin. Stains for desmin, vimentin, GFAP, S-100, lysozyme, and alpha1-antichymotrypsin were negative.
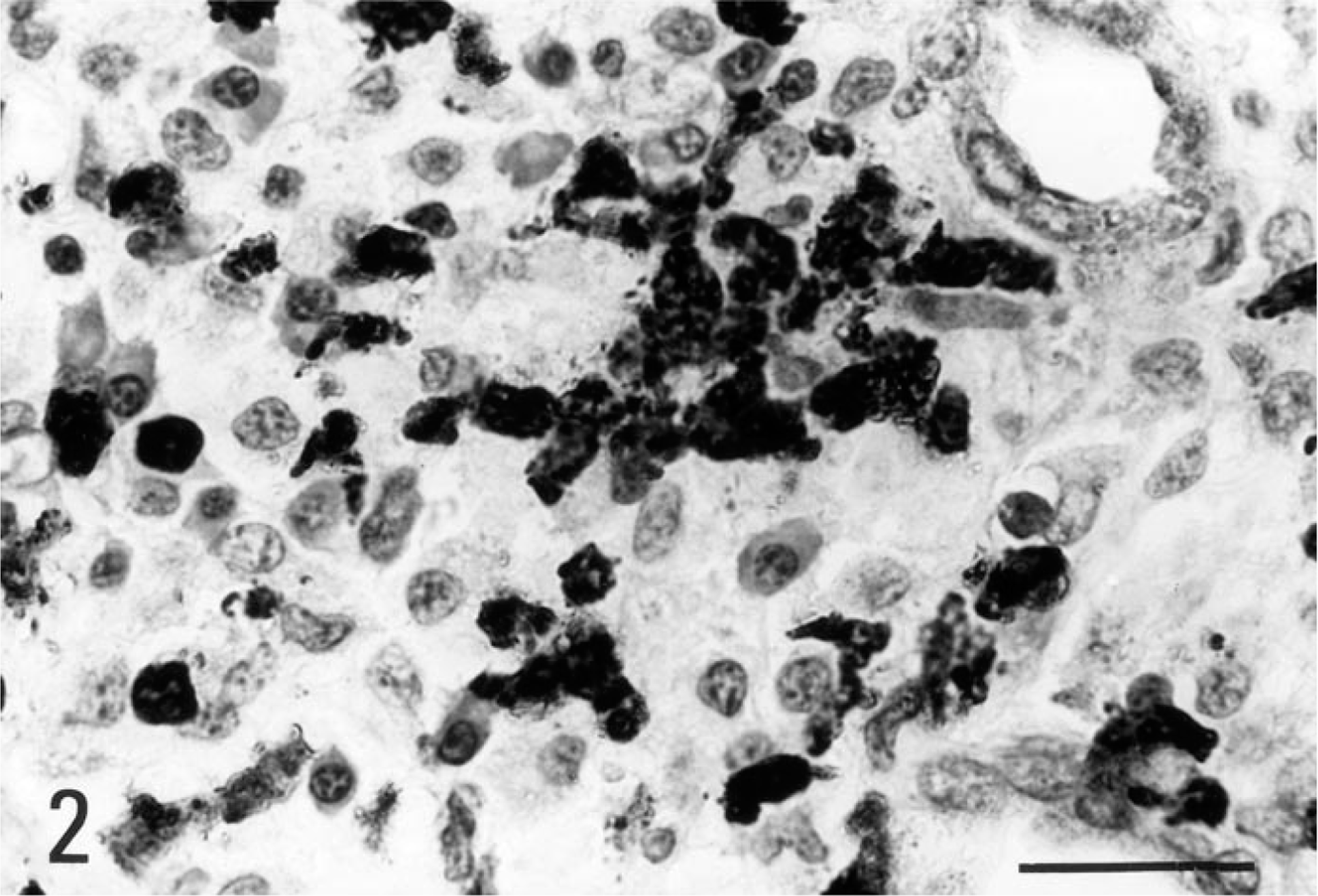
Kidney, oncocytoma; dog. Several tumor cells demonstrate granular cytoplasmic and nuclear staining for cytokeratin. ABC method, Mayer's hematoxylin counterstain. Bar = 20 µm.
Ultrastructurally, the neoplastic cells were a monotonous population of closely opposed, round to oval to polygonal cells with prominent, complex interdigitations and invaginations of the basal plasmalemma. The cytosol was moderately filled with mature mitochondria, some rough endoplasmic reticulum, and a few free polyribosomes (Fig. 3). Cytoplasmic vesicles were absent. Mitochondria had various numbers of irregular lamellar cristae. Adjacent neoplastic cells lacked junctional complexes. Nuclei were large, round to oval, and occasionally indented. Heterochromatin was marginated (Fig. 3).
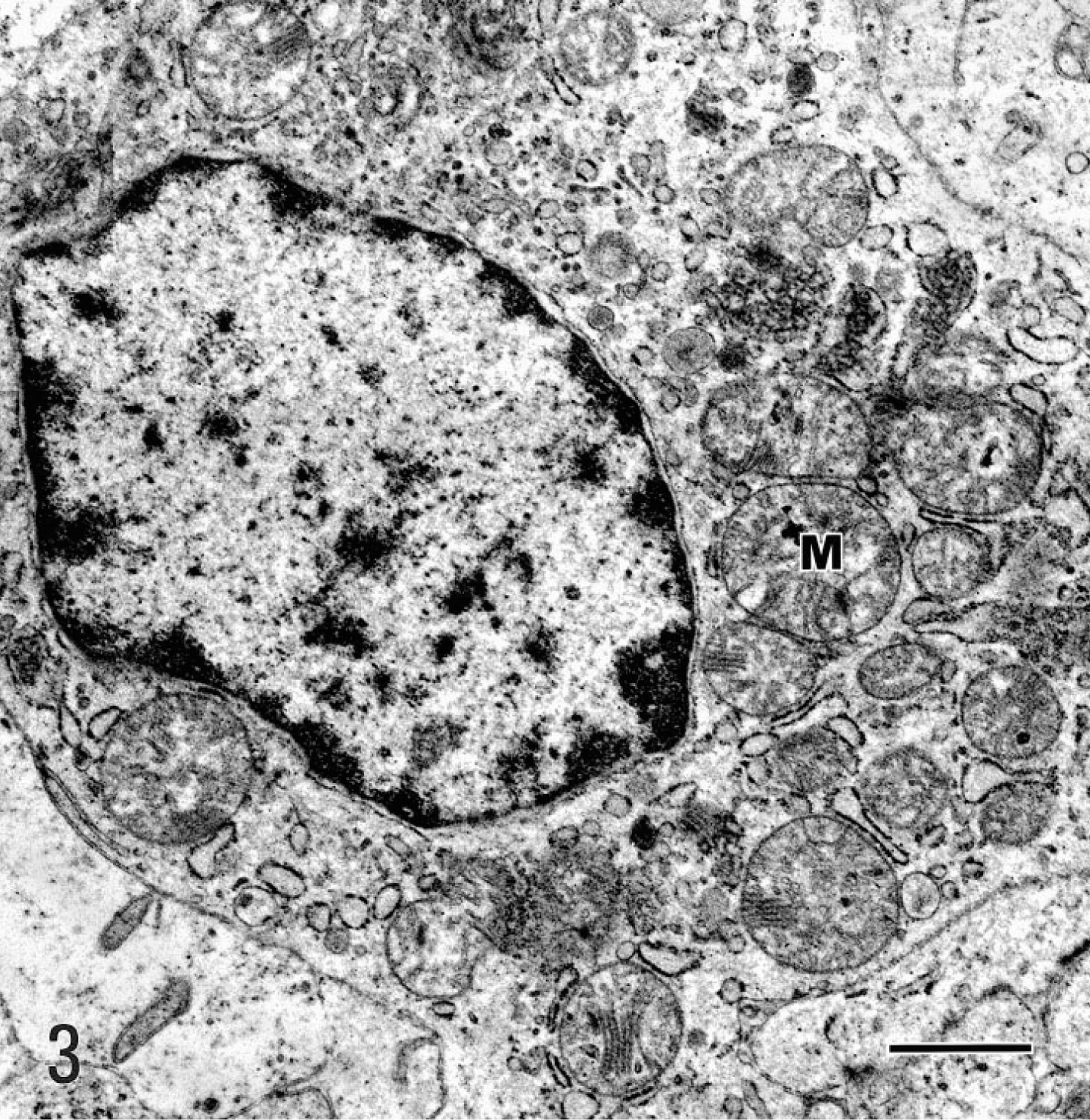
Transmission electron micrograph. Renal oncocytoma; dog. Moderate numbers of mitochondria (M) fill the cytosol. A few free polyribosomes are also present. Some rough endoplasmic reticulum is interspersed. The nucleus is slightly irregular and has marginated heterochromatin. Bar = 1 µm.
Based on the tinctorial results, immunohistochemical profile, and ultrastructural features, the tumor in the dog's kidney was identified as an oncocytoma with its major cytosol component being mitochondria. The tumor cells in the skeletal muscles were presumed to be of similar lineage and the result of local invasion from the kidney.
Oncocytomas must be distinguished histologically from granular cell tumors and rhabdomyomas and in the kidney from renal cell carcinomas. 4 , 7 , 11 Microscopically, oncocytomas are composed of neoplastic cells with brightly eosinophilic cytoplasm. The neoplastic oncocytes are most commonly organized as solid compact nests, as in this case, or cords or tubules. 13 Oncocytic tumor cells infiltrate between renal tubules, as in this case. 13 The histogenesis of renal oncocytomas is unclear. They probably arise from intercalated cells of the collecting ducts. 3 They are differentiated from renal carcinomas at the light microscopic level by the absence of papillary structures and the absence of mitoses. The main differential diagnostic difficulty is with chromophobe cell carcinoma, to which these lesions may be related. 13 , 14 Chromophobe cell carcinomas have pale acidophilic cytoplasm and a clear perinuclear region. 14 , 16 They stain positive for mucin. 14 Ultrastructurally, their cytosol contains mitochondria and numerous small cytoplasmic vesicles. 14 Chromophobe cell carcinomas are presumed to also originate from intercalated cells of collecting ducts. 14 Regardless of the organ of origin, ultrastructural studies are needed to define the tumor lineage. Oncocytomas characteristically have abundant mitochondria with stacked cristae filling the cytoplasm of the cells, 14 whereas granular cell tumors are mainly composed of lysosome-laden cells that also contain particulate glycogen, polyribosomes, and mitochondria as up to 50% of the total number of organelles. 3 Rhabdoid tumors ultrastructurally contain mitochondria and aggregates of myofilaments. 7–9
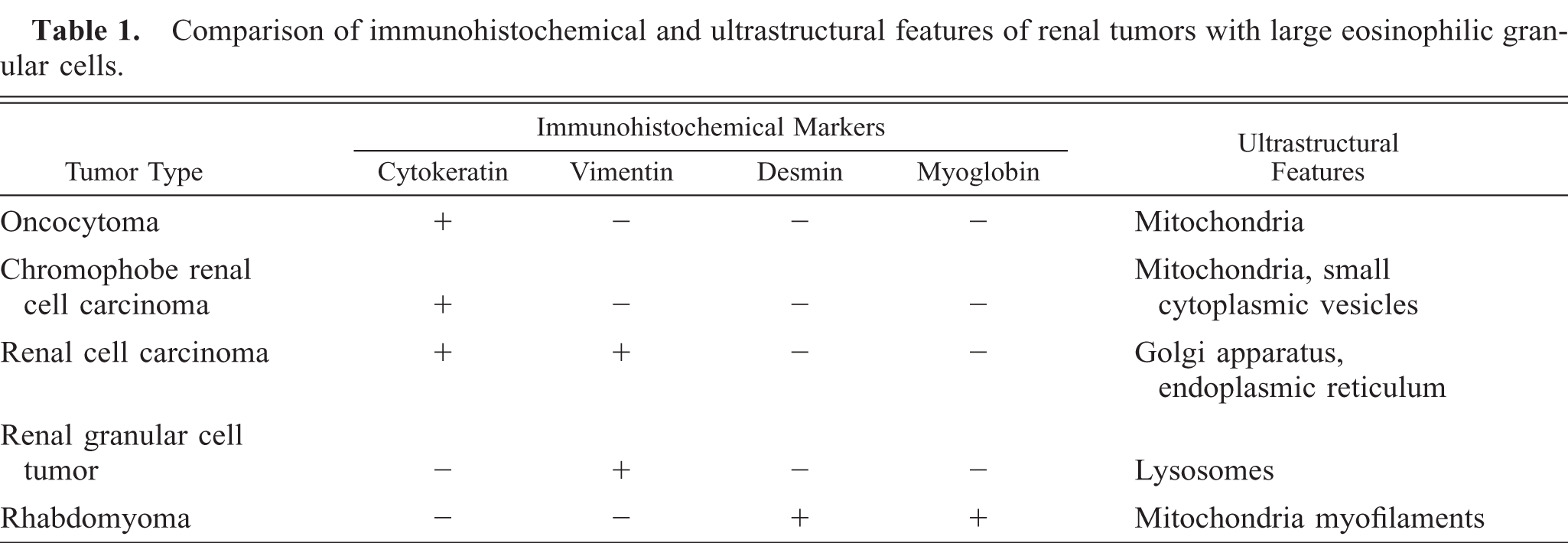
Specific immunohistochemical markers are helpful in making a differential diagnosis. Oncocytomas specifically express cytokeratin, 15 , 17 whereas renal cell carcinomas coexpress vimentin and cytokeratin. 12 Nonrenal granular cell tumors are positive for vimentin and are negative for epithelial cell markers. 10 Rhabdoid tumors react positively for desmin and intracellular myoglobin. 9 The expression of intermediate filament proteins in subtypes of renal cell carcinomas and in renal oncocytomas makes it possible to distinguish between two classes of renal cell tumors. The consistent absence of vimentin in chromophobe cell carcinomas and oncocytomas enables one to define these tumors as a separate class of renal cell tumors. These distinguishing features may be of importance for surgical pathologists because granular cell tumors have many similarities at the light microscopic level. Table 1 summarizes a comparison of markers for the various tumors with granular cytoplasm.
Comparison of immunohistochemical and ultrastructural features of renal tumors with large eosinophilic granular cells.
The diagnosis of oncocytoma in this dog primarily was based on immunohistochemical and electron microscopic features. The absence of cytoplasmic vesicles ruled out chromophobe renal cell tumor. The tumor had a locally aggressive behavior as evidenced by infiltration of adjacent lumbar muscles. Some undifferentiated features at the ultrastructural level, e.g., inconsistent distribution of mitochondria in cytosol and poorly developed mitochondria, suggested some degree of dysmaturity. Distant metastases were not observed clinically.
Little is known about clinical aspects of renal oncocytomas in humans. 6 These lesions may present with flank pain and hematuria. 11 When involving the kidney, they are usually solid and well-encapsulated tumors and rarely penetrate the renal capsule or invade adjacent structures. 6 They average 7 cm in diameter when detected and typically are unilateral. 6 , 12 The specific diagnosis is usually made by the surgical pathologist after thorough examination of the entire neoplasm. 6
Footnotes
Acknowledgements
We thank Dr. Ronald Mason (Borita Springs, FL) for referring the specimens to our Surgical Pathology service; Ms. Betty Hall for superb immunohistochemical work, and Karin L. Vaughn (ICBR) for electron microscopic assistance.