
Abstract
The vasa vasorum is a delicate network of small arterioles that supplies nutrients to the adventitia and outer media of large arteries. In humans, dysfunction of the vasa vasorum contributes to the pathogenesis of aortic dissection and atherosclerosis. Twenty-four cats from 1 to 18 years of age were prospectively evaluated. Cases were divided into 3 cohorts—with systemic hypertension, without systemic hypertension, and uncertain. Histologic sections of the aorta and main pulmonary artery, as well as sections of kidney and lung, were blindly examined by 2 pathologists. The severity of vasa vasorum arteriopathy was compared to the presence of renal arteriosclerosis, aortic medial degeneration, subintimal fibroplasia of the main pulmonary artery, and blood pressure. We found that vasa vasorum arteriopathy correlated strongly with hypertensive status, degree of renal arteriosclerosis, and lesions in the great vessels. The positive predictive value of a severe vasa vasorum score for systemic hypertension was 84.6%. Lesions of vasa vasorum arteriopathy were predictive of renal arteriosclerosis with 100% sensitivity and 64.7% specificity. The positive predictive value of a severe vasa vasorum score for the presence of aortic lesions was 69.2% vs 91.6% for lesions in the main pulmonary artery. The vasa vasorum appears to be an important responder to systemic hypertension in cats, and arteriopathy of this vascular bed has significant implications for the integrity of the great vessels.
Keywords
The vasa vasorum (VV) is a small capillary branching network that supplies the adventitia and outer medial wall of large vessels such as the aorta and main pulmonary artery. The VV fills during diastole; with increased pressure in the aorta and increased rigidity in the arterial wall associated with systemic arterial hypertension (HT), the VV is compressed and blood flow decreases. 23,29 Decreased blood flow through this network results in local hypoxia and aortic medial necrosis, and it may result in aortic dissection. 29 Experimental ligation of the VV results in medial aortic necrosis in dogs. 23 In human patients undergoing aortic dissection repair, 18 of 20 patients showed sclerotic lesions of the VV, including muscular hyperplasia and intimal fibrosis. 26 The cumulative result of decreased flow in the VV is increased vascular tone and local oxidative stress causing local hypoxia, leading to neovascularization with reduced vasodilatory capacity. These changes also predispose the aorta to the development of atherosclerotic plaques in humans. 29 Lesions in the VV secondary to spontaneous disease have not been described in domestic species.
Systemic arterial hypertension is a common complicating condition of chronic diseases in cats and may also occur as a primary disease of unknown cause. Common causes of HT in cats include kidney disease, hyperthyroidism, primary hyperaldosteronism, chronic anemia, and diabetes mellitus. 34 The histolopathologic determination of HT in cats with chronic kidney disease (CKD) remains a topic of debate, with recent work demonstrating that the incidence of arteriosclerosis is not significantly different between hypertensive and normotensive cats with CKD. 24 A different study found conflicting results suggesting arteriosclerosis was uncommon in normotensive cats with CKD. 8 Morphologically, arteriosclerotic lesions in the retinal, meningeal, and renal vasculature have been well described in cats with clinically documented HT. 3,9,34
Responses of small arteries and arterioles to HT include intimal remodeling with narrowed lumen diameter and hypertrophic remodeling of the media. 19,35 Arteriosclerosis is a morphologic description of these changes, which include medial smooth muscle degeneration with vacuolation and/or increased amounts of cytoplasm, hypertrophy, and hyperplasia. Pathologic criteria for the diagnosis of HT in veterinary species are not well described. Instead, there are lesional findings in small arteries and arterioles as well as pathologic conditions that are considered “consistent” with hypertension. 3,36 Animals with documented elevations in blood pressure present with a spectrum of lesions that may include arteriosclerosis and/or hyaline vasculitis in end organs such as brain, eye, kidney, and heart. Arteriosclerosis is typically interpreted as secondary to HT in humans; however, the pathogenesis of this lesion in domestic species is poorly understood. 10,27,28 Neovascularization, as noted in the VV of humans with HT, is not a commonly described feature in other vascular niches. This is likely due to the microenvironment in the adventitial adipose tissue of large vessels and may be a unique finding to VV in the context of HT.
Based on these descriptive findings of vascular lesions in both humans and in experimental settings of veterinary species with HT, we designed a prospective study of VV lesions in cats. The aims of the study were to evaluate the presence of VV arteriopathy in cats and to correlate lesions of the VV to the presence of HT. Our hypotheses were (1) that cats develop VV arteriopathy, (2) that these lesions occur in the context of HT, and (3) that these lesions may have a consequential impact on the integrity of the great vessels they supply.
Materials and Methods
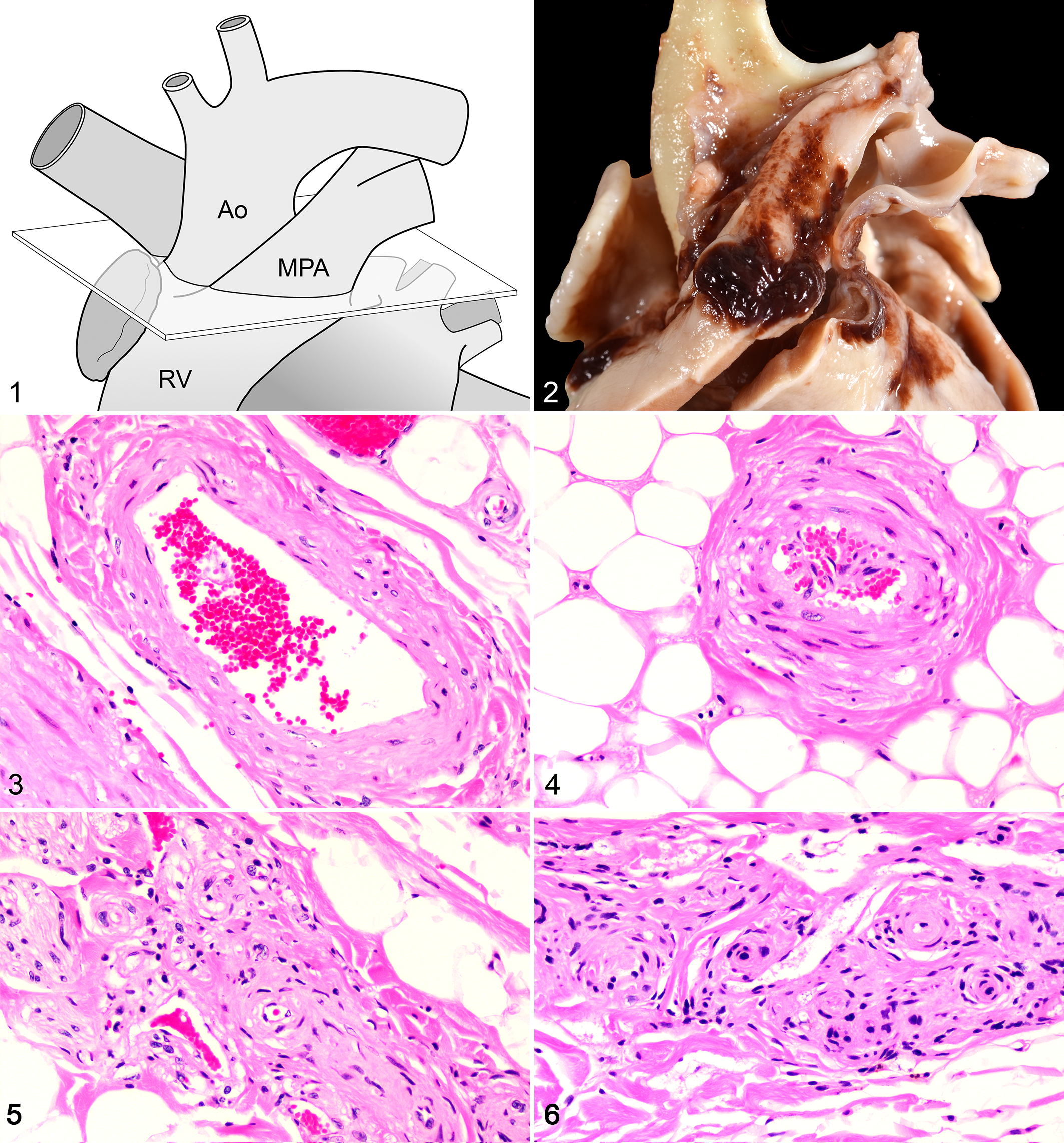
Animals in our cohort were identified postmortem from the Applied Pathology service at The Ohio State University College of Veterinary Medicine. Case inclusion criteria were (1) cats, (2) age greater than 1 year, (3) and lack of inflammatory cardiovascular diseases such as feline infectious peritonitis. Selected animals were given arbitrary designations to blind the evaluators to the clinical history and diagnoses. The tissues evaluated included a coronal cross section 0.2 cm distal to the annulus of the main pulmonary artery, which included aorta, main pulmonary artery, and intervening tissue (Fig. 1). Additional tissues included a section of kidney to include the corticomedullary junction and a section of lung to include the secondary bronchus or larger. Tissues were fixed in 10% neutral buffered formalin, embedded in paraffin, and cut into 3- to 5-μm sections. Each set of tissues was stained with hematoxylin and eosin and Verhoeff–van Gieson.
A grading scheme to assess the severity of VV lesions, as well as lesions in the aorta, main pulmonary artery, and renal vasculature, was designed a priori (Suppl. Table S1).
To facilitate consistent evaluation, sections of great vessels that included fewer than 10 cross sections of the VV were excluded from the study cohort. A veterinary pathology resident (R.K.) and a board-certified veterinary pathologist (C.P.), blinded to the identification of each cat as well as to clinical and pathological diagnoses, independently evaluated all tissues. Any additional (nonvascular) findings in evaluated sections were noted. A consensus score was arrived at upon conference between the 2 pathologists, while still blinded to the diagnosis. Following histologic evaluation, the cases were unblinded so that VV severity scores could be correlated to clinical findings.
Three cohorts of cats were evaluated—with HT, without HT, and uncertain HT status. Cats with measured HT (defined as systolic arterial blood pressure >150 mm Hg), as well as those cats with clinical and pathologic findings consistent with HT (such as multisystemic arteriopathy or hyaline vasculitis), were included in the HT cohort. Multisystemic arteriopathy, arteriosclerosis, and fibrointimal hyperplasia affecting small-caliber arteries and arterioles in multiple end organs are findings consistent with HT and were thus the basis for diagnosis of HT in this study in cases where blood pressure was not available. Morphologic components of arteriosclerosis were included in the grading scheme (Suppl. Table S1). Importantly, this consideration excluded any renal vascular lesions suggestive of HT, as we sought to evaluate a potential relationship between VV lesions and renal vascular disease separately. The non-HT cohort included cats with a documented normal blood pressure measurement as well as those cases with diagnoses unrelated to vascular or renal disease, such as fracture and nasal lymphoma, and having no vascular lesions on histopathologic examination. A final cohort of uncertain HT status included cats with mild histologic evidence of chronic renal disease but with no evidence of multisystemic arteriopathy.
The diagnosis of renal and VV vascular disease included evaluation of intimal proliferation, medial hypertrophy and/or degeneration, and adventitial fibrosis. Additional findings, including neovascularization, inflammation, and hyalinosis, were noted. Moderate to severe pulmonary arterial medial hypertrophy was interpreted as suggestive of pulmonary arterial hypertension (PAH). Renal scores and VV scores were stratified into high, medium, and low. A VV score of 15 or greater was considered severe/high, 7 to 14 moderate/medium, and 0 to 6 mild/low. A renal score of 9 or greater was considered severe/high, 4 to 8 moderate/medium, and 0 to 3 mild/low. Further analysis was performed to determine the predictive value of VV lesions for renal arteriosclerosis as well as degenerative changes in the great vessels.
Statistical evaluation was performed using commercially available software. Analyses included Pearson’s correlation analysis, 1-way analysis of variance (ANOVA), and Student t test where appropriate. Positive and negative predictive values, sensitivity, and specificity were calculated. Receiver operating characteristic curve (ROC curve) analysis was performed using the methods described 15 with binomial exact determination for the 95% confidence interval using MedCalc Statistical Software (MedCalc Software, Ostend, Belgium). Youden’s J index was calculated for an optimal balance sensitivity and specificity. Significance was defined as P < .05.
Results
Our prospective study included 24 cats ranging in age from 1 to 18.3 years of age. Only 6 of 24 (25%) of the cats in our study had arterial blood pressure measurements obtained and recorded. Eleven of the 24 cats (46%) were diagnosed with HT based on clinical and/or pathologic evaluation (Suppl. Table S2). Of these cats, 4 (36%) had recent systolic blood pressure evaluations available with measured blood pressures of 260, 178, 160, and 160 mm Hg. Concurrent diseases in the HT cohort included main pulmonary arterial (MPA) aneurysm (cat No. 1; Fig. 2), cerebral aneurysm, renal vascular hyalinosis, multisystemic arteriopathy, hyperthyroidism, and acromegaly. Of the 8 cats classified as non-HT, 2 had recent systolic blood pressure measurements of 92 and 110 mm Hg. Five cats were designated as uncertain HT status.
There were 5 animals (21%) with moderate to severe pulmonary arterial medial hypertrophy suggestive of pulmonary hypertension (PAH), with 3 in the HT cohort, 1 in the non-HT cohort, and 2 in the uncertain HT cohort. Eight animals (33%) were diagnosed with hypertrophic cardiomyopathy (HCM) based on clinical evaluation, heart weight, increased left ventricular mass, and/or histopathologic cardiac lesions. 20 Eight animals were diagnosed with CKD based on presence of moderate to severe interstitial lymphoplasmacytic interstitial nephritis with variable interstitial fibrosis and glomerulosclerosis (Suppl. Table S2).
Neovascularization Is a Prominent Feature of VV Arteriopathy
Cat No. 1 was a 14-year-old female spayed mixed longhair cat that at necropsy had extensive hemorrhage surrounding the base of the heart with a focal thin-walled dilation at the base of the main pulmonary artery (Fig. 2). Histologically, there was widespread neovascularization of the VV with mononuclear inflammation and vascular hyalinosis. Lesions typical of HT, including arteriosclerosis of the meningeal and retinal vessels, as well as renal interlobular arterioles, were also noted in this cat. Arteriosclerosis as described above was a predominant lesion in all of the study cohort that displayed VV lesions (13/24, 54%) (Figs. 3, 4). Neovascularization or vascular proliferation was noted, as well as occasionally significant amounts of adventitial proliferation and fibrosis, in all cats with severe VV lesions (Figs. 5, 6). Medial hyalinosis and thrombosis were uncommon in our study population.
Cat No. 9 was an 18-year-old female spayed American Shorthair cat that at necropsy had moderate renal cortical atrophy. Histologically in the kidney, there was chronic interstitial fibrosis and tubular atrophy, as well as lymphohistiocytic interstitial nephritis with mineralization. VV lesions were considered mild to moderate, featuring multifocal medial hypertrophy and degeneration, neovascularization, and adventitial proliferation. Cat No. 13 was a 5.5-year-old male castrated mixed longhair cat that at necropsy had a severely enlarged heart (weighing 33 g). Histologically in the heart were interstitial fibrosis and myofiber disarray consistent with hypertrophic cardiomyopathy. VV lesions were considered mild, featuring multifocal medial hypertrophy and degeneration.
VV Arteriopathy Occurs in HT Cats and Lesions in the VV Are Predictive of HT
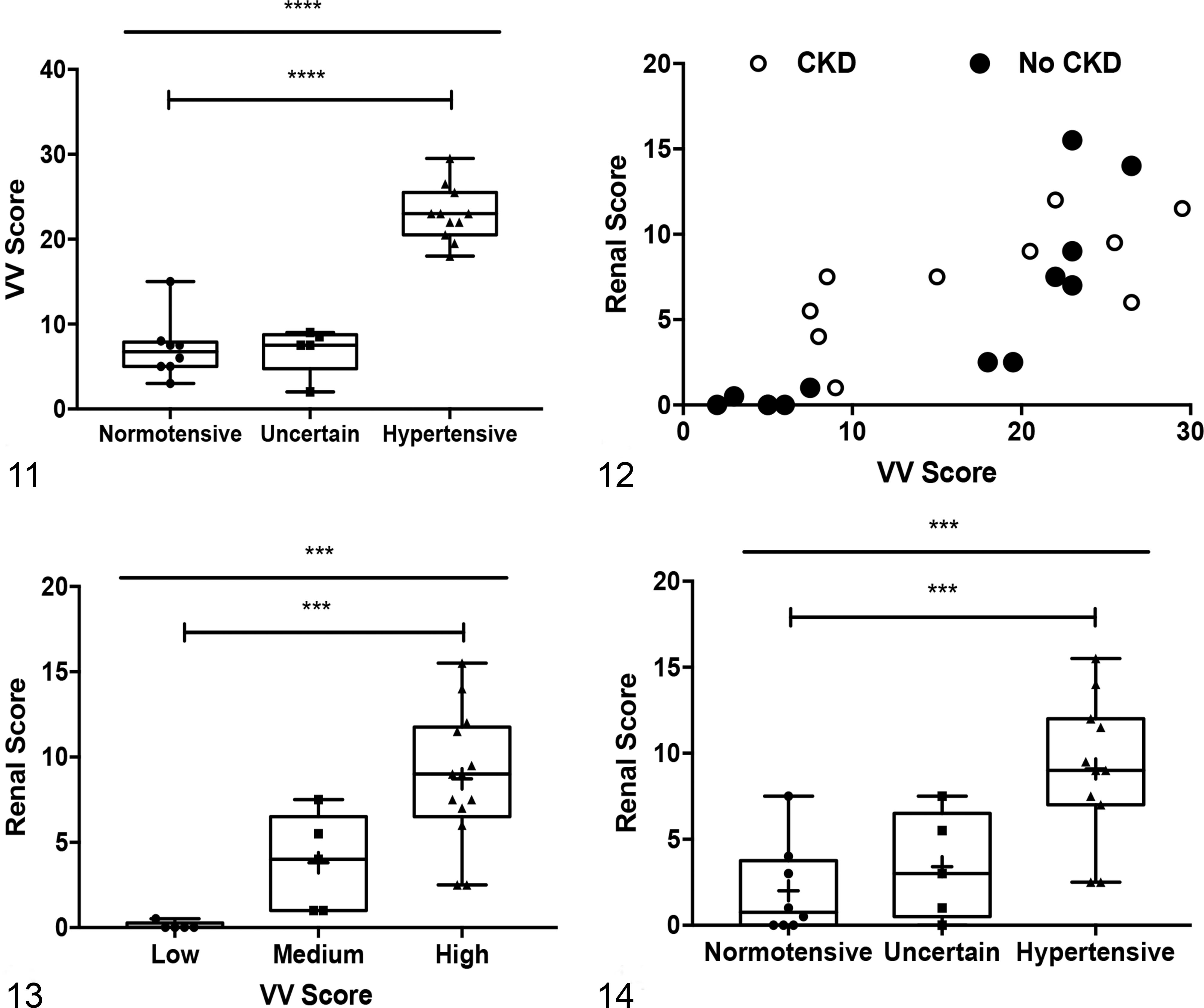
The VV scores were 22.9 ± 3.3 (mean ± SD, n = 11) for cats in the HT group, 7.1 ± 3.6 (n = 8) for non-HT animals, and 6.9 ± 2.8 (n = 5) for animals with uncertain HT status (Fig. 11). There was a significant association between VV score and HT status (P < .0001, ANOVA) and a significant difference between HT and non-HT animals (P < .0001, Student t test) (Fig. 11). The positive predictive value of severe VV score (≥15) for HT was 85%, and the sensitivity of the VV score for detection of hypertension was 92% (Table 1). In addition, the area under the ROC curve (AUC) was 93.4% (95% CI, 75.3%–99.5%; z = 6.48, P < .0001) (Table 1, Suppl. Fig. S1). Youden J index equaled 0.92 using the criterion index of >15 with a sensitivity of 100% and specificity of 92.3%. Note that this cutoff was the same as was used to delineate severe VV lesions.
Relationships Between Severe Lesions in the Vasa Vasorum and Other Vascular Changes in Cats.
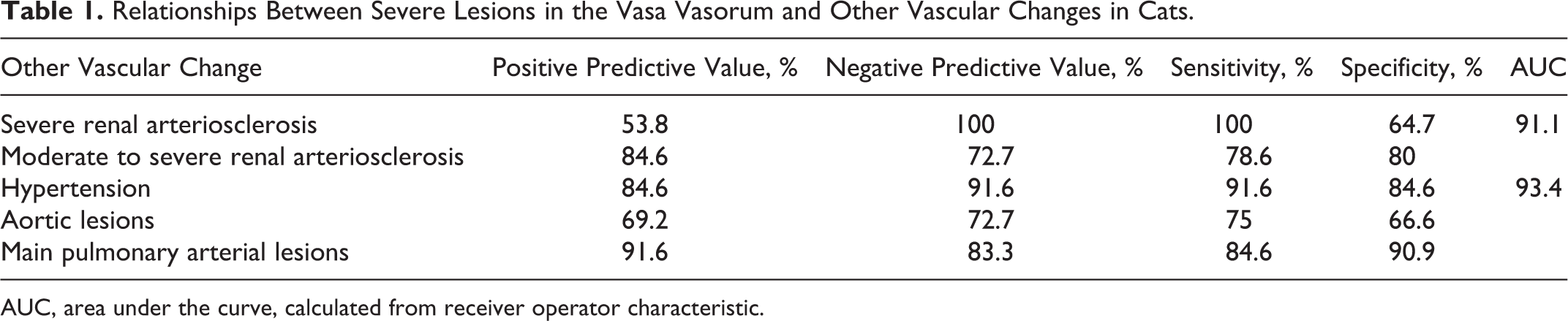
AUC, area under the curve, calculated from receiver operator characteristic.
Occurrence of VV Arteriopathy Does Not Correlate With Concurrent Diagnoses Such as HCM, PAH, or CKD
In the study population, 8 of 24 (33%) cats were diagnosed with HCM based on clinical and pathologic findings. An additional 2 cats had a clinical diagnosis of severe left ventricular hypertrophy secondary to hyperthyroidism and acromegaly. The VV score for these animals with severely increased left ventricular mass not attributable to HT alone was 16 ± 9.3 (mean ± SD, n = 10), while the score for the remaining cats was 14.5 ± 8.6 (n = 14). There were no significant differences between these data. Similar findings were noted for CKD (16.3 ± 8.7, n = 11 with CKD vs 14.3 ± 9.5, n = 13 without CKD) and PAH (17 ± 10.2, n = 6 with PAH vs 14.5 ± 8.4, n = 18 without PAH).
VV Arteriopathy Correlates With Degree of Renal Arteriosclerosis
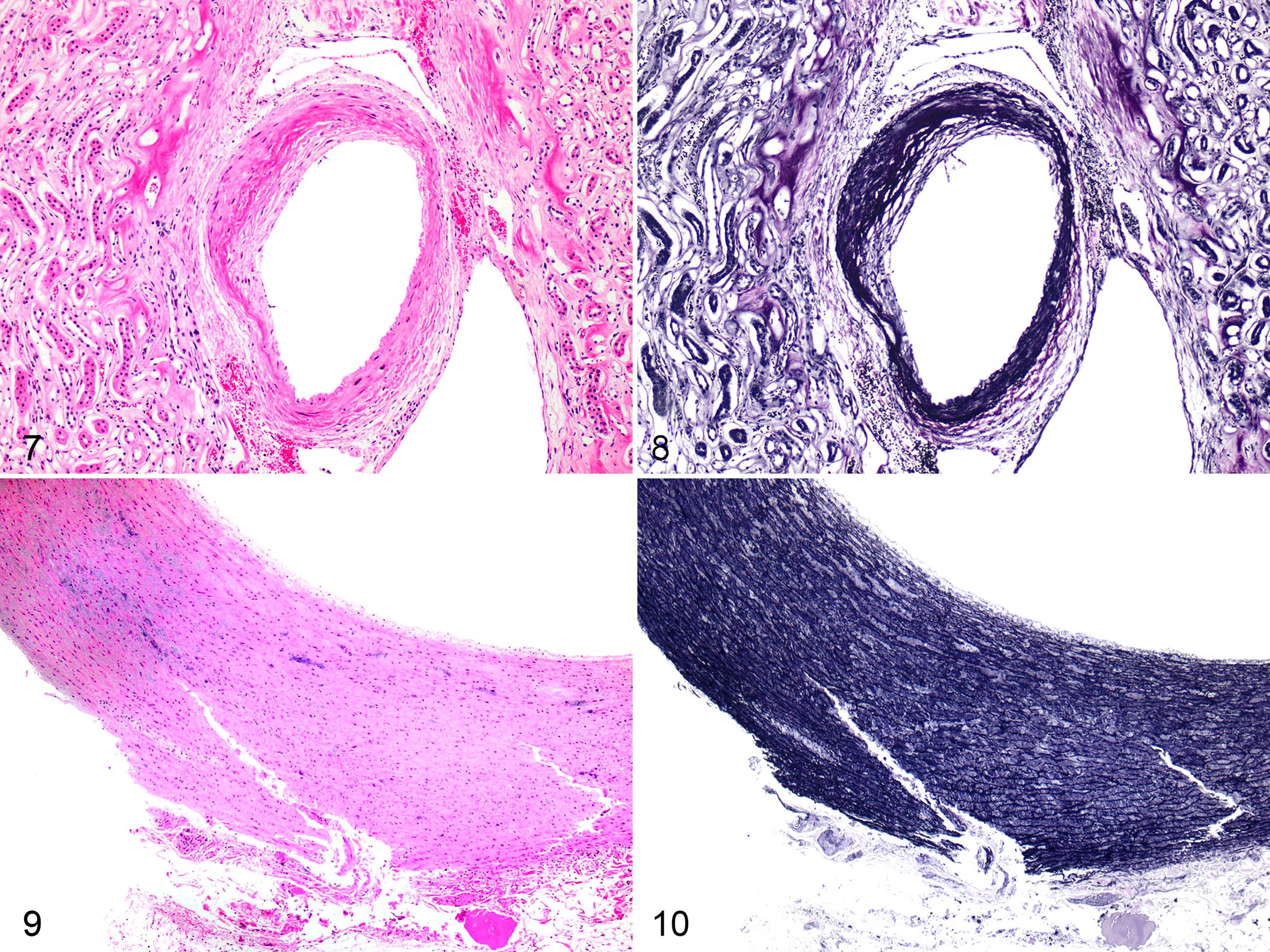
Renal arteriosclerosis in our cohort was characterized by medial hypertrophy and degeneration, fibrointimal hyperplasia, and adventitial proliferation affecting interlobar, arcuate, interlobular arteries, and/or peritubular arterioles (Figs. 7, 8). Comparison of VV scores and renal vascular scores revealed a significant positive correlation (Pearson’s R 2 = 0.63; P < .00001) (Fig. 12). The relationship between VV scores and renal vascular scores was stronger when cats with concurrent renal lesions such as segmental glomerulosclerosis and lymphoplasmacytic interstitial nephritis were removed (Pearson’s R 2 = 0.72; P < .0002) (Fig. 12). The VV scores (mean ± SD) were 25.3 ± 3 (n = 5) for animals with high renal scores, 17.1 ± 7.5 (n = 9) for animals with medium renal scores, and 8.3 ± 6.3 (n = 9) for animals with low renal scores (Fig. 13). The differences in the means of these groups were significant (P = .0002, ANOVA). These renal scores were significantly correlated to the presence of HT (P = .0007, ANOVA) (Fig. 14), and there was a significant difference between renal scores in HT and non-HT animals (P = .0006, Student t test).
When comparing only severe VV scores (≥15) and severe renal scores (≥9), the positive predictive value (the probability that cats with severe VV scores also had severe renal scores) was 53.8%. The negative predictive value (the probability that absence of VV lesions was coincident with absence of renal vascular lesions) was 100%. Lesions of VV arteriopathy were predictive of renal arteriosclerosis with 100% sensitivity, while specificity was only 64.7%. AUC was 91.1% (95% CI, 71.7%–98.9%; z = 6.82, P < .0001) (Table 1, Suppl. Fig. S2). Youden’s J index equaled 0.81 using a criterion index of >19.5 with a sensitivity of 100% and a specificity of 81.3%. Parameters for positive predictive value and specificity were improved by enlarging the allowable renal scores to include moderate lesions (score ≥4) (Table 1). These data suggest that VV lesions are not confounded by renal disease and that VV lesions around the great vessels are predictive of lesions in the renal vasculature. Importantly, while both renal arteriosclerosis and VV arteriopathy may occur in hypertensive cats, VV lesions were better correlated and more predictive of HT than was renal vascular disease.
VV Arteriopathy Correlates With and Is Predictive of Degenerative Lesions of the Great Vessels
Degeneration of the aorta in our cohort was characterized by cystic medial degeneration with mucinous change, medial necrosis with cyst formation, and fragmentation (Figs. 9, 10). Degenerative lesions of the MPA included fibrointimal hyperplasia and medial sclerosis. We stratified the VV scores in the same manner as previously to determine if there was a significant difference in the presence of great vessel lesions between cats with low, medium, and high VV scores. There was significant difference between the means of these groups for aorta (P = .039) and main pulmonary artery (P = .023). In addition, comparing low VV scores to high VV scores for main pulmonary artery, the difference in means was significant at P = .002 (Fig. 15). Correlation analysis of the VV scores and great vessel scores revealed a significant positive relationship for both the aorta (R 2 = 0.28, P = .008) and main pulmonary artery (R 2 = 0.32, P = .004) (data not shown).
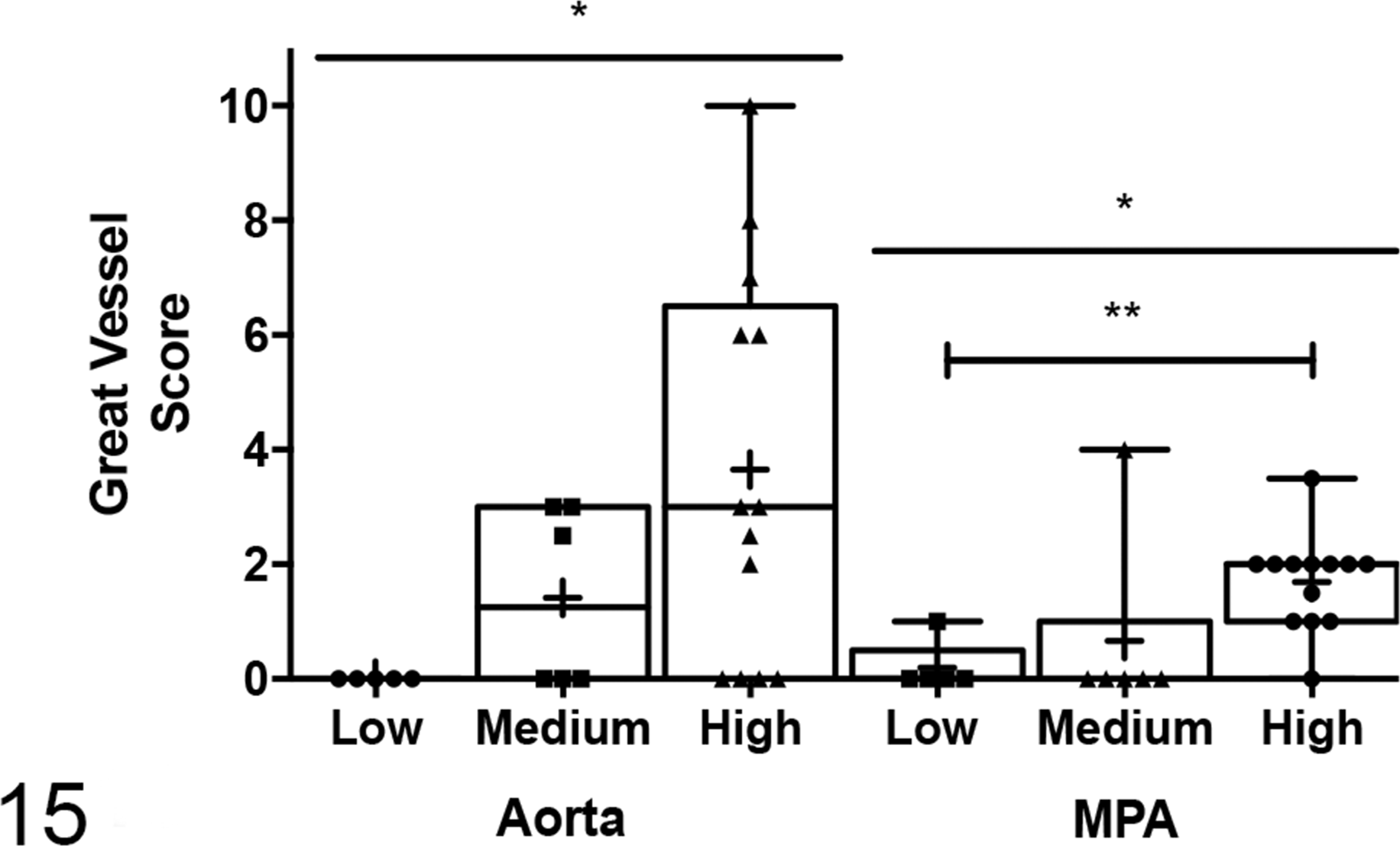
Cats with high vasa vasorum (VV) scores (n = 13) have significantly higher aorta scores than cats with low VV scores (n = 5), P = .0391. Cats with high VV scores have significantly higher main pulmonary arterial (MPA) scores than cats with low VV scores, P = .0227.
The positive predictive value of severe VV scores for the presence of aortic lesions was 69.2% vs 91.6% for lesions in the main pulmonary artery (Table 1). These data show that severe VV lesions are a risk factor for lesions in the great vessels in cats.
Discussion
This study was performed to characterize the morphology of arteriolar lesions in the VV of cats and compare the occurrence of these changes in cats with HT, renal arteriosclerosis, and degenerative lesions of the great vessels. We found that neovascularization was a common finding in cats with VV arteriopathy, that VV arteriopathy occurred in hypertensive cats, and that degenerative lesions in the great vessels also occur in the context of severe VV lesions compared to cats without these changes.
Hypertension in humans is a significant risk factor for aortic dissection, due to increased vessel wall stress secondary to local hypoxia. 12 Experimental interruption of VV flow in dogs leads to a decrease in distensibility of the aorta and chronically results in structural changes with loss of elasticity. 31 Aortic aneurysm and aortic dissection are uncommon occurrences in dogs and cats, with sporadic case reports in the literature. 11,22,37 Two case reports describe aortic dissection secondary to systemic hypertension in cats, 30,38 although the VV was not evaluated in these cases. Our hypothesis that neovascularization of the VV secondary to HT could predispose to degenerative changes in the great vessels was supported by the findings of increased VV scores in the HT cohort and a correlation of VV scores to degenerative lesions in the great vessels. Thus, as in humans, severe VV lesions in cats may predispose to the occurrence of aneurysm and dissection.
Chronic renal changes can confound vascular changes in cats with CKD. Alterations in the renal vasculature are noted in cats with CKD such as chronic hyperplastic arteriosclerosis, likely due to local changes in oxygen tension. 5 –7,10,34 It remains challenging to differentiate these chronic vascular changes associated with CKD alone from those lesions that are due to HT. CKD can result in HT, and also HT can contribute to the development of CKD. 10,24 We were therefore interested in determining if VV arteriopathy may be a more specific indicator of HT than renal arteriosclerosis, as renal arteriosclerosis may occur in healthy cats. 24 We found that VV arteriopathy correlated strongly with HT status. We also determined that VV lesions are a predictive and sensitive measure of HT status in cats. While renal scores correlated with HT status, the correlation and significance for VV score and HT were higher. In addition, we found that concurrent diseases such as HCM, CKD, and PAH did not affect the relationship between HT and VV scores. Due to the high predictive value and absence of significant confounding features, we suggest that VV lesions should be assessed postmortem in cats suspected of HT and that VV score may be more predictive of HT status than renal vascular lesions.
A challenge of this study was the evaluation of the VV, as minimal histologic and morphologic descriptions of this vascular bed are available in the veterinary literature. An interesting finding in this study was the prevalence of neovascularization in the VV of all HT cats. Neovascularization of the VV can be induced by pathologic conditions such as inflammation and atherosclerosis, as shown in a hypercholesterolemic pig model. 17,18,25 Neovascularization of the VV is also noted in cases of PAH and idiopathic pulmonary fibrosis in humans. 29,33 Pulmonary arterial adventitial fibroblasts activated by hypoxia respond by inducing angiogenesis in the VV endothelium. 14 Neovascularization is mediated by vascular endothelial growth factor (VEGF) signaling and fibroblast growth factor-2. 1,16 In HT, decreased VV blood flow is mediated by upregulation and release of vasoactive mediators as well as increased nuclear factor–κB signaling, which then stimulates angiogenesis in the VV. 29 This finding is confirmed in rat models of induced HT in which increased vascular density of the VV follows increased local expression of hypoxia-inducible factor 1-alpha (HIF-1α) and VEGF. 21 Hypertension is also found to increase the production of adventitial matrix. 29 Thus, neovascularization may represent a common morphologic change of VV compared to other vascular niches, with significant consequences for the pathogenesis of vascular disease.
The major limitation in the present study was the challenge of accurately determining HT status in these cats. Indeed, this is a limitation in clinical practice as well, even when blood pressure measurement is available. Studies of arterial blood pressure in clinical feline practice suggest high variability with currently available noninvasive devices. In addition, poor agreement is found when noninvasive measurements are compared to direct measurements, particularly in awake cats. 2,13 These inaccuracies in blood pressure measurement likely relate to variable stress responses between cats, limb movement during measurement and other technical factors, and the lability of blood pressure measurement throughout the day. 4 Thus, the blood pressure measurements that were available for 25% of our cohort may be unreliable, and the histologic determination of suspect HT may have been inaccurate. Every attempt was made to be as rigorous in our definition of HT as possible, including investigation of medical records for diagnoses or treatment history for HT and evaluation of target organs such as retinal and meningeal vasculature for “classical” lesions of HT. 3,10,36 While clinical documentation of HT was not available for all cats, we believe that the hypothesis of our study and the clinical relevance for future work relate to cats with systemic hypertension and not just multisystemic arteriopathy or vascular lesions typical of HT. And despite these limitations, we found that the stratification and distribution of VV scores between what we classified as HT vs non-HT or uncertain were significant. One possible way to mitigate this limitation would be to evaluate the VV of cats with experimentally induced hypertension undergoing telemetric measurement of arterial blood pressure, and this avenue is currently being pursued for future study. We also had a high proportion of cats with a diagnosis of HCM (33% of our cohort) (41.6% of our cohort). This higher incidence than expected for the general population is likely due to the initial selection bias of cats that are necropsied at our diagnostic service and furthered by the inclusion criteria of cats that were selected for this study (older cats without systemic inflammatory diseases). However, we found that the diagnosis of HCM did not confound our analysis.
The VV is an extensive vascular network supplying oxygen to large vessels throughout the body and plays a key role in the development of many vascular diseases. 14,29,32 An understanding of the role of the VV in vascular diseases of domestic species is lacking. Lesions of the VV could reflect a critical vascular niche in the pathogenesis of HT and PAH, atherosclerosis, and aortic dissection. Histologic evaluation of this tissue should be incorporated into any thorough investigation of systemic vascular disease in cats. This study is the first to examine the morphology of the VV in cats. We conclude that the VV is an important responder to HT in cats and that this lesion has significant implications for the integrity of the great vessels.
Footnotes
Acknowledgements
We acknowledge helpful discussions with Drs Duncan Russell and Rachel Cianciolo. We thank Dr John Bonagura for assistance with statistical analysis. We also thank Tim Vojt for assistance with figure design and compilation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.