
Abstract
Splenitis is uncommonly reported in dogs. Herein, the authors describe its prevalence, clinical findings and outcomes, histologic patterns, and causes. Splenic samples of dogs diagnosed with splenitis between 2005 and 2013 were collected and stained with hematoxylin and eosin, Gram, green-Gram, Giemsa, periodic acid–Schiff, and Ziehl-Neelsen. Samples were processed for polymerase chain reaction (PCR) to detect bacteria, fungi, and protozoa (Leishmania infantum, Hepatozoon canis). Thirty-three of 660 splenic samples (5%) had splenitis. Clinical findings and outcomes were available in 19 dogs (58%); 49% had weakness, 33% had fever, and 84% survived. The most frequent inflammatory patterns included purulent splenitis (27%), pyogranulomatous splenitis (24%), and neutrophilic perisplenitis (15%). One dog had a putative diagnosis of primary splenitis; in 8 dogs, microorganisms were identified histologically or by PCR in the spleen without obvious comorbidities. Twenty-four dogs (73%) had concurrent diseases; a permissive role in the development of splenitis was suspected in 21 of these cases. Histologic examination identified the cause of splenitis in 10 dogs. Bacteria were identified by PCR in 23 cases, but the bacteria were confirmed histologically in only 6 of these. Leishmania was detected with PCR in 6 dogs. Leishmania was identified in 1 dog and H. canis in another histologically, but both were PCR negative. Fungi were identified in 8 spleens by PCR and in 1 by histology. This study suggests that splenitis is uncommon in dogs and is frequently associated with systemic diseases. Prognosis is favorable in most cases. Identification of bacteria, fungi, and protozoa in the spleens of affected dogs with PCR should be interpreted cautiously, because the findings are not confirmed histologically in many cases.
The spleen is a secondary lymphoid organ as are lymph nodes and mucosa-associated lymphoid tissues. It is formed by the red and white pulp; the first harbors numerous macrophages and dendritic cells that are part of the reticuloendothelial system, whereas the latter contains B and T lymphocytes and dendritic cells. Both take part in the immune response and react to pathologic insults, ranging from infectious to neoplastic diseases. 51 Non-neoplastic diseases of the spleen are commonly described in dogs; on the basis of the current literature, their prevalence among all splenic diseases ranges from 35% to 70%. 7,10,11,20,47 Amyloidosis, congestion, hemorrhage, hematomas, infarction, necrosis, siderotic plaques, splenitis, thrombosis, torsions, and traumatic ruptures are included among non-neoplastic disorders. 47
Splenitis is an inflammatory process of the splenic parenchyma that is uncommon in dogs. Survey studies of splenic diseases in this species have reported a prevalence of splenitis ranging from 0.9% to 8%. 7,20 Among its causes, splenitis was described in only single case reports associated with fungal, 2,5,14,25,34,45,46,52 protozoan, 3,18,29,39 or bacterial 1,2,6,12,17,31,40,42,48 infections.
The cases related to fungal infections invariably had poor prognosis. In these dogs, necropsy identified splenomegaly and multiple foci of necrosis, while histology documented pyogranulomatous inflammation, multinucleated giant cells, and, in some cases, fungal hyphae. Fungi that have been identified in dogs with splenitis are Monocillium indicum, 25 Scedosporium prolificans, 14 Scopulariopsis chartarum, 52 Aspergillus terreus, 34 Cryptococcus neoformans, 8 Candida albicans, 5 Ochroconis gallopavum, 46 Xylohypha bantiana, 43 and Acremonium spp. 45
The protozoa identified in dogs with splenitis include Neospora caninum, 18 Hepatozoon canis, 3,16 Trypanosoma cruzi, 29 and Leishmania chagasi. 36,39,50 L. chagasi and Leishmania infantum, responsible for leishmaniasis in the New World and Old World, respectively, are considered genomically indistinguishable and therefore synonymous. 27 Lesions of the spleen of dogs with leishmaniasis are characterized by thickening of trabecular regions, granulomatous reaction and hemorrhagic areas, atrophy of lymphoid follicles and marginal zone, abundant macrophages with amastigotes in the cytoplasm, and perisplenitis. 36,39,50
Considering bacterial splenitis, dogs with Staphylococcus spp., 1 Mycobacterium avium Mycobacterium tuberculosis, 6,17,26,31 Listeria monocytogenes, 42 Bartonella henselae, and Bartonella vinsonii, 40 Clostridium spp., 2 Bacillus anthracis, 28 Burkholderia pseudomallei, 48 and multiple bacterial infection 11 have been described; in these cases, histologic lesions of the spleen are generally pyogranulomatous 6,40 or neutrophilic. 2 Splenic abscesses, likely due to bacterial infection, have been described in some dogs. 1,10,12 Interestingly, in one study, it was shown that bacteria were cultured from 35% of surgically excised spleens irrespective of the disease affecting the organ, and the most commonly identified bacteria include Staphylococcus spp., Enterococcus spp., and Klebsiella pyogenes. 37 Prognosis for bacterial and protozoan splenitis is generally better than that of fungal origin, although it may vary according to the causative microorganism and individual factors.
The aims of this study were to define the prevalence of splenitis in dogs, describe clinical findings and outcomes, characterize histologic patterns of splenic inflammation, and investigate possible causes.
Materials and Methods
Cases and Clinical Data
Splenic biopsies and case histories of dogs collected at necropsy or at surgery after splenectomy and partially or entirely submitted to the Department of Comparative Biomedicine and Food Sciences of the University of Padua between 2005 and 2013 with histologic diagnoses of splenitis were retrieved from the archives and included in the study. Because of the retrospective nature of the study and because most dogs were not admitted at authors’ institutions, clinical data were often incomplete or entirely missing. Owners were therefore contacted to retrieve further information. In particular, a telephone-based questionnaire was used, with the following questions: (1) What clinical signs did the dog present at admission? (2) Was the dog affected by other diseases? (3) what was the final diagnosis, other than splenitis? (4) what was the treatment of the dog after splenectomy? and (5) How long did the dog survive following surgery?
Histology
From each paraffin-embedded splenic sample previously fixed in 10% neutral-buffered formalin, 6 consecutive sections of 4 μm were obtained and mounted on slides. The first section was stained with hematoxylin and eosin, and the others were stained with Giemsa, and/or periodic acid–Schiff, Ziehl-Neelsen, Gram, and green-Gram (see Supplemental Materials). Findings were classified according to the type and localization of inflammation (Supplemental Table 1). Tissue sections were also examined to identify bacteria, protozoa, or fungi. All slides were assessed by 2 pathologists (S.F., M.C.), and any difference in diagnosis was resolved by consensus.
Molecular Analysis
Total deoxyribonucleic acid (DNA) from splenic samples was purified (see Supplemental Materials) from formalin-fixed paraffin-embedded splenic tissue.
Polymerase chain reaction (PCR) was used to assess the presence of microorganism in the spleen. Detection of bacterial and protozoan infections was achieved as previously described. 21,22,32 The protocol for fungal PCRs was as follows: 15 minutes of denaturation at 95°C, 40 cycles at 94°C for 1 minute, 51°C for 1 minute, and 72°C for 1 minute, and a 10-minute final extension at 72°C. Amplified ribosomal DNA restriction analysis was used to amplify the 16 S ribosomal ribonucleic acid (rRNA) of bacteria. Identification of bacteria was performed on an approximately 310-bp fragment of the 16 S rRNA gene using primers 16SUNI-L and 16SRNAV-S, and sequencing was performed according to a previously established protocol. 21
Fungal internal transcribed spacers (ITSs), highly conserved RNA sequences located between 2 areas of rRNA, were amplified to detect mycotic agents. 15 In addition, identification of fungi was performed on an approximately 330-bp fragment of the ITS region 2 using primers ITS3 and ITS4. 35
For protozoa, the analysis was performed to identify L. infantum and Hepatozoon spp. The target sequence for Leishmania was LT1 of the conserved region of the circular kinetoplast DNA; the primers used were RV1 (forward, 5′-CTTTTCTGGTCCCGCGGGTAGG-3′) and RV2 (reverse, 5′-CCACCTGGCCTATTTTACACCA-3′), with a reported sensitivity of 100% in detecting Leishmania infections. 22 To detect the presence of Hepatozoon spp., a partial sequence of 18 S rRNA, common to different species of Hepatozoon, was amplified. The primers used were HepF (forward, 5′-ATACATGAGCAAAATCTAAC-3′) and HepR (reverse, 5′-CTTATTCCATGCTGCAG-3′). 32 All PCR products were submitted to electrophoresis in an 0.8% agarose gel and stained with ethidium bromide; an ultraviolet transilluminator was used to visualize the different bands.
Immunohistochemistry
A monoclonal mouse anti-KMP11 antibody (dilution 1:300; Abcam, Cambridge, UK) was used to confirm the presence of L. infantum in all PCR-positive cases. Sections were incubated with the antibody for 24 minutes at room temperature. A canine splenic biopsy specimen previously proved to have Leishmania spp. amastigotes in macrophages served as a positive control. Immunohistochemistry was performed with an automatic immunostainer (Ventana Benchmark XT; Roche Diagnostics, Monza, Italy) using a secondary antibody with a horseradish peroxidase–conjugated polymer (ultraViews Universal DAB; Ventana Medical Systems, Tucson, AZ).
Results
Clinical Findings
Thirty-three dogs were included in the study, with a median age of 8.5 years (range, 2–15 years). Seventeen dogs were intact males (51%), 7 were intact females (21%), 6 were spayed females (18%), and 2 were neutered males (6%); sex was unknown in 1 dog. Ten dogs were mixed breed dogs (30%) and 23 were pure breeds (70%), including 6 German Shepherds (18%); 2 (6%) each Great Dane, Italian Hound, Boxer, Rottweiler, and Labrador Retriever; and 1 (3.0%) each English Bulldog, English Setter, Dachsbrake, Griffon, Airedale Terrier, Doberman, and Doberman Pinscher.
According to the available clinical data and questionnaires, presenting signs at the time of splenectomy or necropsy were known for 28 dogs. Severe and acute weakness was observed in 16 dogs (48%), hyperthermia in 11 (33%), weight loss in 6 (18%), and painful abdomen and vomiting in 4 (12%). Twenty-five animals underwent abdominal ultrasound that identified splenic masses or nodules in 14 dogs (56%); peritoneal effusions in 8 (32%), consistent with purulent peritoneal exudate in 2; altered echotexture of the spleen or nonsplenic abdominal masses in 4 each (16%); pyometra or endometritis, splenic torsion, or testicular nodules in 3 dogs each (12%); and portal vein and splenic vein thrombosis, prostatic nodules, hepatomegaly, and hypoechoic hepatic nodules in 1 dog each (4%). Twelve dogs had more than 1 ultrasonographic alteration. In the remaining dogs, abdominal ultrasound was not performed, because physical examination allowed diagnosis of gastric dilation-volvulus or abdominal masses were palpated.
Among the 33 dogs, 24 (73%) were diagnosed with additional non-splenic conditions, including 8 (24%) with peritoneal effusion, 6 (18%) with neoplastic diseases (1 dog each with peritoneal hemangiosarcoma, testicular seminoma, fibrohistiocytic nodule, hepatic cystadenoma with concurrent testicular seminoma, metastatic mammary carcinoma, and hepatocellular carcinoma), 5 (15%) with gastric dilatation-volvulus, 3 (9%) with pyometra or endometritis, 3 (9%) with splenic torsion, 2 (6%) with granulomatous hepatitis (in 1 case due to leishmaniasis), and 1 (3%) each with idiopathic hepatic lobar torsion, gastric ulcer, systemic fungal infection, immune-mediated hemolytic anemia, recent trauma, hemorrhagic gastroenteritis, cholangiohepatitis, and portal vein thrombosis. Eight dogs were concurrently affected by more diseases, and 9 dogs (27%) did not show any disease other than splenitis.
Information on outcomes was available for 19 dogs. The dog with systemic mycosis died a few days after admission. The remaining 18 dogs underwent surgery and were then treated with different antibiotics; 16 (89%) survived to discharge, and 2 (11%) died during hospitalization because of surgical complications at 7 and 40 days after surgery, respectively. Of the 16 surviving dogs, 6 (38%) are still alive at the time of writing, and 10 (62%) died of causes unrelated to splenitis, with a median survival of 2.5 years (range 1–3.5 years).
Histologic Findings
The 33 cases of splenitis were classified histologically (Supplemental Table 1). In particular, 9 dogs (27%) had purulent splenitis (Figure 1), 8 (24%) had pyogranulomatous splenitis (Figure 2), 5 (15%) had neutrophilic perisplenitis (Figure 3), 4 (12%) had neutrophilic perisplenitis and splenitis, 3 (9%) had granulomatous splenitis (Figure 4), 2 (6%) had neutrophilic splenitis (Figure 5), and 1 dog each (3%) had fibrinous-suppurative perisplenitis and splenitis, and fibrinous-suppurative perisplenitis (Figure 6). In 1 dog affected by purulent splenitis and in 1 affected by pyogranulomatous splenitis, splenic abscesses were identified.
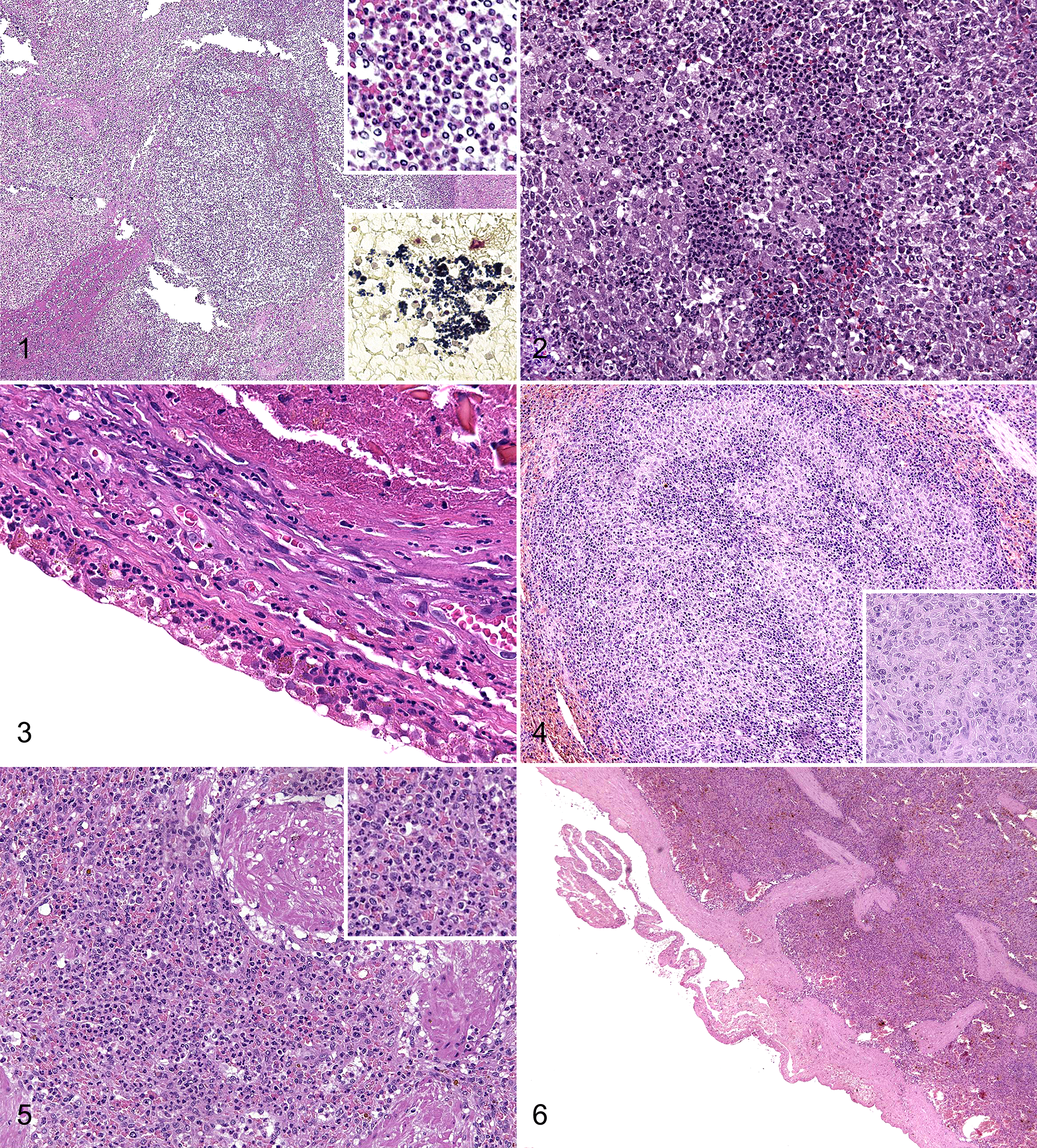
Of the 9 dogs with purulent splenitis, 6 yielded positive results with Gram staining (67%) (Figure 1); in particular, Gram-positive cocci were identified in 3 dogs and Gram-negative cocci, concurrent Gram-positive cocci and bacilli, and concurrent Gram-negative and positive cocci in 1 dog each.
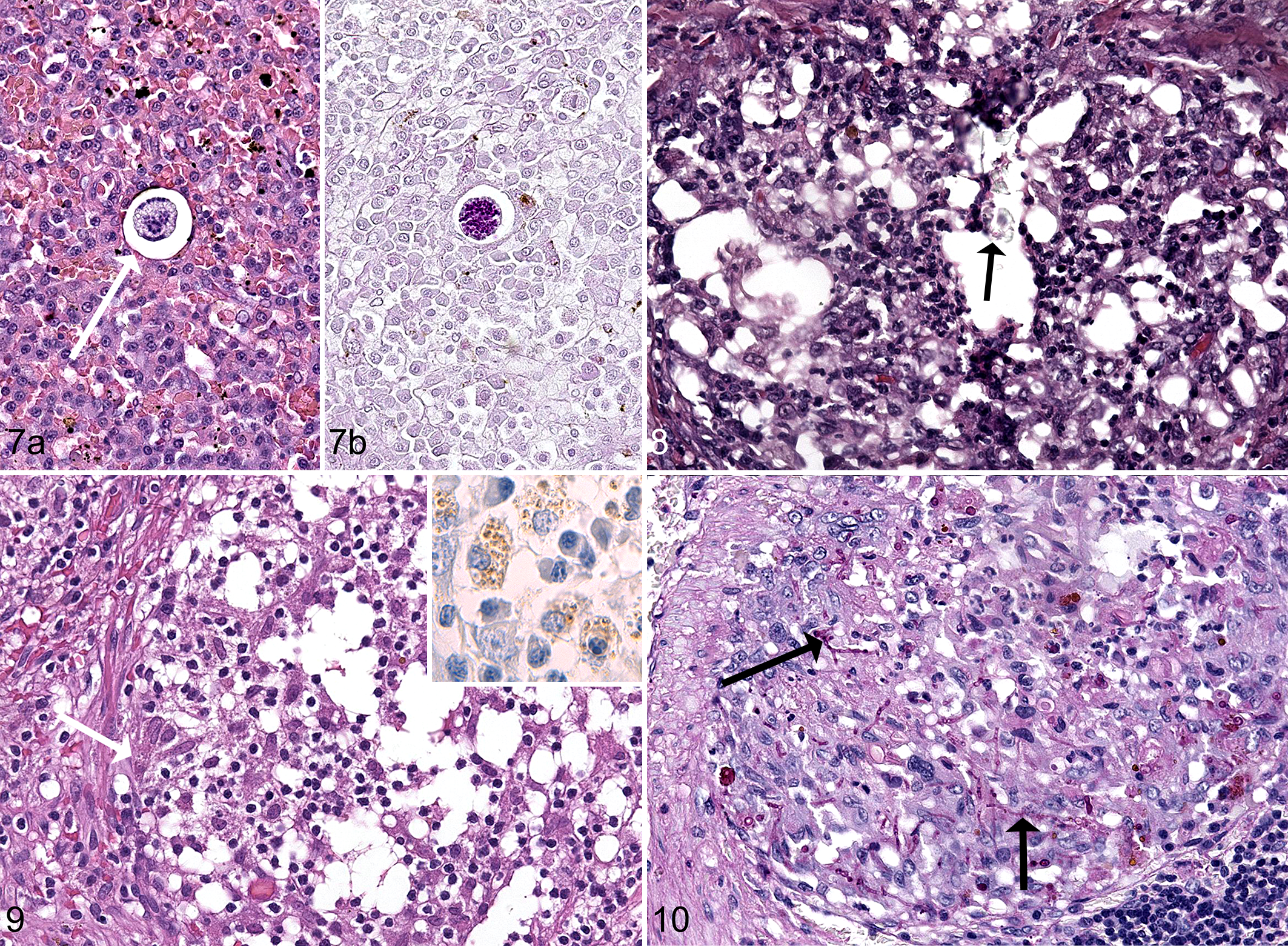
Among the 8 cases of pyogranulomatous splenitis, meronts of Hepatozoon canis were identified in 1 dog (Figure 7) and intra- and extracellular material compatible with exogenous material in another dog (Figure 8). Among the 3 cases of granulomatous splenitis, amastigotes of L. infantum (Figure 9) and fungal hyphae (Figure 10) were identified in 1 dog each. Twenty-four splenic samples yielded negative results for infectious agents on the basis of microscopic examination.
In total, 11 dogs presented histologic signs of altered splenic circulation consistent with splenic hemorrhage, splenic hematomas, splenic vein thrombosis, and splenic torsion. In particular, these conditions affected 4 dogs with neutrophilic perisplenitis and splenitis, 3 dogs with neutrophilic perisplenitis, and 1 dog each with fibrinous-suppurative perisplenitis and splenitis, granulomatous splenitis, fibrinous-suppurative perisplenitis, and pyogranulomatous splenitis.
PCR
Bacterial pathogens were identified by PCR in 23 dogs (Supplemental Table 2). Pseudomonas spp. DNA was identified in 19 dogs, Propionibacterium spp. and Clostridium haemolyticum in 1 dog each, and mixed bacterial populations in 2 dogs. Among these 23 dogs, histologic diagnoses were neutrophilic or purulent-suppurative perisplenitis and splenitis in 12 dogs (52%), granulomatous or pyogranulomatous splenitis in 9 dogs (39%), and fibrinous-suppurative inflammation in 2 dogs (9%).
On the basis of histologic findings, bacterial infection was confirmed in only 3 of these 23 dogs: in particular, 1 Great Dane affected by gastric dilation-volvulus had mixed bacterial infection identified by PCR analysis, and histology identified Gram-positive cocci; 1 Griffon with purulent peritoneal exudate and free abdominal gas had C. haemolyticum identified by PCR analysis, while histology identified cocci; and 1 Doberman Pinscher affected by endometritis had Pseudomonas spp. infection identified by PCR analysis, and histology identified both Gram-positive and Gram-negative cocci.
Of the 19 Pseudomonas spp. PCR-positive dogs, 8 had concurrent infections on the basis of PCR analysis or histology: 4 dogs with L. infantum and 4 with fungal infection (Cryptococcus spp. in 2 dogs, Cladosporium spp. and Rasamsonia argillacea in 1 dog each). One of the 2 dogs with a mixed DNA bacterial population was positive for Exophiala xenobiotica by PCR. Other fungi identified by PCR in dogs with concurrent bacterial infection were Truncatella angustata and Bipolaris cynodontis (1 dog each).
Overall, fungal DNA was amplified in 8 dogs (24%); in addition to the 7 above described, the DNA of a not previously cultured fungus was identified in a dog. The corresponding histologic diagnoses of these 8 spleens were consistent with purulent splenitis in 4, granulomatous or pyogranulomatous splenitis in 3, and neutrophilic perisplenitis in 1.
Six dogs (18%) were positive for L. infantum DNA; 4 presented concurrent infections, including Pseudomonas spp. in 3 dogs and Cladosporium spp. in 1 on the basis of PCR, and histologically visible Gram-positive cocci in 1 dog. The histologic diagnoses suggested neutrophilic perisplenitis in 2 dogs and neutrophilic perisplenitis and splenitis, purulent splenitis, fibrino-suppurative, and pyogranulomatous splenitis in 1 dog each. None of these dogs was positive by immunohistochemistry for L. infantum infection, and it was not possible to identify L. infantum amastigotes histologically. None of the dogs yielded positive results for Hepatozoon spp. using PCR.
Discussion
To our knowledge, this is the first comprehensive study of splenitis in dogs. In the present series, 33 dogs had histologic diagnoses of splenitis, representing 5% of all submitted spleens. This prevalence is similar to that previously described by other investigators and confirms that splenitis is uncommon in dogs. 7,20 Clinical and diagnostic findings of splenitis are unspecific or related to the associated disease, and therefore, its diagnosis relies on histology.
Only 1 dog with splenitis of the present series had no concurrent systemic disease and yielded negative results in all tests. Hence, the dog had a tentative diagnosis of primary splenitis. In 8 other dogs, although no obvious systemic disease was present, PCR and histology identified bacterial, fungal, or protozoan infection of the spleen. In these dogs, PCR identified Pseudomonas spp., an unknown fungus, Cladosporium spp., or L. infantum, and histology allowed observation of meronts of H. canis. The actual role of the above microorganisms in the pathogenesis of splenitis remains unclear because systemic involvement was not identified. Thus, it cannot be excluded that in some the microorganisms merely represented passive bystanders or contaminant, rather than the cause of splenitis.
Concurrent diseases were very frequent, present in 24 cases (73%). For most, an explanation for splenitis was deemed possible. Six dogs had neoplastic diseases that might be considered to play a causative role in the development of splenitis. For instance, hemangiosarcoma and mammary adenocarcinoma have been shown to predispose to thrombosis and to alter vascular anatomy, possibly favoring bacterial engraftment. 23 In the present series, 2 dogs had these tumors, and both had vascular splenic lesions detected together with splenitis. Two other dogs had liver neoplasia; hepatic tumors have been sometimes associated with liver abscesses in dogs, likely because of increased tissue susceptibility to bacterial growth, which in turn might cause bacteremia and subsequent splenitis. 44 Five dogs presented gastric dilation-volvulus, and all had splenitis along with splenic vascular abnormalities. We hypothesize that in these cases, as gastric dilatation-volvulus develops, normal splenic vascularity and blood supply is progressively compromised, thus generating splenic inflammation. In addition, bacterial translocation from the gut, which is observed in up to 43% of cases with gastric dilatation-volvulus, 53 might have had a primary role in the establishment of splenitis. In addition, splenic inflammation was likely associated with bacterial translocation in the 6 dogs affected by pyometra, endometritis, hemorrhagic gastroenteritis, gastric ulcer, purulent peritoneal effusion, and hepatic lobar torsion. Propionibacterium spp. DNA was amplified in 1 dog affected by pyometra; this bacterium has been previously associated with pyometra in a woman and was shown to translocate into the bloodstream in healthy dogs undergoing ovariohisterectomy. 9,55 It is remarkable that the blood reaching the spleen originates only from the arterial supply of the systemic circulation (ie, splenic artery), and, differently from the liver, no venous blood from the gastrointestinal tract flows directly through the organ in dogs; hence, if pathogens translocate from the gut, to reach the spleen and cause splenitis, they have to pass the liver, lungs, and heart and eventually reach the systemic circulation. 4
One dog presented laboratory signs compatible with intravascular hemolysis. This dog had splenic torsion and was PCR positive for L. infantum; both conditions might have triggered splenitis because of altered vascularity and blood supply or activation of the reticuloendothelial system and likely caused anemia. 33,41 Five other dogs had granulomatous hepatitis with L. infantum amastigotes or Pseudomonas spp., exogenous material, systemic R. argillacea, and abdominal trauma; all of these conditions might have led to splenitis. A clear association between the concurrent disease and splenitis was not evident in only 3 dogs.
The potential cause of splenitis was identified histologically in 10 dogs. Specifically, in 4 cases with pyogranulomatous or granulomatous splenitis, exogenous material, fungal hyphae, H. canis, and L. infantum were identified. It is interesting to note that of the latter 3, PCR yielded R. argillacea in the dog affected by systemic mycosis, whereas in the other 2 it did not amplify H. canis or L. infantum DNA. Searching for the 2 protozoa failed, probably because of the paucity of microorganisms in the sample. In 6 dogs with purulent splenitis, bacteria were histologically visible. Of these, only 3 had bacterial DNA amplified by PCR, including 1 each with Pseudomonas spp., C. haemolyticum, and a mixed population. In the remaining 23 dogs, showing a variety of histologic patterns, no pathogens were identified histologically within the splenic parenchyma. Therefore, on the basis of these findings, histology is able to identify the cause of splenitis in only about one third of cases.
Conversely, PCR amplified bacterial DNA in 23 dogs, but bacteria were observed by histology in only 3 cases, as already mentioned. It is therefore possible that PCR performed on paraffin-embedded splenic samples leads to various positive results because of its elevated sensitivity. However, some of the positive results might have been due to contamination of samples with environmental bacteria or to the presence of DNA fragments within macrophages and other cells of the spleen. The fact that 3 dogs had splenic bacteria on the basis of histology, but not PCR, indicates that false-negative results can occur with the latter. It is possible that DNA damage caused by formalin fixation and paraffin embedding of samples also reduced the sensitivity of the assay.
With regard to mycosis, in 8 dogs, fungal DNA was found by PCR, but the presence of hyphae was confirmed by histology in only 1 case; the large majority (ie, 7 of 8) presented neutrophilic or pyogranulomatous splenitis. The explanation for false-positive or false-negative PCR results for fungal infection is likely similar to those mentioned for bacteria. Concerning R. argillacea, it is worth noting that this fungus is considered an emerging pathogen in humans, causing chronic granulomatous disease and cystic fibrosis. 24,49 R. argillacea has been reported in only 2 dogs to date. 13,38 Other fungi identified in the present series were B. cynodontis, Cladosporium spp., Cryptococcus spp., E. xenobiotica, T. angustata, and an uncharacterized fungus. Among those that have never been described in dogs, B. cynodontis is a dematiaceous hyphomycete widely distributed in soil and normally associated with plant infection. It was recently associated with clinical disease in humans. 30 E. xenobiotica is an opportunistic fungus responsible for phaeohyphomycosis, in particular in immunocompromised humans. 56 T. angustata is a coelomycetous fungus, recently reported to cause subcutaneous infection in an immune-competent humans. 19 Because none has been reported in dogs, it cannot be excluded that they resulted from contamination of samples.
In relation to protozoa and PCR, 6 dogs yielded amplification of L. infantum DNA, and histologic diagnosis was neutrophilic splenitis and perisplenitis in 3 cases and fibrinosuppurative perisplenitis and splenitis, pyogranulomatous splenitis, and purulent splenitis with visible bacteria in 1 dog each. Except for the last case, similar histologic findings have been described in previous studies. 34,37,48 It is noteworthy that all PCR-positive dogs had negative results with immunohistochemistry. It is thus possible that some splenic macrophages had phagocytosed DNA fragments, but that intact amastigotes were not detectable. The amplification methods used with PCR allow positive results with very small amounts of DNA, while this is not achievable by means of immunohistochemistry. In a prior study of canine skin biopsies, PCR testing for leishmaniasis yielded sensitivity of 82.8%, whereas the sensitivity of immunohistochemistry was 62.1%. 54 None of the dogs in the present study were H. canis positive with PCR. The single dog with H. canis on histology did not display obvious clinical signs, perhaps because of the low parasitic burden.
In 19 dogs, it was possible to collect data on outcomes. Of these, 84% survived surgery and 37% are alive at the time of writing. The median survival of dogs that were followed until death was 2.5 years (range, 1–3.5 years); in these dogs, deaths were unrelated to the previous disease. The prognosis for dogs affected by splenitis can therefore be considered good.
There were some limitations to the present study that need to be mentioned. Because of the retrospective nature of the investigation and the fact the cases came from different institutions, information gathered from available medical records were often incomplete. In addition, samples were retrieved from archives, and prior contamination cannot be excluded.
Conclusion
Splenitis is an uncommon disease in dogs; clinical signs are vague, and concurrent diseases that might predispose to splenic inflammation are generally present. Prognosis is favorable in the majority of cases. Identification of bacteria, fungi, and protozoa in the spleens of dogs with splenitis should be interpreted cautiously if PCR is used, because histology does not provide supportive evidence of infection in many cases. Furthermore, the histologic classification used in the present study is expected to be helpful for future investigations, either for clinicians or pathologists.
Footnotes
Acknowledgements
We thank Dr Rossella Zanetti and Dr Emilia Cavicchioli for excellent technical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.