
Abstract
Asphyxia in a forensic context refers to death by rapid cerebral anoxia or hypoxia due to accidental or nonaccidental injury. Death due to nondrowning asphyxia can occur with strangulation, suffocation, and mechanical asphyxia, each of which is categorized based on the mechanism of injury. Individuals dying due to various types of asphyxia may or may not have lesions, and even those lesions that are present may be due to other causes. The interpretation or opinion that death was due to asphyxia requires definitive and compelling evidence from the postmortem examination, death scene, and/or history. Beyond the postmortem examination, pathologists may be faced with questions of forensic importance that revolve around the behavioral and physiological responses in animals subjected to strangulation, suffocation, or mechanical asphyxia to determine if the animal suffered. While there is no prescriptive answer to these questions, it is apparent that, because of physiological and anatomical differences between humans and animals, for some mechanisms of asphyxia, consciousness is maintained for longer periods and the onset of death is later in animals than that described for people. Veterinary pathologists must be cognizant that direct extrapolation from the medical forensic literature to animals may be incorrect. This article reviews the terminology, classification, mechanisms, and lesions associated with asphyxial deaths in companion animals and highlights significant comparative differences of the response to various types of asphyxia in animals and people.
Keywords
To ancient Greeks, asphuxia meant “without pulse,” a definition that was transformed in the mid-19th century to denote “suffocation.” Although modern medical dictionaries often differ in their exact definition of asphyxia, all refer to oxygen deprivation. 36,91 Life depends on oxygen, and deprivation of oxygen causes cell injury or death due to decreased oxidative respiration. 71 The respiratory system’s primary function is to provide oxygen to tissues and remove carbon dioxide. 105 Effective respiration requires adequate environmental oxygen, the ability to inhale air into the lungs, oxygen and carbon dioxide exchange across the air-blood barrier, oxygen transport in the blood by binding of oxygen to hemoglobin in erythrocytes, and finally, release of oxygen into the tissues. Ventilation is controlled by the brainstem and is mediated by central and peripheral chemoreceptors and peripheral stretch receptors. 105 Ischemia, anoxia, and hypoxia result in the inability of cells to receive or use oxygen and remove carbon dioxide by different mechanisms. 83,86 Hypoxia is a generic term for reduced oxygenation, hypoxemia refers to low levels of oxygen in the blood, 7 and, similarly, anoxia is oxygen depletion, whereas anoxemia refers to no oxygen in the blood, 7 ischemia is reduction or cessation of blood flow to a tissue, 71 and histotoxic hypoxia is due to impaired tissue utilization of oxygen. 7 Glycolytic energy production can occur in hypoxic states but is abrogated with ischemia as the substrates for glycolysis do not reach the tissues 71 and waste products are not removed. 54 In contrast, oxygen delivery is impaired with hypoxemia, and waste products are removed. 7
Asphyxia can result from endogenous diseases such as anemia or pneumonia and exogenous physical, chemical, or environmental factors. In this article, asphyxia refers to death by rapid cerebral anoxia or hypoxia 96 due to accidental or nonaccidental causes.
The medical forensic pathology literature is replete with case reports, case series, reviews, and book chapters on asphyxia, whereas scant case reports 22,55,81 and few book chapters 25,77,83 on this topic exist in veterinary pathology. Morphologic and physiologic responses to injuries and asphyxia in reptiles, birds, fish, amphibians, or quadrupedal mammals may manifest differently from those described as characteristic in people. Anatomic variations in blood supply to the brain 29,49,79,122,135 affect the degree and duration of physiological responses of animals compared to people. 13 In 1897, Brouardel 18 stated “que la resistance des animaux aux divers genres d’asphyxie est plus grande que celle de l’homme” (“the resistance of animals to various kinds of asphyxia is greater than that of man”). For example, permanent brain damage in people occurs within 4 minutes of carotid artery occlusion 108 but takes 8 minutes in dogs with total occlusion of the cerebral circulation. 68 Even after 6 minutes of cerebral ischemia, dogs eventually recovered to full functionality in 1 experiment. 68
Questions of forensic importance in suspected asphyxia-related deaths not only relate to the anatomic lesions but often those pertaining to animal welfare and suffering: how long does it take for an animal to become unconscious and develop respiratory and cardiac arrest, when does irreversible cerebral damage occur, and what are the diagnostic criteria to establish that asphyxia was the mechanism of death? This article reviews physiological data from animals used as experimental subjects for various mechanisms of asphyxia. Because responses in animals may differ from those reported in people, veterinary pathologists must be cognizant that direct extrapolation from the medical forensic literature may be incorrect. The terminology and classification of asphyxia, mechanisms, and lesions associated with asphyxial deaths primarily in companion animals are also reviewed.
Asphyxia: Terminology and Classification
The classification of asphyxia in medical forensic pathology, including that promulgated by standard textbooks 9,33,35,84,108,117,119 and review papers, 19,78,84,103,117 is not standardized 111 and is highly variable. 103 The terminology and definitions as proposed by Sauvageau 111 (Table 1) are used in this article, although any of the above classification schemes may be used. Regardless of the classification system, asphyxia is considered a mechanism rather than a cause of death, 78,96 and for clarity, the pathologist should attempt to identify the underlying mechanism of oxygen deprivation. In many cases, this will require additional information from the death scene, history, or witness accounts. 14,96
Classification and Definition of Nondrowning Asphyxia.a
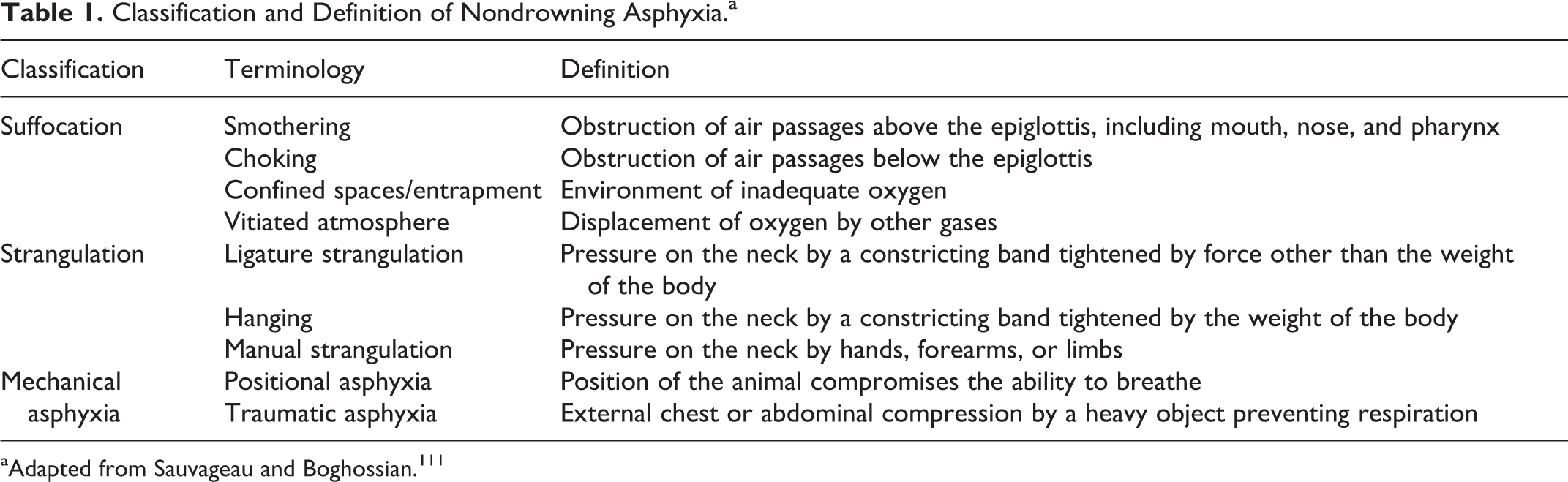
aAdapted from Sauvageau and Boghossian. 111
Other terms used in medical forensic pathology include burking, garroting, throttling, chokehold, and carotid sleeper hold. Chest compression combined with smothering is called burking after the 19th-century criminal W. Burke, who killed victims in this manner. 33 Garroting or throttling usually refers to ligature or manual strangulation, respectively, 108 although garroting was initially a method of legal execution in Spain. 66 A chokehold is a forearm or cylindrical object placed across the neck and pulled back with the other hand, causing airway compression and frequently laryngeal fractures, whereas with a carotid sleeper hold, the airway remains open while the carotid arteries are compressed. 119
Asphyxia: Differential Diagnostic Dilemmas, Myths, and Misconceptions
Despite the plethora of literature available, medical pathologists are frequently in a quandary regarding the diagnosis asphyxia-related deaths. 42,78,103 Depending on the mechanism, individuals dying due to asphyxia may or may not have lesions, and to further complicate the matter, the lesions of asphyxia may resemble those arising from other causes. 19,100,108 The 5 classic tenets of death due to asphyxia of cyanosis, fluidity of the blood, engorgement of the right ventricle, visceral congestion, and petechiae are now refuted and are often referred to as “the obsolescent quintet.” 19,78,85,96,103,108 Veterinary pathologists know that cyanosis, fluidity of the blood, and visceral congestion are common postmortem findings and are not etiologically specific.
Of the 5 lesions, petechiae are the most compelling indicator of fatal neck compression, 19,78,108 their presence indicating impaired venous return from the head. Increased intravascular pressure due to compression of neck veins and concurrent arterial flow ruptures postcapillary venules, 12,19,78,108 producing petechiae. 96 If the arterial vascular supply and venous return are completely obstructed, petechiae will not occur as blood is prevented from entering the tissue. The development of petechiae in fatal neck compression depends on the duration, consistency, and intensity of the force applied to veins and arteries, and if present, a detailed examination of the neck is warranted. Petechiae may be visible in tissues and mucous membranes anterior to the area of neck compression: in the skin, conjunctiva, sclera, larynx, and oral mucosa. 14,19,42,77,82,83,97 Mechanical or crushing trauma of the chest or abdomen causes marked congestion and petechiation cranial to the injury site. 19 Petechiae, however, are not specific lesions of fatal neck compression because strenuous sneezing, coughing, 19,46,108 vasculopathies, and coagulation disorders can also cause petechiae. 33 The disposition of the body, particularly if the animal was in an inverted position when found, is particularly important as congestion and petechiae can develop in dependent sites due to livor mortis. 103,108 Tardieu spots, a term used in the medical forensic pathology literature, specifically refers to subpleural petechiae 103,108,127 but is often used to describe petechiae in soft tissues to infer asphyxial death. 108,119 This eponymous term should be avoided in veterinary forensic pathology, and the distribution and location of petechiae should be described to avoid confusion and the implicit causal inference of this label.
Pulmonary edema with or without hemorrhage, atelectasis, and interstitial emphysema are common macroscopic and microscopic lesions in animal and human victims of strangulation and suffocation* but also occur with a myriad of other conditions. Proponents of semiquantitative morphologic analyses of histological sections claim that pulmonary lesions of strangulation, hanging, drowning, and suffocation can be distinguished in people 32,52 but do not address the effect of decomposition on histological detail. 94
Reflex cardiac arrest following neck trauma and stimulation of the carotid sinus is a presumptive mechanism of death currently debated by medical forensic pathologists, especially when anatomic lesions are absent. 6,34,42,96,114,119 A meta-analysis of hanging deaths in people concluded that concurrent underlying conditions such as cardiac disease, sympathetic stimulation, and/or drug abuse are present in suspected cases of reflex cardiac arrest. 114 Similarly, bradycardia with subsequent cardiac asystole as a result of vagal stimulation in cases of hanging has been argued for over 120 years. 23 In their review of the historical proposed mechanisms of death in hanging, Clement and coauthors 23 remarked that those who supported the concept of vagal stimulation considered it only as a potential but unproven mechanism of death. In some textbooks of forensic pathology, vagal stimulation is considered a mechanism of death resulting from strangulation or from foreign body esophageal occlusion, 35,108 but this is discounted by others because there is no supporting scientific proof. 33,96
The activation of both sympathetic and parasympathetic responses in experimental asphyxia 43,47,74 has been called a “brainstorm which accelerates premature death of the heart and brain.” 74 Autonomic conflict between sympathetic and parasympathetic responses was a postulated cause of cardiac arrest during cold water immersion in individuals with predisposing conditions. 107,116 Carbon dioxide–induced asphyxia accelerated the onset of cardiac arrest in rats by stimulating cortical neurotransmitter release, causing detectable and accelerated bidirectional corticocardiac communication that intensified as cardiac function deteriorated. 74 This autonomic cardiac toxicity was mitigated by removing the effects of the sympathetic but not the parasympathetic system. 74 Because vagal stimulation or carotid sinus trauma due to neck pressure is not proven to cause death, and neither mechanism is required for autonomic conflict to occur, it is the author’s opinion that veterinary pathologists should refrain from invoking these as potential mechanisms in asphyxia-related deaths. Vasovagal inhibition and reflex cardiac arrest, as stated by Pollanen, 96 are “probably better viewed as part of the folklore of forensic pathology rather than a robust concept based on scientific evidence.”
Strangulation
There are a few reports describing lesions of strangulation in domestic animals. 24,55,77,83 Accidents, intentional abuse, and occasionally a technique known as “helicoptering,” where the dog is lifted or swung off the ground as a method of punitive training, are situations in which an animal can be strangled. 16,55 Hanging, ligature, and manual strangulation cause neck compression. 111 Hanging requires that a neck ligature is tightened by the body weight, whereas ligature and manual strangulation are due to forces applied to the neck other than the weight of the individual’s body. 111 The duration, consistency, and type of applied force; the anatomic site of compression; and structures occluded all influence the physiological responses, the time until death, 66 and the lesions produced. 35,129 The larynx, trachea, jugular veins, common carotid, and vertebral arteries and their branches may be partially or totally occluded: death may be due to vascular obstruction and/or airway obstruction. 111 Pressures to occlude neck vessels and trachea in people are often quoted as 2 kg for the jugular veins, 5 kg for the carotid arteries, 15 kg for the trachea, and 30 kg for the vertebral arteries, 33,117 even though these values were determined by experiments on cadavers well over a hundred years ago. 112 It is not known if these absolute values are applicable to animals, but they likely reflect the relative amount of pressure required to obstruct the vessels and trachea. In hanging, the dynamics, including where a ligature is placed and angle of the head acting as a fulcrum, will affect the amount of force needed to occlude the vessels. 136 Irreversible cerebral damage occurs in dogs when the arterial oxygen drops below 20 to 23 mm Hg and the cerebral blood flow is below 10 mL/100 g/min. 54,70 If arterial oxygen is less than 45 mm Hg, heart failure and systemic hypotension will affect cerebral perfusion. 95
Species Differences in the Vascular Supply to the Brain
Species differences in vascular anatomy and blood supply to the brain affect the physiological responses to strangulation. Because numerous extracranial and intracranial arterial anastomoses in dogs and cats makes them far less susceptible to cerebral ischemia than people, veterinary pathologists must be aware that occlusion of the internal carotid artery in dogs and cats does not have the same, rapid, and significant effect on cerebral blood flow as is reported in humans. In people, the brain is supplied by the internal carotid and vertebral-basilar arterial systems. 50,51 Compression of the carotid arteries in people causes rapid unconsciousness 129 as the vertebral arterial circulation is insufficient to maintain cerebral blood flow and function. 78 In contrast, ligation of both common carotid arteries in nonanesthetized dogs, pigs, goats, and calves does not produce neurological deficits or even a change in behavior. 80 In dogs and cats, the maxillary and vertebral arteries contribute significantly to the cerebral blood supply. 51,120 It is difficult to occlude the vertebral arteries, 63,68 and even when occluded, the numerous extracranial vascular anastomoses in dogs and cats maintain an adequate vascular supply to the brain. † Dogs will survive simultaneous ligation of all common carotid and vertebral arteries, and cerebral global ischemia is not produced 5,49,99,135 unless severe hypotension is also created. 99
Physiological Responses in Strangulation
In people, the pathophysiology of hanging is unclear, as death may be caused by partial or complete obstruction of the neck vessels and/or airways. 23,109,110 Direct pressure on the trachea or dorsal displacement of the base of the tongue against the palate in hanging may occlude the trachea, 129 but death can occur without tracheal occlusion in people 111 and dogs. 104 A consistent agonal sequence in people is documented by filmed suicidal, homicidal, or autoerotic hangings: audible and visual respiratory movements continued following rapid loss of consciousness within 8 to 18 seconds, generalized convulsions (10–19 seconds), and loss of muscle tone in 52 to 135 seconds, with the last muscle movements occurring between 1 minute 2 seconds and 7 minutes 31 seconds. 109,110 In these case series, 109,110 marked differences were not noted between complete suspensions (with limbs suspended) and incomplete suspensions, where the body was partially supported. 35
Much of the information on the biological responses to strangulation in the medical literature, however, is derived from experiments in dogs, cats, and rodents. The objective and design of the experiments vary from investigating the blood supply to the brain or developing techniques to produce cerebral ischemia, often followed by attempts at resuscitation, to those examining the effects of vascular occlusion with or without tracheal occlusion sometimes to mimic the effects of hanging or ligature strangulation. ‡ Meaningful comparison of these results as it relates to asphyxia is difficult due to the inconsistent design and documentation of the temporal sequence and methodological determination of the respiratory, cardiac, and neurological responses. In addition, with few exceptions 1,40,45,126 animals were anesthetized during the studies. Because general anesthesia also affects the physiological responses and abrogates the behavioral responses of animals during asphyxia, 1,27 extrapolating the findings from most experimental studies to clinical cases of suspected strangulation should be done with caution. 1,17,27 A nonanesthetized animal subjected to strangulation by any method will struggle, 83,126 in part due to the severe physiological “air hunger” 11,75 that occurs before loss of consciousness. A dog suspended by its chain as a punitive method of training struggled for approximately 1 minute before it lost consciousness, 55 and in 1 experiment, unanesthetized dogs continued to “struggle violently” for 7 to 14 minutes following tracheal occlusion. 126 Videos of accidental or intentional strangulation of dogs on the Internet also confirm that animals do not lose consciousness as rapidly as reported in people. 109,110 Ligatures of thick rope, wire, or chain that were tightened by 2 “strong” men, toggles or levers, respectively in anesthetized dogs did not result in complete tracheal occlusion. 17 Only after the larynx was also manually compressed was asphyxia produced, resulting in an isoelectric electroencephalogram (EEG) at 40 seconds to 2 minutes, apnea at 4 minutes, and cardiac arrest at 9 to 10 minutes. 17
Many of the experiments in dogs, cats, rabbits, and rats simulating ligature and manual strangulation and hanging 12,50,55,56,62,66 –68 are reviewed by Boghossian. 13 Based on these papers, the general sequence of physiological responses is respiratory distress and tachycardia, followed by bradycardia, then apnea, an isoelectric (EEG), terminal or agonal respirations, and cardiac arrest. 13,49,57,63,68,122 Convulsions were described by some authors, 49,57,68,122,135 but it is not clear in other studies if convulsions were absent or occurred but were not recorded.
If only the trachea was occluded, the EEG became isoelectric between 3 minutes 45 seconds and 8 minutes, 62,70,132 and cardiac arrest occurred in dogs usually within 4 to 6 minutes 28,123,126,132 but did not develop until 1017 to 14 minutes 126 in some studies. Occlusion of the trachea with ligation or compression of the common carotid arteries, vertebral arteries, and jugular veins (with or without ligation of the vagus nerve) is thought to recapitulate the obstruction of significant anatomic structures in hanging. 13,63 Immediate dyspnea lasting 1 to 1.5 minutes, 63,123 followed by apnea for 30 seconds to 2 minutes 123 and then terminal respiratory movements for 2 to 3 minutes, 63,123 was observed. The EEG was isoelectric at 1.5 to 2 minutes, roughly half of the time than with simple obstructive asphyxia, 63,123 and cardiac arrest occurred between 4 and 6 minutes. 63 To differentiate ligature strangulation from hanging, a similar model was used but with patent vertebral arteries. 123 The respiratory and cardiovascular responses for the simulated strangulation were almost the same as those for simple obstructive asphyxia caused by tracheal obstruction. 123 Compression or ligation of the common carotid and vertebral arteries with a patent trachea in dogs or cats 49,68,99,135 caused immediate dyspnea 49 followed by apnea within 15 seconds 68 to 8 minutes. 49,57 Six of 9 dogs survived ligation of all the major vascular supply to the brain and returned to normal function in 7 to 21 days. 135 In other experiments, cerebral ischemia of 8 minutes or more resulted in permanent brain damage in dogs, but ischemia of 6 minutes or less resulted in functional recovery, often after a 5- to 40-day period of neurological dysfunction. 68
Lesions of Strangulation
There is no consensus on the number and types of lesions required to diagnose strangulation in people, 97 in part due to the biological and physical differences in response to injury; types and placement of the ligatures if used; the duration of strangulation while alive; the postmortem interval; the crime scene information; the postmortem protocols used, including those of detailed neck dissection; and standards of individual pathologists. The interpretation of the lesions depends on a balance of probabilities and exclusion of other causes of death. 19,20,78,96,100
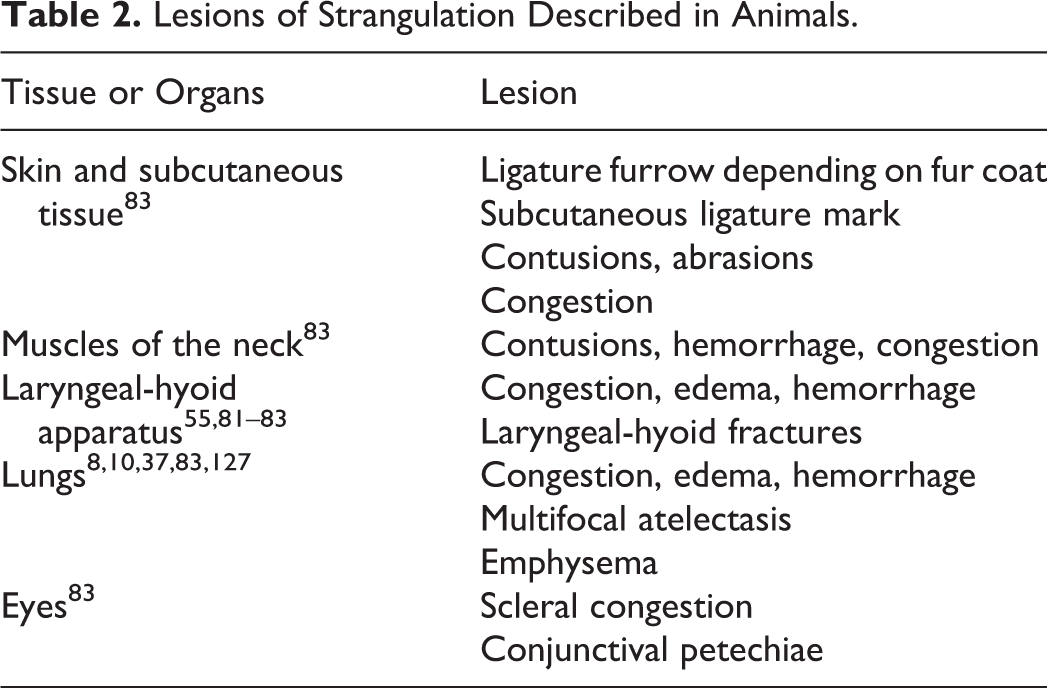
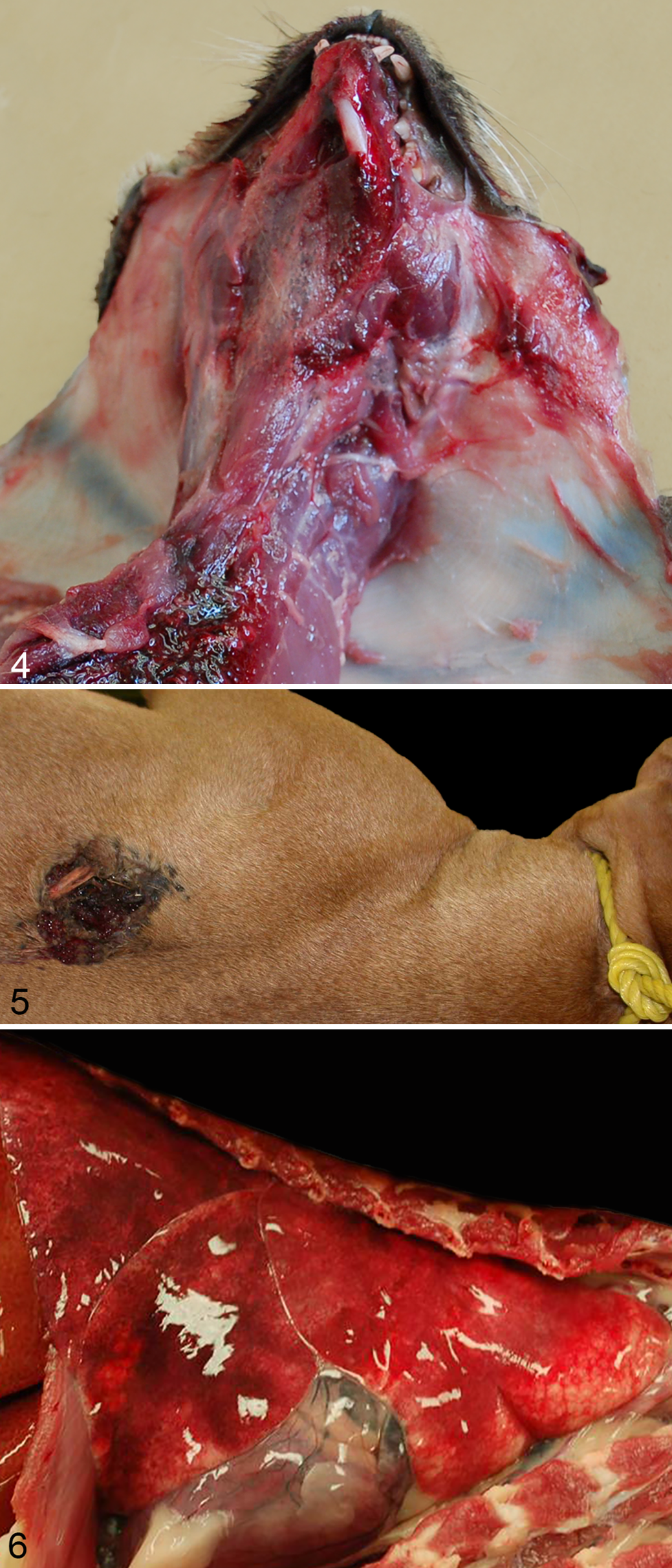
There are few reports of lesions of strangulation in the veterinary pathology literature (Table 2). 24,55,77,83 The ligature mark is the most relevant lesion in hanging and ligature strangulation, 4,38,121 although it may be absent depending on the type of ligature used, the duration, and the characteristics of the animals’ fur. 83 The ligature should be described and photographed in situ (Figs. 1, 2) and swabs for DNA from the ligature, claws, and oral cavity should be taken prior to removal of the ligature. Slipping the ligature over the animal’s head is preferable; however, if it must be cut, the knot should be kept intact, and it is recommended that the cut edges are secured with string. 119 The ligature should be placed in a paper evidence bag and sealed appropriately. Many types of material, including collars, leashes, ropes, chains, cords, clothing, towels, fabric, and wire, are used as ligatures. The animal’s coat often protects the skin from abrasions and may interfere with identification of a ligature mark. 77,83 Characteristics of the ligature furrow should be noted as to whether it is single, complete, or incomplete and the location on the neck. The pathologist’s description may differ from photographs and documentation from the death scene as the ligature may move during transport of the body. If possible, the skin should be shaved as the indentation made by the ligature may be more apparent (Fig. 3). Patterns should be noted and are often dependent on the ligature material such as links in a chain or rope twists. A ligature mark is most likely to be produced with ligatures that are narrow and hard especially if the animal was suspended for a prolonged period of time. 130 It is often easier to identify the ligature placement following reflection of the skin as a dark line of compression may be seen (Fig. 4). Frequently animals with ligatures or those that have been manually strangled also have localized abrasions and contusions, other lesions of blunt force trauma, sharp force trauma, sexual abuse, and/or projectile wounds (Fig. 5). Struggling in animals may also cause self-inflicted trauma, including abrasions, contusions, and possibly lacerations. 83 The intermittent pressure and release on the neck that tends to occur with manual strangulation 14 increases the likelihood of petechiae because the arterial blood supply to the brain is more difficult to occlude than the venous supply. 108
Lesions of Strangulation Described in Animals.

If a ligature mark, contusions, or petechiae are present, it should be noted how they relate to the major neck vessels, trachea, and laryngeal-hyoid apparatus. The jugular veins and common carotid arteries should be examined in situ and if possible the intima examined for lacerations. 129 The common carotid artery bifurcates into the internal and external carotid arteries at the same transverse plane as the hyoid bone in dogs. 41 Examination of the internal structures of the neck should include palpation of the larynx and hyoid apparatus, which may detect fractures. The stylohyoid, thyrohyoid, and epihyoid bones ossify in utero in dogs, and the basihyoid and ceratohyoid bones ossify 1 and 2 months respectively following birth. 41 Mineralization of the thyroid and cricoid cartilages in dogs is reported as early as 6 to 12 months of age, although there is considerable individual variation. 26 In people, the frequency of reported fractures of the laryngeal-hyoid apparatus varies for all types of strangulation 97,115,121,130 and usually increases with age of the person due to ossification of the hyoid and thyroid bones. 115
Detailed descriptions of neck dissections are available in the medical forensic literature. 98,101,115,119 Removal and fixation of the larynx and trachea enable additional examination following serial sectioning. 98 Microscopic hemorrhage and fractures may be present in the laryngeal-hyoid apparatus even if no macroscopic lesions are evident. 98 Documentation and identification of injuries such as fractures of the hyoid bone or displacement of the tongue or pharynx will be aided by high-quality diagnostic imaging. 39
While specific lesions may be characteristic of strangulation, none are pathognomonic (Table 2). Pulmonary edema, congestion, hemorrhage, and/or atelectasis may occur, and the dependent lobes are usually the most severely congested with hanging. 83 Munro and Munro 83 also describe congestion of the uterine cervix in female dogs, likely due to postmortem hypostasis. As the survival period may be relatively short, the absence of inflammation or hemorrhagic foci or in the lungs should also be noted. 83
Suffocation
Death due to choking, smothering, inadequate environmental oxygen, and chemical asphyxiants is collectively classified as suffocation. 111 Obstructive asphyxia caused by accidental inhalation of foreign bodies such as food or toys that lodge in the trachea or larynx is occasionally found at postmortem. Gagging is a term used in people when material is fixed over the face to prevent breathing (such as duct tape) or inserted into the mouth. 108 Animals may have foreign objects inserted into their mouth or may have their muzzle taped shut. Insertion of occlusive foreign objects into the nasal cavity of obligate nasal breathers such as horses 59 will likely suffocate the animal. Objects in the oral cavity may displace the tongue so it obstructs the airway and absorbent materials may become saturated with saliva or vomitus and become impermeable to air. These not only affect the ability to breathe but also decrease heat dissipation in animals that cannot sweat. 118 The general sequence of events in obstructive asphyxia is immediate dyspnea with convulsions, followed by bradycardia and apnea, an isoelectric EEG, agonal respirations, and cardiac arrest usually within 4 to 6 minutes. 123 In 1 experiment, all dogs with cardiac arrest could be successfully resuscitated after 5 minutes of obstructive asphyxia, some between 5 and 10 minutes, and none after 10 minutes. 28
Nonobstructive Suffocation
In contrast to obstructive asphyxia, cardiac arrest in dogs takes at least twice as long and up to 30 minutes with nonobstructive asphyxia by plastic bag suffocation 123 or in experiments where the inspired oxygen concentration is 2.43%. 125,126 This is different from humans, who die in less than a minute if the oxygen concentration is 2% to 3%. 86 Depending on the experimental design, cardiac arrest occurs before, after, or concurrent to respiratory arrest. 125,126
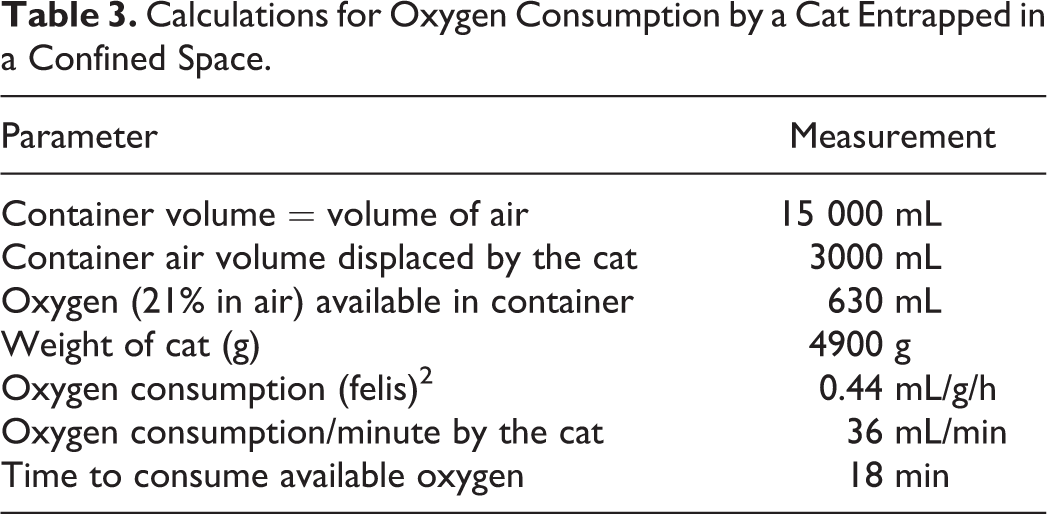
Death due to entrapment in small, enclosed spaces that are airtight or nearly airtight is likely due to oxygen deprivation, but hyperthermia and heat stroke also need to be considered. 3,31,53 A cat confirmed to have died in a confined space was received for postmortem at the Animal Health Laboratory, University of Guelph. The stray cat had been transported in a 15-liter plastic airtight container by the person who found it to a shelter about an hour’s drive away. Upon arrival at the shelter, the cat was dead and not in rigor mortis. Based on data for oxygen consumption in the domestic cat, 2 it was determined that the available oxygen in the container would be consumed within 18 minutes (Table 3). These calculations illustrate the amount of available oxygen in the container but do not consider the probable increased physical exertion, volume of exhaled CO2, and elevated local environmental and body temperature, all of which would have likely decreased the survival time. 3,31,53
Calculations for Oxygen Consumption by a Cat Entrapped in a Confined Space.
Asphyxiants
CO2 is both an exogenous asphyxiant and an endogenous product of tissue metabolism. Mechanisms of CO2 toxicity are reviewed by Guais et al. 56 Elevated atmospheric CO2 is encountered in industrial settings, from use of dry ice, and with combustion, fermentation, or putrefaction. 56 Probably most animals exposed to toxic levels of atmospheric CO2 are those intentionally euthanized by this method, although fatal hypercarbia in dogs and cats is reported due to malfunction of an anesthetic machine. 21 Strongly aversive responses occur in animals exposed to even very high concentrations of CO2 until unconsciousness is reached. 72 Above 80% CO2 inhalation results in an isoelectric EEG within 30 seconds and respiratory arrest within 1 minute in anesthetized dogs, but it takes 7 to 8 minutes to develop cardiac arrest with 80% CO2 compared to 1 minute with 100% CO2. 64
Carbon monoxide (CO) and hydrogen cyanide (HCN) are 2 of the primary chemical asphyxiants. 78 Car exhaust and inefficient gas heaters produce high levels of carbon monoxide due to incomplete combustion of hydrocarbons. 19,102 Combinations of reduced oxygen and elevated CO2, CO, and HCN 78 often occurs in house fires, and animals may be both victims and evidence in crimes against people where a fire is set to destroy evidence. 76 Histological evidence of smoke inhalation, burns with a vital reaction, and laryngeal edema will aid in determining if the animal was alive prior to the fire. Carbon monoxide has 200 to 300 times greater affinity for hemoglobin than oxygen, producing carboxyhemoglobin, which liberates CO very slowly. 83,133 Additional mechanisms and physiological responses of animals and people to CO are reviewed extensively. 92,102,106,133 Briefly, the toxic effects of CO extend beyond simple hypoxia and include the binding of CO to other heme proteins impairing mitochondrial function, as well as proinflammatory effects leading to neutrophil degranulation, platelet-neutrophil aggregation, and production of reactive oxygen species. 102,106,133 If the animal survives a period of time, lesions produced are a result of hypoxia and direct toxicity affecting primarily the brain 69,92,137 and heart. 87,89 Carboxyhemoglobin is stable in tissues, and the cherry red color of soft tissues is usually maintained in the body; however, this should not be confused with postmortem artifact seen in some animals that have been frozen. 83 Carboxyhemoglobin is also remarkably stable in stored blood samples for weeks or even months. 48,58
HCN interferes with cellular respiration by combining with the ferric iron atom of cytochrome c oxidase, 78 preventing mitochondrial respiration and tissue utilization of oxyhemoglobin. 33 Inhalation results in death within 6 to 8 minutes, 35 and pathologists should note that it could be absorbed percutaneously and inhaled from remnants in the stomach. 108 Even though it is caustic to the esophagus and stomach, HCN can be ingested as potassium or sodium salts forming hydrocyanic acid once the substance contacts gastric acids or water. 108 The bitter almond odor produced by cyanide cannot be detected by everyone, and its absence should not rule out HCN toxicity. 33,35 HCN is unstable and may not be detectable if sufficient time elapses between death and toxicological analysis. 33 The evanescent characteristic bright red color of the blood and tissues is due to oxyhemoglobin. 96
Hydrogen sulfide (H2 S) is a component of “sewer gas,” produced by fermentation of organic matter, 33 and even a small concentration of 1000 to 2000 ppm (0.1%–0.2%) in air can be rapidly fatal. H2 S also inhibits mitochondrial respiration and reduces oxyhemoglobin to methemoglobin, resulting in cyanosis and darkly colored blood. 33
Lesions of Suffocation
Obstructive asphyxia due to a foreign body lodged in the trachea or larynx is usually a straightforward diagnosis. The diagnosis may be problematic if a foreign body was removed prior to postmortem examination, although there may be intraluminal trace evidence of the object, focal edema, congestion, hemorrhage, erosion, or ulceration at the obstructed site.
Evidence such as adhesive from duct tape around the muzzle or mouth or plastic bags may provide clues to the methods used. An animal may traumatize itself during struggling and may have abrasions, contusions, or lacerations such as a torn frenulum inflicted by the individual attempting to subdue it (Table 4). If an animal is entrapped in a container, claws may be frayed in attempts to escape. Sand or dirt in the nasal cavity or trachea of an exhumed animal indicates respiratory inhalation, but if the material is only in the mouth, then passive transfer into the orifice must be considered. 83
Lesions of Suffocation Described in Animals.
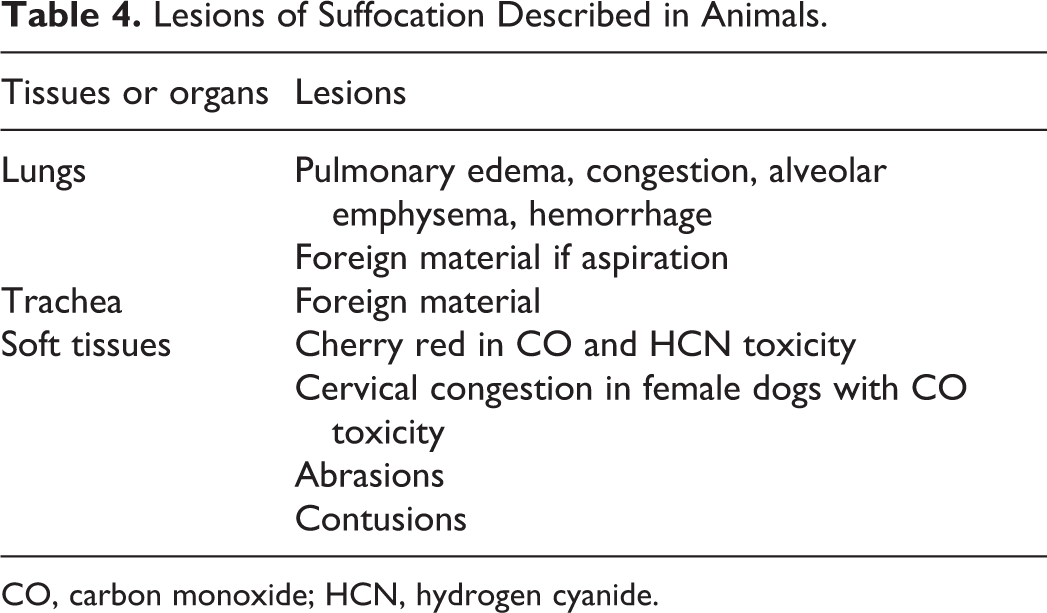
CO, carbon monoxide; HCN, hydrogen cyanide.
There are often no macroscopic lesions in nonobstructive suffocation, 33,108,117 particularly if the individual rapidly becomes unconscious in a space where oxygen is markedly reduced, depleted, or replaced by carbon dioxide. 33,108 Partial, total, or intermittent airway obstruction causes noncardiogenic pulmonary edema in dogs. 8,44,65 The lungs may have nonspecific lesions of edema, multifocal emphysema, and patchy congestion (Table 4, Fig. 6).
Animals exposed to toxic levels of CO or HCN will have a cherry red tissue color that is stable with CO toxicity but unstable with HCN, and either may be masked by postmortem changes. 83 Specific histologic lesions associated with CO toxicity in dogs and cats are neuronal necrosis of the palladium, substania nigra, and cerebellum. 69,89 In experimental models of CO toxicity, pericardial effusion, myelin damage, cerebral vascular congestion, and perivascular hemorrhage occur in dogs. 137 Demyelination of the deep white matter occurs in people and cats. 88,106 The distribution of brain lesions in CO toxicity is thought to be related to the blood supply, hypotension, hypoxia, and direct cytotoxicity. 87 –89 Coagulation necrosis of cardiac myofibers with CO toxicity is also reported in cats 89 and people. 133
Mechanical Asphyxia
Respiration restricted by external pressure on the chest and/or abdomen or by an acquired posture are types of mechanical asphyxia. Positional asphyxia will occur in an animal hanging from the hind feet in an inverted position, which results in pressure on the respiratory tract from the abdominal organs and reduces cerebral circulation. 131 In people, death is thought to be due to hypoxia and cardiac failure due to cardiac overload. 12,113 Animals trapped in a posture impeding respiration by producing pressure on the thorax or narrowing of the airways will die if they are unable to extricate themselves due to the awkward position, traumatic injury, or prior incapacitation. In these instances, the history, information from the scene, and the pattern of lividity if the animal is not removed immediately may aid in identifying positional asphyxia as the cause of death. However, lesions if present may not be informative. 12 The congestion and petechiation that occur in these cases may be difficult to distinguish from postmortem hypostasis. Reflection of the skin may identify contusions and hemorrhages created by a ligature or manual restraint around the hind limbs.
Crush injuries of the thorax and abdomen also result in asphyxia by preventing respiratory movements and inhibiting venous return to the heart. 12,33,113 These can occur by animals being crowded and trampled 83 or intentionally in sadomasochistic videos where animals are intentionally crushed. 93
Lesions of Mechanical Asphyxia
As in other types of asphyxia, the lesions of positional asphyxia may not be sensitive or specific, and knowing the animal’s position at death may be helpful in determining if some lesions were due to postmortem hypostasis. Petechiae and congestion are directly proportional to the degree of venous obstruction and may be absent if there is arterial occlusion anterior to the heart. 12 Hemorrhage of the respiratory muscles and muscles of the back and neck is described in people and attributed to strained muscular movements and convulsions. 12 Discoloration of the face, neck, and upper body due to mechanical asphyxia in people is occasionally referred to as masque ecchymotique, 113 another term that should be avoided in veterinary forensic pathology due to the difficulty in documenting this in animals because of their hair coat. Venous obstruction results in edema of the dependent tissues. Other lesions described in people are retinal and tympanic hemorrhages, pulmonary congestion and edema, cerebral edema, and petechiae. 113 Fractures, lacerations, and internal hemorrhage due to trauma are likely to be present if the animal was crushed.
Summary
Animals and people are similar in that death due to the various mechanisms of asphyxia may or may not produce lesions and, if present, the lesions are neither sensitive nor specific indicators of asphyxiation. Nonetheless, the presence and absence of lesions should be documented in all forensic postmortems: this is the evidence. The interpretation or opinion that the death was due to asphyxia requires definitive and compelling evidence from the postmortem examination, history, and/or death scene. 19,20,78,96,108,128 Unlike medical examiners, veterinary pathologists rarely attend a death scene. Veterinary pathologists are often not provided the entire information from the scene investigators 90 and therefore may lack some of the crucial information required to confirm death due to an asphyxial mechanism. In cases of strangulation, there may be evidence of a ligature, contusions, abrasions, hemorrhage, and/or fracture of the laryngeal-hyoid apparatus. Investigators should provide the pathologist with information obtained at the recovery or death scene, such as the position of the animal, to aid in distinguishing petechiae due to neck compression by ligature or manual strangulation, positional asphyxia, or lividity.
Beyond the postmortem examination, pathologists may be faced with questions of forensic importance involving the behavioral and physiological responses in animals subjected to strangulation, suffocation, or traumatic asphyxia to determine if the animal suffered. Aversive behavior to noxious or painful stimuli is addressed in the increasing literature on animal welfare, 11,30,73,75 and several reviews have specifically tackled the welfare implications of breathlessness in animals. 11,75 How long does it take to become unconscious and develop respiratory and cardiac arrest, and when does irreversible cerebral ischemia occur? People become unconscious during hanging within 8 to 18 seconds and develop irreversible brain damage within 4 to 6 minutes. 14,109 While there is no prescriptive answer to these questions in animals, the peer-reviewed literature indicates that for some mechanisms of asphyxia, 13,18,55,125 consciousness is maintained for longer periods, and the onset of death is often delayed compare to that in people. Experimental data offer some insight into the pathophysiology of various mechanisms of asphyxia in animals but do not provide the veterinary pathologist with sufficient or easily applicable information when confronted with these cases. The paucity of peer-reviewed literature in veterinary forensic pathology will hopefully be remedied in the future by the publication of case series, case reports, and registries describing macroscopic and microscopic lesions in cases of confirmed asphyxial deaths.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.