
Abstract
Pectinate ligament dysplasia (PLD) is a common cause of canine glaucoma and the definitive clinical diagnosis is based on gonioscopy. Although the histologic lesions of PLD have been described, it has not been determined whether these changes are specific for PLD or if similar histologic changes can develop as a consequence of secondary glaucoma. The filtration angles of 61 enucleated canine globes with chronic glaucoma were evaluated with light microscopy by 3 examiners who were masked to the clinical history, signalment, and gonioscopic results. A histologic diagnosis of PLD versus non-PLD was determined by each examiner based on previously reported morphologic criteria and compared with the clinical gonioscopic diagnosis. Of the 61 enucleated glaucomatous eyes, 40 were clinically diagnosed with PLD. For all 3 examiners, a histologic diagnosis of PLD corresponded poorly with the clinical diagnosis of PLD (range of kappa score: 0.149-0.269; range of AUC: 0.592-0.621). There was no difference between examiners in their ability to correctly diagnose PLD histologically (P = .978). A fair degree of agreement was noted among examiners in obtaining their suspected histologic diagnosis of PLD (kappa score 0.256). No individual or sets of histologic ICA features were consistent with clinical PLD. The results indicate the histologic ICA changes proposed to be characteristic of PLD are also noted in canine globes affected with chronic secondary glaucoma. Therefore, using routine histologic evaluation, a histologic diagnosis of PLD is not possible in the face of chronic canine glaucoma.
Keywords
Glaucoma is a common condition in dogs typically characterized by an elevated intraocular pressure (IOP). Primary glaucoma is defined as an elevated IOP without other antecedent intraocular disease. In contrast, secondary glaucoma occurs as a direct result of antecedent ocular disease or its sequela. 1 The most common type of primary glaucoma in dogs is associated with pectinate ligament dysplasia (PLD). 10,20 PLD, also commonly known as goniodysgenesis, is a bilateral condition in which there is a lack of fenestration of the iridocorneal angle (ICA) during development of the eye. PLD-associated glaucoma has been reported in many dog breeds including the American Cocker Spaniel, 2 English Cocker Spaniel, 2 Basset Hound, 2 Bouvier des Flandres, 26 Welsh Springer Spaniel, 6 Chow Chow, 5 Samoyed, 9 and Norwegian Elkhound. 8 The exact pathogenesis of PLD-associated glaucoma is unknown. Although PLD is congenital and inherited, not all dogs with PLD develop glaucoma 6,9,28 and in those that do, glaucoma typically does not develop until middle age (ie, 4-8 years of age) or older. 1 Typically, affected dogs initially present with unilateral disease, with the contralateral eye becoming glaucomatous in the ensuing days to years. 12,16
Gonioscopy is the clinical examination of the ICA and opening of the ciliary cleft (CC) (also known as the filtration angle). This technique uses a corneal contact lens and a source of illumination (most commonly a slit-lamp biomicroscope) to evaluate the aqueous outflow pathways in a conscious patient following topical anesthesia. 3 Gonioscopy has long been advocated for studying canine glaucoma and it is a useful clinical procedure that facilitates the diagnosis, categorization and management of canine primary and secondary glaucoma. 1,12 –14 Using gonioscopy, the ICA can be subjectively described as open, narrow, or closed. The ICA angle is considered closed when there is anterior displacement of the base of the iris to overlie the pectinate ligament (PL) and the peripheral cornea. This occurs most commonly with peripheral anterior synechiae and with iridal neoplasms. 10
Clinically, PLD can be readily diagnosed by gonioscopy. 3 In PLD the ICA is open but there is failure in development of the PL such that it appears as a solid sheet of uveal tissue spanning the ICA. 10 Using both gonioscopic and light microscopic observation, Martin and Wyman 15 were the first to describe dysplastic PLs in Bassett Hounds. A histologically observed dysgenesis was described in 1 dog where the base of iris was pulled forward by a “thick band of tissue which merged into the posterior peripheral corneal surface.” 15 Further gonioscopic and histologic studies 1 examined various breeds including the English Cocker Spaniel and Bassett Hound noting narrowing of the ICA by gonioscopy. Histologically these cases were noted to have loss of the trabecular meshwork arrangement and ICA alterations described as “extensive peripheral anterior synechia.” 1 In some cases Descemet’s membrane was thickened and divided the iris root from the compacted trabecular meshwork tissue. 1 Since these early studies, many histopathological studies have described the filtration angle of dogs affected with PLD. 2,4,15,17,18,22,25 –27 A retrospective histologic study 25 described morphological patterns of aqueous outflow pathway alterations that were suggestive of PLD. These alterations were similar to some of the features of PLD described in other studies and resources 2,4,5,7,11,15,17,18,22,23,25 –27 and included an open ICA but closed CC, the absence of a clearly defined PL, solid uveal tissue spanning from iris root to termination of Descemet’s membrane (DM), thickening of trabecular meshwork (TM) beams, alterations in the termination of DM, extension of pigmented spindle cells into the deep corneal stroma adjacent to DM and extension of uveal tissue onto the posterior surface of peripheral DM.
After years of regularly evaluating glaucomatous canine globes clinically and histologically, the authors noted that histologic alterations in the filtration angle of glaucomatous globes clinically unaffected by PLD often appeared similar to the aforementioned alterations reported to be consistent with PLD. Furthermore, when reviewing the literature, there is a lack of correlation between the clinical (gonioscopic) and histological alterations of the ICA in canine globes. This masked, controlled study was designed to histologically investigate the filtration angles of glaucomatous canine globes clinically confirmed with and without PLD and to correlate the morphologic findings with the gonioscopic data. We hypothesized that the histologic diagnosis of PLD may not correlate with the gonioscopic diagnosis of PLD and that PLD cannot be diagnosed solely by routine histological examination in canine globes affected with chronic glaucoma.
Materials and Methods
Data Collection
Medical records at the Western College of Veterinary Medicine were searched over a 10-year period for canine patients with a clinical diagnosis of glaucoma, resulting in enucleation and submission of the globe for light microscopic evaluation. Inclusion criteria were a complete ophthalmic examination of the patient, including gonioscopy of both eyes by a board certified veterinary ophthalmologist and enucleation with availability of a histologic section of the affected glaucomatous globe. Gonioscopy was always performed on the unaffected eye and included the affected eye when edema or secondary changes did not preclude visualization of the ICA. All gonioscopy was completed following topical anesthesia and using a Koeppe lens with placement of methylcellulose gel on the cornea. The filtration angle was viewed with the aid of a slit-lamp biomicroscope and the entire ICA and opening of the CC were evaluated systematically. Normal filtration angles were identified by the presence of normal PLs circumferentially, originating from the iris base, traversing the CC and inserting onto the corneal endothelium. Standard variation in PL thickness between breeds and individual animals was taken into account. 3 Based on previous investigations, 4,9,21 PL were considered normal if less than 10% of “normally focally dysplastic” PLs were present within the angle circumference. Similarly, a clinical diagnosis of PLD was based on the absence of normal PLs and the presence of solid sheets of uveal tissue spanning 90-100% of the circumference of the ICA with or without the presence of flow-holes in both the affected and unaffected eye, or solely in the unaffected eye. Peripheral anterior synechia (also known as a closed ICA) were differentiated from PLD based on a shallow anterior chamber and the attachment of iris to the corneal endothelial surface. Clinical information including history, signalment, and gonioscopic data was recorded for all cases.
The formalin-fixed, vertically sectioned, paraffin-embedded enucleated eyes were retrieved from archived collections. For each case a minimum of one 4 μm sagittal section through the pupil and optic nerve was stained with hematoxylin-eosin (H&E) and periodic acid-Schiff (PAS) reaction. The slides were separately examined with light microscopy by 3 examiners: 1 board-certified veterinary pathologist (HP) and 2 board-certified veterinary ophthalmologists with experience in histopathology (BG, LS). Examiners were unaware of the history, signalment and gonioscopic findings and examiners evaluated the entire globe with focus on the filtration angle. The filtration angle alterations suggestive of PLD by Smith et al 25 (Table 1) were evaluated in each globe and were used by examiners to histologically diagnose whether the ICA was affected or unaffected with PLD. As alterations in the posterior iris epithelium have been reported in PLD-associated glaucoma 22 examiners also evaluated the posterior iris epithelium. Data obtained was then statistically evaluated. Each examiner’s final histological diagnosis of PLD or not was then compared with the clinical diagnosis. Agreement between examiners was analyzed, as well as whether any specific histologic ICA features or group of features were consistent with a clinical diagnosis of PLD.
Agreement (Kappa Coefficients) Among Examiners for Evaluating Histologic Features in Glaucomatous Canine Eyes.
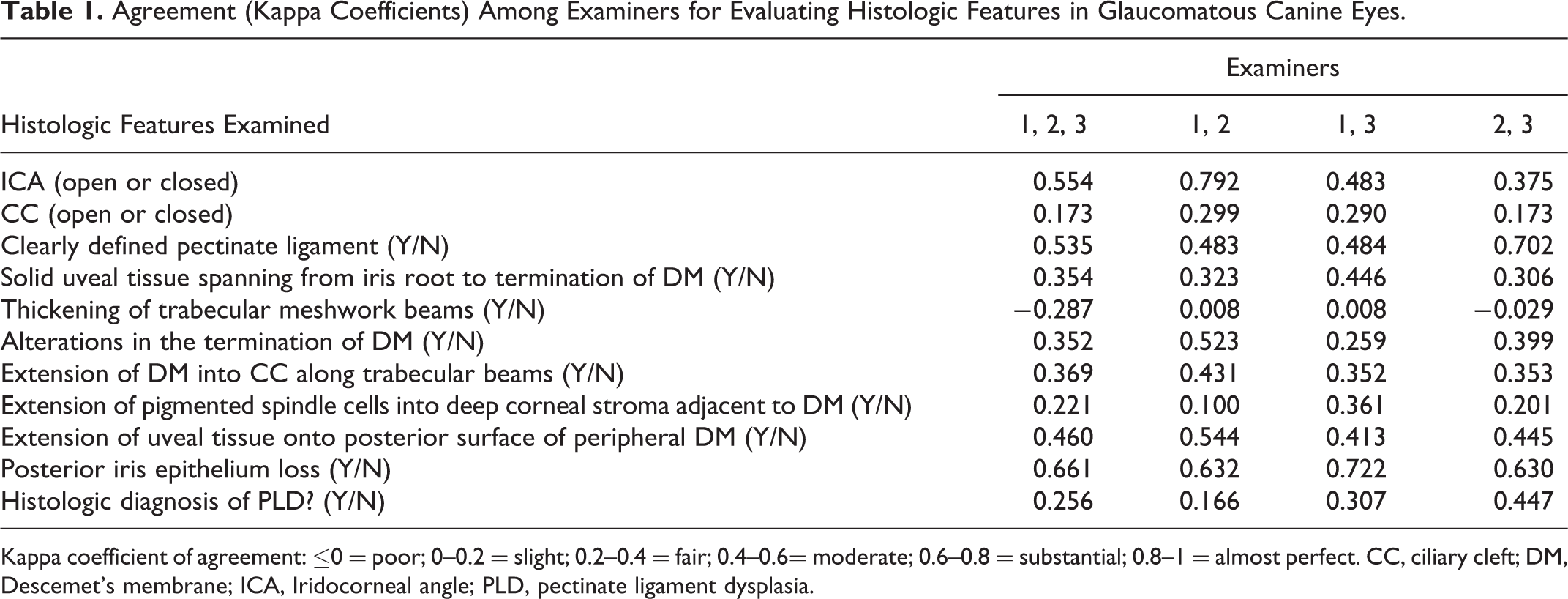
Kappa coefficient of agreement: ≤0 = poor; 0–0.2 = slight; 0.2–0.4 = fair; 0.4–0.6= moderate; 0.6–0.8 = substantial; 0.8–1 = almost perfect. CC, ciliary cleft; DM, Descemet’s membrane; ICA, Iridocorneal angle; PLD, pectinate ligament dysplasia.
As per Smith et al, 25 the ICA was defined as the angle created by the termination of DM, the primary PL spanning the base of the angle and the anterior surface of the iris root. The CC was defined as the area bordered by the uveoscleral TM externally, the ciliary body stroma internally and posteriorly and the primary PL anteriorly (Fig. 1). A closed ICA was defined as the anterior iris face being in direct apposition to the corneal endothelium and DM (ie, anterior synechia). Extension of DM into CC along the TM beams was defined as continuous or noncontinuous thickening of terminal DM with finger-like extensions into the CC along the uveoscleral and uveal TM (descemetization of TM) (Fig. 2). PAS reaction was used to highlight DM to allow for more accurate evaluation of the termination of DM.
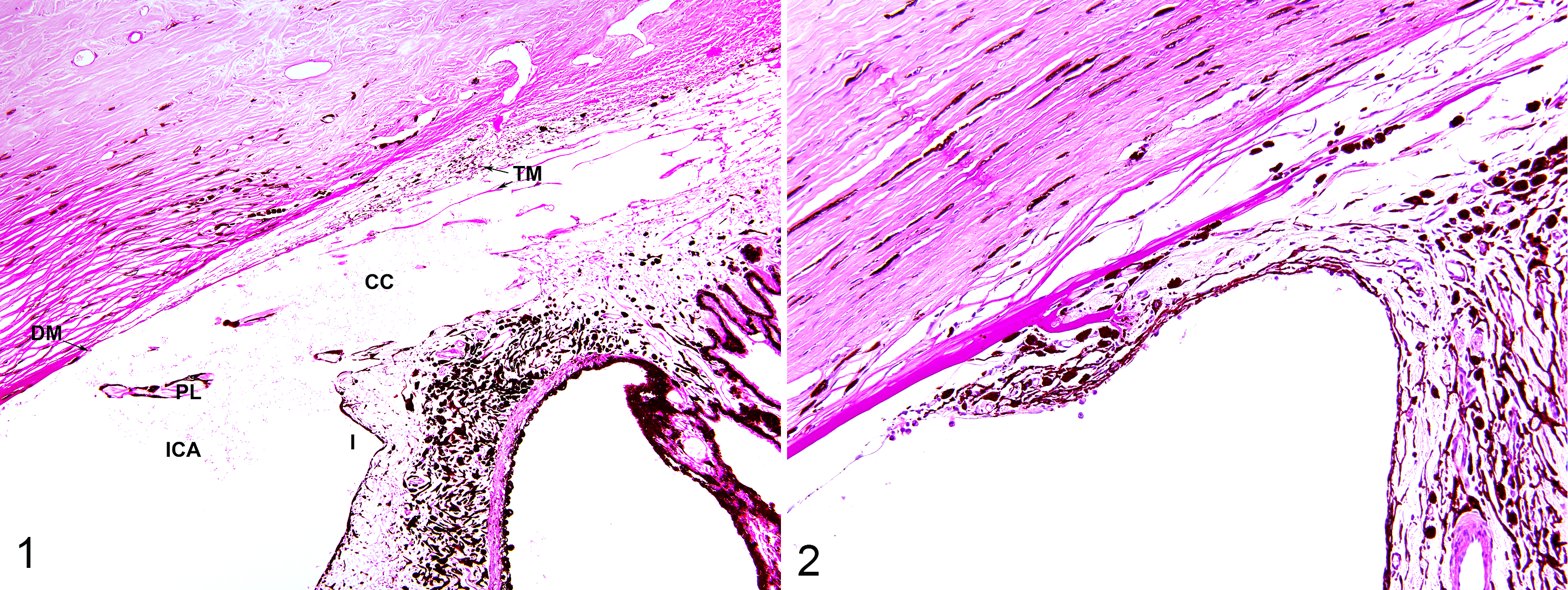
Filtration angle, eye, dog.
Statistical Analysis
The overall discriminatory ability of each of the histologic features and the final histologic diagnosis for each examiner were evaluated using the kappa coefficient of agreement, which adjusts for chance agreement. The area under the receiver operating characteristic (ROC) curve (AUC) was also assessed, which was calculated based on a logistic regression model using the true clinical status (ie, PLD via gonioscopy) as the outcome and each of the histologic features as the covariate. To test if there was no difference in the discriminatory ability of the 3 examiners, Kruskal-Wallis’s test was applied to the kappa and AUC scores. To measure the degree of interexaminer agreement for each of the histologic features and their agreement for the final histologic diagnosis a kappa coefficient of agreement was used.
To examine whether there was a set of histological features most consistent with a diagnosis of PLD for each examiner, logistic regression model was used with PLD as the outcome and histological features as covariates. First, the variables were screened by examining the unconditional association between each histological feature and PLD. Variables with P <0.2 based on the type 3 Wald test were retained for consideration in building the final model. Then, backward model selection was applied such that the least significant variable is dropped sequentially until all the covariates are significant at the 0.05 level of significance. The analyses were performed using SAS software version 9.3 (SAS Institute Inc, Cary, NC, USA).
Results
Of the 61 enucleated glaucomatous eyes, 40 were diagnosed clinically with PLD. Eyes diagnosed clinically with PLD-associated glaucoma included the following breeds: Cocker Spaniel (10), Shiba Inu (5), Basset Hound (3), Chow-Chow (3), Cocker Spaniel-cross (2), Husky-cross (2), Great Pyrenees and Great Pyrenees-cross (2), Labrador Retriever-cross (2), Golden Retriever and Golden Retriever-cross (2), Siberian Husky (2), Bouvier de Flandres (1), Labrador retriever (1), Norwegian Elkhound (1), Shih Tzu (1), Chow-Chow-cross (1), Shepherd-cross (1), Terrier-cross (1). Eyes clinically diagnosed without PLD included the following breeds: Cocker Spaniel-cross (4), Shih Tzu (4), Shih Tzu-cross (3), American Cocker Spaniel (2), Labrador Retriever (2), Australian Shepherd and Australian Shepherd-cross (2), Golden Retriever (1), Gordon Setter (1), Lhasa Apso (1), Pekingese-cross (1). Primary clinical diagnoses for non-PLD-affected glaucomatous dogs included chronic uveitis (8), retinal detachment (4), lens luxation (3), chronic cataract (3), glaucoma following phacoemulsification surgery (2), and intraocular neoplasia (1).
Light microscopic examination of all globes examined by all masked examiners confirmed histopathologic evidence of glaucoma. Using the kappa coefficient of agreement and AUC scores for all 3 examiners separately, a histologic diagnosis of PLD corresponded poorly with the clinical diagnosis of PLD (range of kappa score: 0.149-0.269; range of AUC: 0.592-0.621) (Table 2). Similar histologic lesions in filtration angles from dogs with gonioscopic diagnoses of PLD-associated glaucoma and dogs with secondary glaucoma are demonstrated in Figs. 3–8. There was no difference in the discriminatory ability of the 3 examiners based on the Kruskal-Wallis’s test (P = .978). Evaluation of interexaminer agreement of all 3 examiners revealed a substantial degree of agreement in determining posterior iris epithelial loss (kappa score 0.661); and a moderate degree of agreement for assessment of an open or closed ICA (kappa score 0.554), a clearly defined PL (kappa score 0.535), and extension of uveal tissue onto the posterior surface of the peripheral DM (kappa score 0.460) (Table 1). All other features examined revealed fair to poor degrees of agreement (kappa scores –0.287 to 0.369), including a fair degree of agreement among examiners in their histologic diagnosis of PLD (kappa score 0.256) (Table 1).
Comparisons Between Histologic Diagnosis and Gonioscopic Diagnosis of Pectinate Ligament Dysplasia in Glaucomatous Canine Eyes, for 3 Different Examiners.
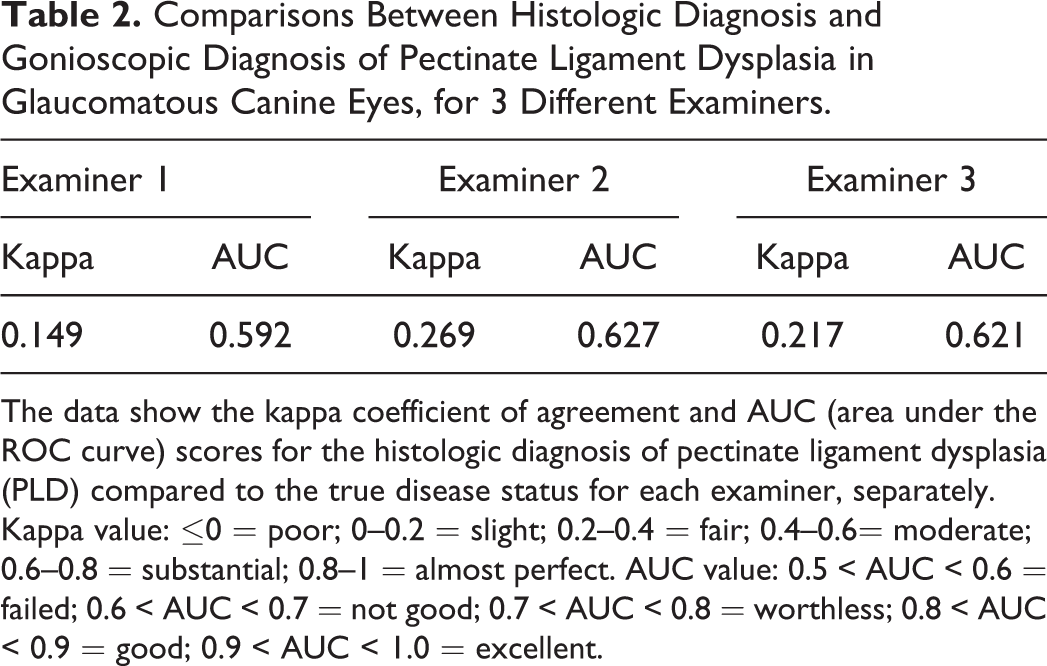
The data show the kappa coefficient of agreement and AUC (area under the ROC curve) scores for the histologic diagnosis of pectinate ligament dysplasia (PLD) compared to the true disease status for each examiner, separately. Kappa value: ≤0 = poor; 0–0.2 = slight; 0.2–0.4 = fair; 0.4–0.6= moderate; 0.6–0.8 = substantial; 0.8–1 = almost perfect. AUC value: 0.5 < AUC < 0.6 = failed; 0.6 < AUC < 0.7 = not good; 0.7 < AUC < 0.8 = worthless; 0.8 < AUC < 0.9 = good; 0.9 < AUC < 1.0 = excellent.
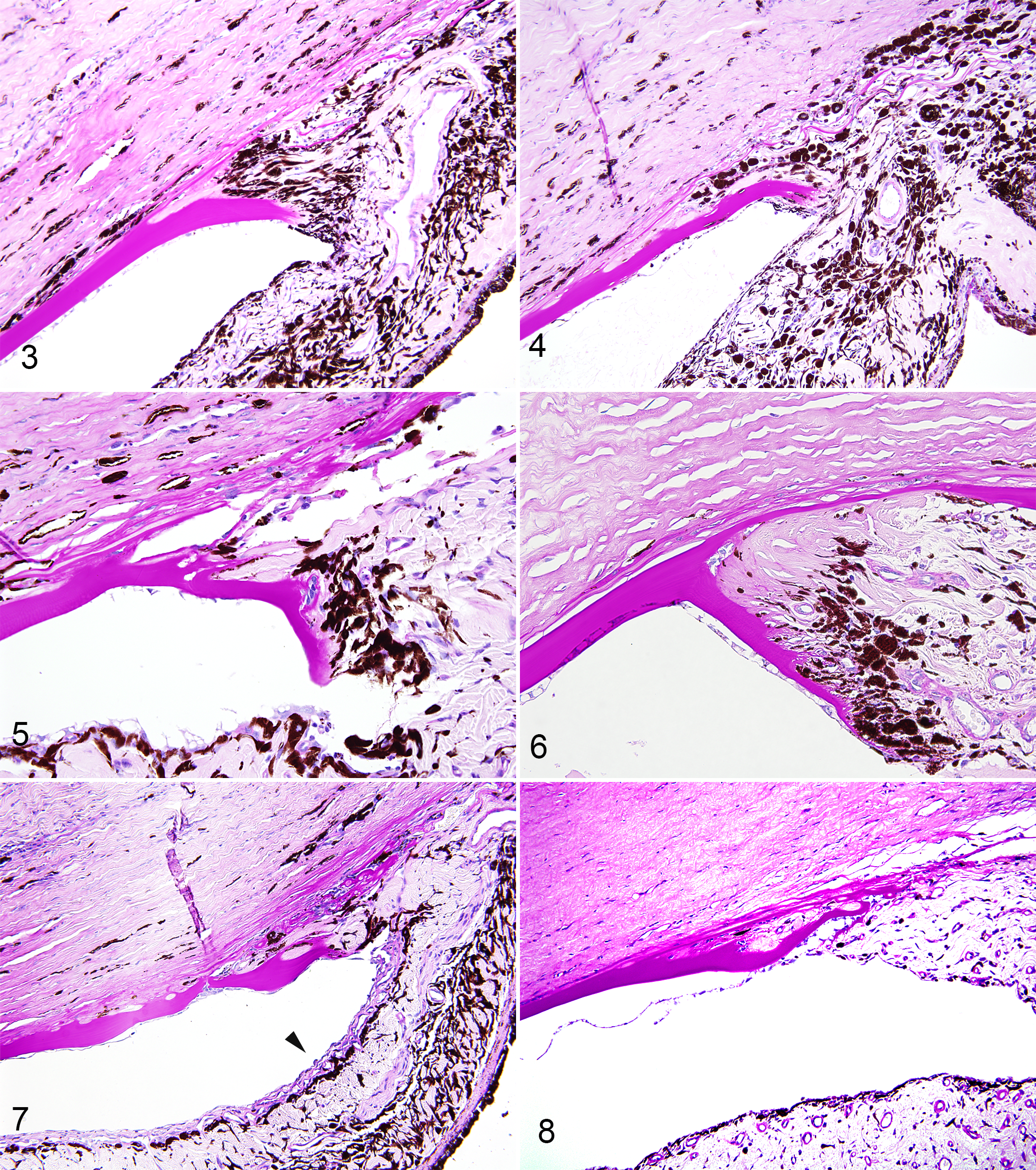
Filtration angle, eye, dog. The panel shows pairs of similar histologic lesions in filtration angles from dogs with gonioscopic diagnoses of pectinate ligament dysplasia (PLD)-associated glaucoma and dogs with secondary glaucoma. In all photos note the absence of a clearly defined pectinate ligament, solid uveal tissue spanning from iris root to the termination of Descemet’s membrane, and alterations in the termination of DM. Periodic acid-Schiff.
No individual or sets of histologic ICA features were consistent with clinical PLD; however, for 2/3 examiners, a globe with a closed CC was more likely to be diagnosed with PLD. The odds ratio and the 95% confidence interval (CI) for these examiners were 12.34 (2.21-68.88) and 9.33 (2.61, 33.39). No sets of histologic features were consistent with a histologic diagnosis of PLD for any examiner; however, for 1 examiner, globes were 14.29 times more likely to be diagnosed with suspected PLD if alterations in the termination of DM were noted (95% CI: 2.22-90.91) and 13.20 times more likely if the CC was closed (95% CI: 2.97-60.72). For another examiner, globes were 12.35 times more likely to be diagnosed with suspected PLD if descemetization of the TM was noted (95% CI: 1.33-111.11) and 8.55 more likely, if alterations in the termination of DM were noted (95% CI: 2.16-34.48). For the last examiner, no sets of histologic ICA features were identified to be consistent with a diagnosis of PLD.
Discussion
The first objective of this study was to determine whether the clinical diagnosis of PLD corresponded with the histological diagnosis of PLD in chronic glaucomatous globes by routine light microscopy using certain histological features noted 25 to be suggestive of PLD. Using the AUC scores for all 3 examiners separately, a histologic diagnosis of PLD did not correspond to the clinical diagnosis of PLD in the face of chronic canine glaucoma. The authors speculate that the secondary effects of glaucoma alter the filtration angle morphology such that the filtration angles of secondary glaucoma cases appear histologically similar to PLD (Figs. 3–8). Specifically, in many cases of glaucoma the authors suspect that ICA stretching and recession due to elevated IOP cause the PLs and TM to appear more thickened histologically. Interestingly, the unmasked morphologic study by Smith et al 25 suggested that as the CC collapses in some cases of secondary glaucoma, the PL flattens giving a similar appearance to a dysplastic PL, and that similar ICA alterations may occur in globes affected with primary and secondary glaucoma. 25 The findings from our masked study confirm these suggestions. It has been suggested that PLD can progress in individual dogs over time. 19 However, similar to ICA alterations that are proposed to occur with glaucoma, the authors believe that this congenital condition does not progress but rather that the normal age-related increases in lens size 24 result in narrowing of the ICA. This narrowing can then be misinterpreted as PLD progression.
The second objective was to determine whether there was a difference noted between examiners in their ability to diagnose PLD histologically. No difference was noted between examiners (P = .978). Although 2 of the masked examiners were board-certified veterinary ophthalmologists with experience in histopathology (BG, LS) and 1 was a board-certified veterinary pathologist (HP), all examiners have extensive and similar ocular pathology experience and as such, a difference between examiners was not expected.
In evaluating the degree of agreement between examiners the kappa coefficient of agreement revealed a substantial degree of agreement only in the evaluation of posterior iris epithelial loss. Although independent from the main objective of this study, which was to evaluate the morphology of the ICA, the posterior iris epithelium was examined to further evaluate whether pupillary block may play a role in the pathogenesis of PLD-associated glaucoma. A morphologic review of PLD-associated glaucoma cases 22 noted segmental loss of posterior iris epithelium, and theorized that pupillary block associated with iris-lens touching may be important in the pathogenesis of PLD-associated glaucoma. In our study, this feature was not a predictor of PLD-associated glaucoma when compared to secondary glaucoma and all examiners in our study were in agreement with the assessment of posterior iris epithelial loss.
A moderate degree of agreement was noted between all examiners for assessment of an open or closed ICA, a clearly defined PL and extension of uveal tissue onto the posterior surface of the peripheral DM. All other features examined revealed fair to poor degrees of agreement and a fair degree of agreement was noted among examiners in their final histologic diagnosis of PLD. These findings demonstrate that the previously reported histologic features of PLD appear to be ambiguous and they may not be interpreted the same way by different examiners making ICA assessment of chronic glaucomatous globes difficult with light microscopy.
Lastly, no individual or sets of histologic ICA features were consistent with a clinical diagnosis of PLD-associated glaucoma in our study. However, for 2 out of 3 examiners, a globe with a closed CC was more likely to have a clinical diagnosis of PLD-associated glaucoma. This is in contrast to the study by Smith et al 25 where collapse of the CC was the most consistent finding in both PLD associated and secondary glaucoma. Furthermore, no sets of histologic features were consistent with a histologic diagnosis of PLD for each examiner. However, 2 of 3 examiners were more likely to diagnose suspected PLD if alterations in the termination of DM were noted and 1 of 3 examiners was more likely to diagnose suspected PLD if the CC was closed or if descemetization of the TM was noted. The lack of ICA features consistent with PLD in our study is not unexpected. In the study by Smith et al 25 extension of DM into the CC along the TM beams (descemetization of the TM) was noted in secondary as well as primary glaucomas. Overall, Smith recognized that with secondary glaucomas, as the CC collapses, the PL flattens against the sclerocornea and uveoscleral TM, giving a similar appearance to a dysplastic PL. 25 It was, however, proposed that this ligament is not as prominent and does not have the same thickness of tissue seen in the eyes with PLD-associated glaucoma. 25 In our study a difference in PL thickness or prominence was not noted between PLD and non-PLD globes; however, PL thickness was not specifically measured. Furthermore, in the study by Smith et al, 25 alterations of the termination of DM were consistently a feature of PLD-associated glaucoma, regardless of breed, and were not encountered in eyes with secondary glaucoma. Our study did not find similar results. Although 2/3 examiners were more likely to histologically diagnose PLD if alterations in the termination of DM were noted, our masked results demonstrate that alterations in the termination in DM also exist in dogs clinically unaffected with PLD.
Limitations of light microscopic studies are extensive such that the globes examined are at the end-stage of glaucoma and have been subjected to a variety of medical and/or surgical therapies. Furthermore these globes exhibit chronic and advanced morphologic changes such that early changes in the ICA and CC cannot be observed, making it difficult to distinguish cause versus effect. Further prospective studies including the use of other imaging modalities such as optical coherence tomography and high frequency ultrasound are necessary on dogs affected with PLD, with and without glaucoma, to evaluate the ICA.
Based on this study we believe that using routine histologic examination, a histologic diagnosis of PLD in comparison to angle recession is not possible in canine globes affected with chronic glaucoma. All dogs affected with glaucoma should have gonioscopy performed to verify PLD, and this clinical information should be provided to the pathologist with the enucleated globe.
Footnotes
Acknowledgements
The authors would like to acknowledge Larhonda Sobchishin for her technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the Companion Animal Health Fund, University of Saskatchewan.