
Abstract
The current study aimed to determine the specificity, and to a lesser extent the sensitivity, of canine pancreatic-specific lipase (cPL) concentration in dogs with various disease conditions. Dogs were presented for postmortem examination and had serum collected for cPL concentration within 6 hr preceding death or immediately postmortem. Pancreatic tissue was collected postmortem, and sections from the left lobe, right lobe, and body of the pancreas were examined histologically. Inflammation and fibrosis in each section were assessed to determine a total pancreatic inflammatory score and pancreatic fibrosis score in each dog. Correlations between these scores and the cPL concentration were made, as well as determination of specificity. A total of 32 dogs were included in the analysis, 20 of whom had no to minimal pancreatic inflammation. The specificity of cPL with a cutoff value of 200 µg/l was 80% (95% confidence interval [CI]: 56–94%), while with a cutoff of 400 µg/l, the specificity was 90% (95% CI: 68–99%). There was a significant but rather low correlation between cPL concentration and the pancreatic inflammation score, but not with the fibrosis score. Canine pancreatic-specific lipase concentration has good specificity overall in dogs without pancreatitis. This test is less useful in dogs with milder pancreatitis, and both false-positive and false-negative results occur. Results indicated that dogs with clinical signs suggestive of pancreatitis would require abdominal imaging in addition to serum cPL testing to evaluate the cause (or causes) of clinical signs.
Introduction
Pancreatitis in dogs is a commonly diagnosed condition in veterinary clinics worldwide.1,3,5,8,25 Clinically, pancreatitis in dogs results from an acute inflammatory or necrotizing process centered on the pancreas, with variable systemic complications. 5 Histologically, acute pancreatitis is defined as a neutrophilic inflammation, without fibrosis or exocrine atrophy, and usually is present within the body of the pancreas and/or peri-pancreatic fat. 14 The pathological distinction between acute pancreatic necrosis, acute pancreatitis, acute peri-pancreatic necrosis, and acute peri-pancreatic steatitis may reflect a different pathogenesis; however, the clinical signs of the disease will be similar, as the same systemic effects can occur with any of these diseases. 7 Chronic pancreatitis is defined as a mononuclear (often lymphocytic) inflammation, with disruption of the pancreatic architecture due to concurrent fibrosis.5,26 The presence of nodular hyperplasia in the pancreas of dogs is now considered an incidental finding, with an increased presence in older dogs. 13 It has also been shown that pancreatic inflammation is present variably throughout the pancreas, and so single biopsies may miss the true extent of the disease. 12 Histologic grading schemes have been published that take into account the uneven distribution of the inflammatory changes in categorizing exocrine pancreatic disease.14,26
Evidence would suggest that chronic pancreatic inflammation is more common than previously thought, but diagnosis is difficult due to a failure of laboratory testing or imaging modalities to detect it.21,25 Acute pancreatitis is considered easier to diagnose, but this diagnosis is often reliant on ultrasound imaging, something not always available to veterinary surgeons. Acute pancreatitis usually pre-sents with acute vomiting and/or diarrhea, in combination with abdominal pain and anorexia. This combination of clinical signs is not pathognomonic for acute pancreatitis, and other conditions, such as septic peritonitis, acute renal failure, intestinal obstruction, and others, are also associated with similar clinical signs.
Spec-cPL™ is a monoclonal enzyme-based assay a that was developed from the original enzyme-linked immunosorbent assay for canine pancreatic-specific lipase (cPL) immunoreactivity, 23 and the results of each assay are closely correlated. 21 Canine pancreatic-specific lipase has been shown to be virtually undetectable in dogs with exocrine pancreatic insufficiency, 22 and immunohistochemical studies have determined it is localized in the exocrine pancreas. 20 Canine pancreatic-specific lipase immunoreactivity has been reported to have a sensitivity ranging from 63.6% to 82% for the diagnosis of pancreatitis (Steiner JM, Broussard J, Mansfield CS, et al.: 2001, Serum canine pancreatic lipase immunoreactivity (cPLI) concentrations in dogs with spontaneous pancreatitis. J Vet Intern Med 21:274. Abstract). 21 The sensitivity appears to be higher in studies where the disease is more severe in nature. This sensitivity is comparable to a reported sensitivity ranging from <50% to ≤78% for total lipase, using 3 times the upper reference interval as the diagnostic cutoff point.1,3,8 One of these studies established a specificity of 55% for total lipase. 8 Dogs with acute renal failure, intestinal foreign bodies, acute enteritis, and liver disease have all been shown to have increased total serum lipase concentration.8,15,17,24 A study published in 2011 assessing dogs with no clinical or histologic signs of pancreatitis (essentially healthy dogs) determined a specificity of >95% for cPL immunoreactivity assay. 11 The aim of the current study was to determine the specificity, and to a lesser degree the sensitivity, of the Spec-cPL assay in a population of sick dogs, using histological assessment of pancreata as the gold standard for diagnosis.
Materials and methods
Dogs that were submitted for postmortem pancreatic examination, regardless of the cause of death or antemortem diagnosis, to Murdoch University School of Veterinary and Biomedical Sciences (Perth, Western Australia) during the period from September 2008 to May 2010, were initially recruited for the study. Blood samples were obtained within 6 hr preceding death, or immediately postmortem, and then the serum was harvested and stored at −20°C. Informed owner consent was obtained for all postmortem examinations, and if additional serum was needed, specific consent was also sought. Some owners consented only to the pancreas being removed and not to a full postmortem evaluation. The project was approved by the Murdoch University Animal Ethics Committee, following National Health and Medical Research Council guidelines.
Postmortem evaluation when performed was as standard, and in all dogs samples were obtained from the left lobe, right lobe, and body of the pancreas and fixed in 10% formaldehyde for a minimum of 24 hr. The samples were then processed routinely through graded alcohol into paraffin before sectioning at 5 µm and staining with hematoxylin and eosin for later analysis by the 2 investigators (Mansfield and O’Hara). Both investigators were blinded to the final diagnosis and results of serum testing when reviewing the histopathology. Samples that were too autolyzed for histologic interpretation were excluded, as were cases that did not have 3 pancreatic samples available for assessment.
Histologic grading of the pancreas was adapted from 2 previous studies.14,26 Inflammation was assessed, and the following grading system was used for each of the 3 pancreatic sections, with a total possible cumulative score of 12. Zero indicated no inflammation was present or <2 small foci mononuclear cells were present with no disruption of the architecture; 1 indicated <5% neutrophilic or lymphoplasmacytic inflammation; 2 indicated 5–50% neutrophilic or lymphoplasmacytic inflammation; 3 indicated >50% neutrophilic or lymphoplasmacytic inflammation; and 4 indicated necrosis of pancreatic tissue, or peri-pancreatic necrosis/steatitis. Additionally, the presence of fibrosis was defined as mature fibrous connective tissue replacing the acinar structures or expanding the interstitium. The severity of the fibrosis in each section was scaled according to the following numerical system, with a maximum cumulative score of 9. Zero indicated no fibrosis was evident; 1 indicated <20% of each section was effaced by mature connective tissue; 2 indicated 20–50% of each section was effaced by mature connective tissue; and 3 indicated >50% of each section was effaced by mature connective tissue. If fibrosis could not be definitely differentiated on routine hematoxylin and eosin–stained sections, additional staining with Sirius red was performed to characterize this more clearly. 26 Other pancreatic changes, such as hemorrhage, edema, hyperemia, neoplasia, and exocrine nodular hyperplasia, in addition to the above, were recorded if present but were not assigned severity scores.
Serum from every dog that was assessed in the study was sent as a batch for measurement of cPL at a commercial laboratory. a For the purposes of the study, a result of <30 µg/l was recorded as 30, and results >1,000 µg/l were recorded as 1,000 to reflect the limit of quantification of the assay. The Spec-cPL assay has previously been shown to have good reproducibility with both inter- and intra-assay coefficient of variation <12%. 4 Current laboratory recommendations are that a result of >400 µg/l is consistent with pancreatitis and that a result in the 200–399 µg/l interval should be considered to possibly signify pancreatitis. 21
For the purposes of analysis, dogs with a cumulative inflammatory score of ≤3 were considered to have subclinical pancreatitis of little to no significance; dogs with a cumulative inflammatory score of ≥4 had pancreatic inflammation of increasing degrees. Concurrently, a cumulative score of ≤2 for fibrosis indicated a mild to minimal degree of chronicity, while ≥3 indicated moderate to severe fibrosis.
Statistical analysis and graphical representation were conducted using a statistical software package. b Statistical difference between groups was determined using the Mann–Whitney U test. Spearman rank correlation coefficient was calculated to determine the association between cPL concentration and the inflammatory and fibrosis scores, respectively. A 2-tailed P-value ≤ 0.05 was considered to be statistically significant.
Results
There were a total of 54 dogs initially included in the study, but only 32 dogs that had all the required data were analyzed. Twenty dogs had a pancreatic inflammation score of ≤3, 5 dogs had a score of 4–5, 4 dogs had a score of 6–8, and 3 dogs had a score of ≥9. Pictorial examples of histologic sections from each of these categories are shown in Figure 1.
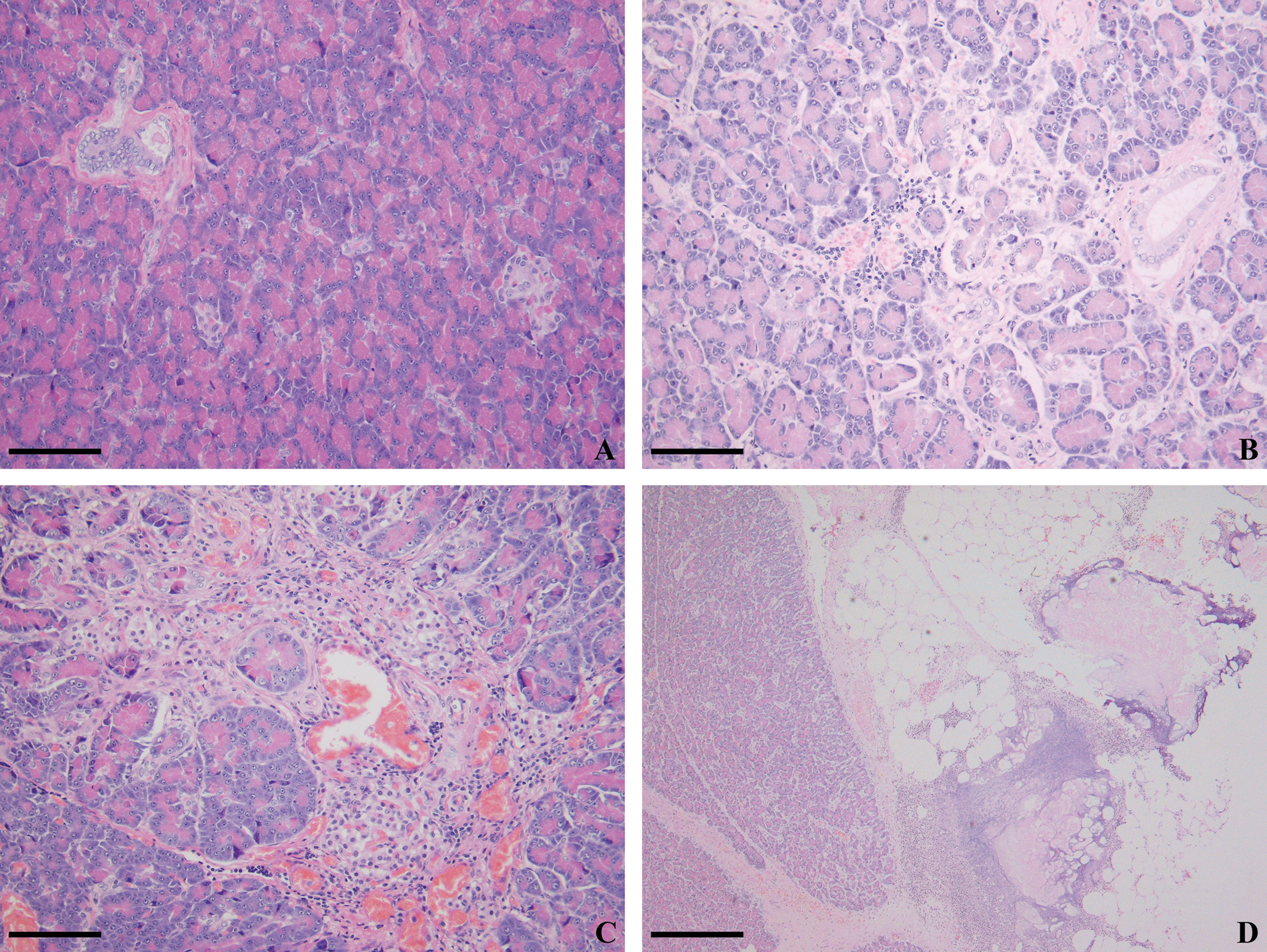
Hematoxylin and eosin–stained sections from 4 dogs with variable pancreatic inflammatory scores (PIS).
In the 20 dogs with a pancreatic inflammatory score of ≤3, the cause of death or euthanasia was determined in 17 and included dog attack (2), and 1 each of the following: vasculitis/coagulopathy, disseminated intravascular coagulation due to anaphylaxis, congestive heart failure, hepatic necrosis, intestinal infarct secondary to nonsteroidal anti-inflammatory drug overdose, osteosarcoma, heart base mass, multiple endocrine neoplasia, lung carcinoma, septic peritonitis (stick foreign body), splenic hemangiosarcoma, metastatic malignant melanoma, snake envenomation, islet cell neoplasia, and metastatic nephroblastoma. In the 12 dogs with a pancreatic inflammatory score of >3, the primary cause of death was identified in 11, and included acute pancreatitis (2), and 1 each of splenic hemangiosarcoma, hemoabdomen secondary to splenic hematoma, small intestinal foreign body, multicentric lymphoma, metastatic carcinoma, pituitary tumor (nonfunctional), pneumonia, septic peritonitis (secondary to hepatic abscessation), and extrahepatic bile duct obstruction due to chronic pancreatitis.
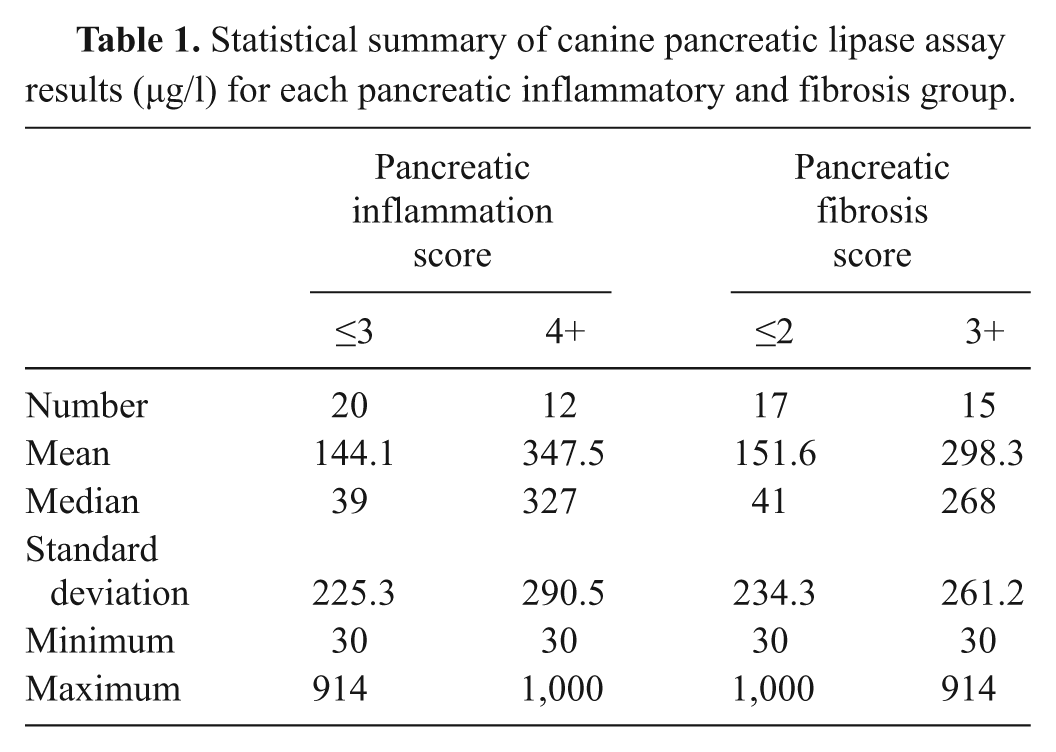
The descriptive statistics for cPL are shown in Table 1. There was a statistical difference in cPL concentration between dogs with a pancreatic inflammation score of ≤3 and those with a score of >3 (P = 0.011), as demonstrated in Figure 2.
Statistical summary of canine pancreatic lipase assay results (µg/l) for each pancreatic inflammatory and fibrosis group.
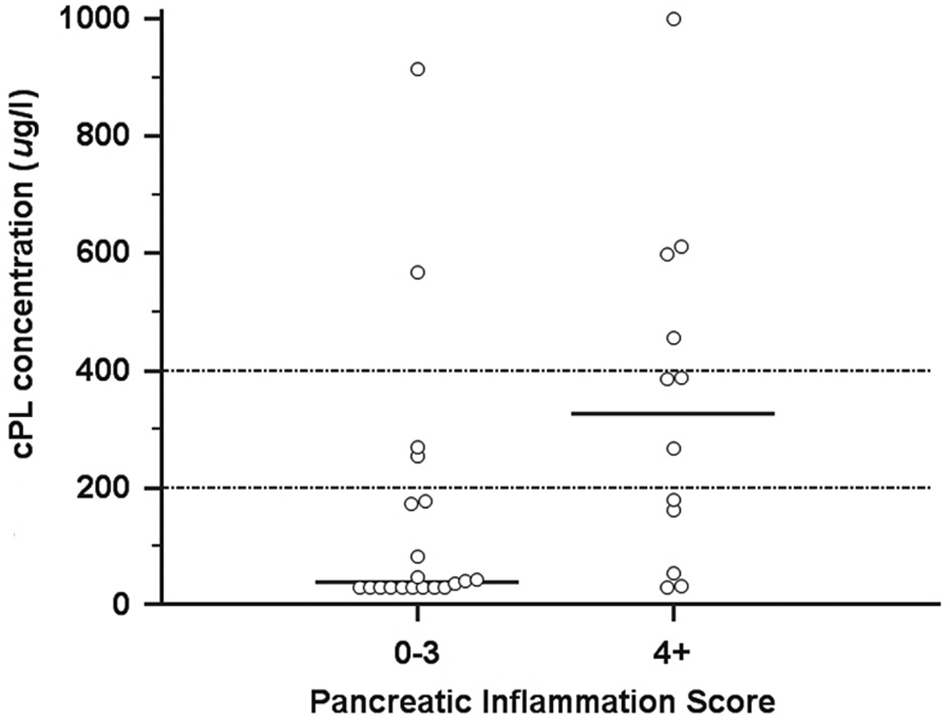
Results of canine pancreatic-specific lipase (cPL) concentrations in 20 dogs with minimal to no pancreatic inflammation (pancreatic inflammation score of ≤3) and in 12 dogs with scores of 4+. The median concentration is represented by the short horizontal bar.
Seventeen dogs had a fibrosis score of ≤2, 10 of which had no observed fibrosis. Thirteen dogs had a moderate (score: 3–6) degree of fibrosis, and 2 had severe (score: ≥7) fibrosis (Table 1). There was no statistical difference in cPL concentration between dogs with a pancreatic fibrosis score of ≤2 and those of >2 (P = 0.055).
Hemorrhage was observed in samples from 8 dogs, all with pancreatic inflammation scores of ≤3. Hemorrhage was not observed uniformly throughout all sections in each dog. Additionally, nodular exocrine hyperplasia was identified in 2 dogs. No edema was noted.
Spearman rank correlation coefficient between pancreatic inflammation score and cPL was significant (rs = 0.47; 95% confidence interval [CI]: 0.15–0.71; P = 0.0060), as demonstrated in Figure 3. There was no correlation between pancreatic fibrosis and cPL (rs = 0.30; 95% CI: −0.05 to 0.59; P = 0.091).
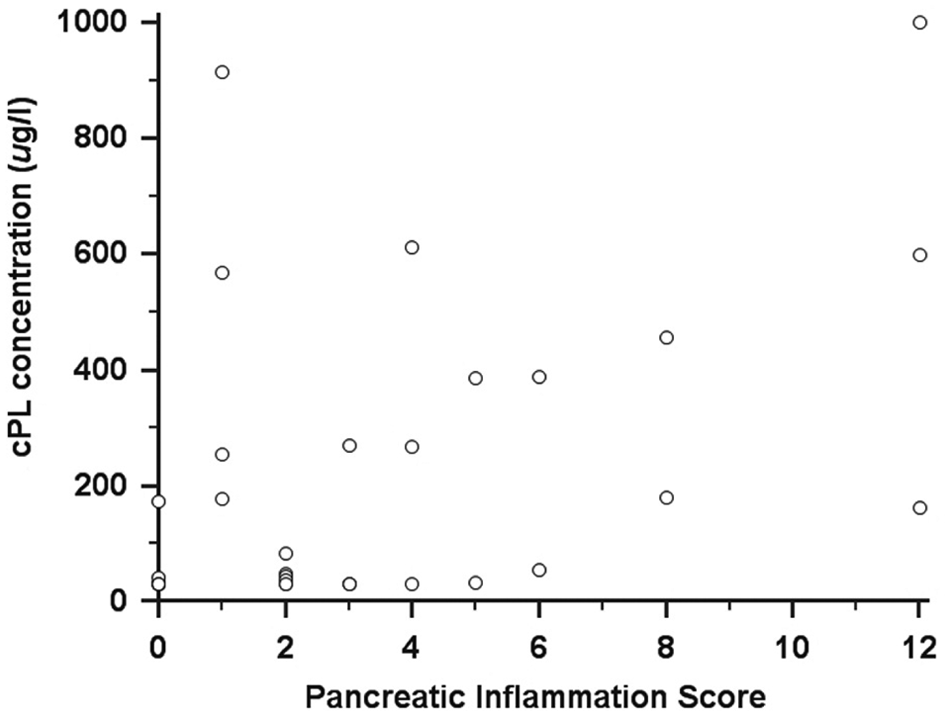
Scatterplot of pancreatic inflammation score and canine pancreatic-specific lipase (cPL) concentrations in 32 dogs. Spearman rank correlation coefficient 0.47 (P = 0.0060).
When using 400 µg/l as a diagnostic cutoff for cPL concentration and a pancreatic inflammation score of ≤3 to indicate no histologic pancreatitis, there were 2 false positives. These 2 dogs had cPL concentrations of 914 µg/l and 568 µg/l, respectively, and pancreatic inflammation and fibrosis scores of 1 and 3, respectively. No other pancreatic abnormalities were observed. When using a diagnostic cutoff for cPL concentration of 200 µg/l, there were 4 false positives. The additional 2 dogs had cPL concentrations of 270 µg/l and 255 µg/l, respectively, with pancreatic inflammation and fibrosis scores of 3.3 and 1.3, respectively. This correlates to a specificity of 90% (95% CI: 68–99%), using a cPL concentration cutoff value of 400 µg/l, and 80% (95% CI: 56–94%), using a cutoff value of 200 µg/l. The area under the receiver operating characteristic curve was 0.77 (95% CI: 0.59–0.90).
There were 12 dogs in the present study that had a histologic diagnosis of pancreatitis (a pancreatic inflammation score of ≥4). By using 400 µg/l as a diagnostic cutoff concentration for cPL, there were 4 true positives (4/12, sensitivity 33%, 95% CI: 10–65%), whereas using the diagnostic cutoff value of 200 µg/l, there were 7 true positives (7/12, sensitivity 58.3%, 95% CI: 28–85%). Three of the 12 dogs had peri-pancreatic fat necrosis present but minimal to no inflammation present within the pancreatic interstitium. On analysis of these 11 dogs designated true positives, with histologic pancreatitis and a known cause of death, only 3 had pancreatitis as the primary cause of their clinical signs.
Discussion
The pathogenesis of clinical pancreatitis is complex and multifactorial. The clinical signs from acute pancreatitis may result purely from the local effects of the pancreatic digestive enzymes released into the cranial abdomen when trypsinogen is activated to trypsin within the pancreatic acinar cell. 18 Pancreatic safeguards such as pancreatic secretory trypsin inhibitor can become overwhelmed, allowing trypsin activation to spill into the interstitium. 2 Circulating antiproteases (such as α-macroglobulin or α1-protease inhibitor) are responsible for binding to proteases and clearing them through the reticuloendothelial system, but these too may become overwhelmed in individual animals. 6 Circulating pancreatic proteases are then capable of inciting inflammation systemically via activation of free-radical, coagulation, complement, and kinin cascades. 19 The generation of chemokines and cytokines leads to further tissue inflammation and injury, which in turn may cause multiorgan failure and death. As such, determination of histologic severity alone cannot conclusively determine if an animal has clinically severe pancreatitis. Additionally, it is possible that mild pancreatic inflammation may be along the spectrum of normal in dogs, and it is the way the body responds to that inflammation that determines if clinical disease is manifested.
Along those lines, the current study demonstrates the difficulty in truly defining clinical pancreatitis based on histologic grading alone. One postmortem survey identified 92% of dogs in a referral institution to have pancreatic inflammation, 14 while another study found approximately 34% of dogs surveyed in a first-opinion clinic to have chronic pancreatitis. 26 As it seems highly unlikely that 90% of sick dogs will be sick due entirely to pancreatitis, it can be surmised that histologic pancreatitis does not always translate to clinically important pancreatitis. It has not been established what percentage of the pancreas needs to have inflammation present before it can be truly categorized as having clinically important pancreatitis. It is interesting to note that in the current study, of the 11 dogs with histological pancreatitis (an inflammation score of >3) and a known cause of death, only 3 had pancreatitis as the primary cause of their clinical presentation. This highlights the need to consider the pancreas as a participant in many presentations, rather than as an instigator.
The use of the current scheme was an attempt by the authors to correct for the potential discrepancy between histologic and clinical pancreatitis. While it is possible that a dog with a pancreatic inflammation score of ≥4 in the present study did not have clinical pancreatitis, the 8 dogs that were designated to be false negatives all had inflammation scores of ≥5 and had clinical signs of pancreatitis. The possible reason for this discrepancy is that 4 of the 8 had predominantly peri-pancreatic fat necrosis, with little to no inflammation or necrosis of the pancreatic interstitium. One possible explanation for this is that the disease may have initiated in the peri-pancreatic fat, and inflammation centered on the pancreas itself had yet to develop. This may have resulted in less stimulation of the pancreatic enzyme cascade than if it had involved the interstitium. This also raises an interesting alternative conjecture in that this subgroup of dogs may not have true pancreatitis as is currently understood (where trypsinogen is activated within the acinar cell as the initiating event). Rather, the disease may actually be initiated in fat within the abdomen and extend toward the pancreas. The role of adipokines in initiating inflammation is increasingly being recognized in human and veterinary fields.10,16 Clinically, these 2 possibilities would be impossible to differentiate. As 3 of these 4 dogs had clinical signs (abdominal pain, vomiting) for more than 3 days, lack of opportunity for inflammation to develop seems unlikely.
When using a cutoff value of 400 µg/l, the specificity of cPL concentration in the current study was 90%, and when using a cutoff value of 200 µg/l, the specificity was 80%. Caution should be taken when interpreting these results, however, as the postmortem nature of the current study biased the selection of cases. By the very nature of requiring the pancreas in its entirety, the study is preselecting for dogs with severe disease. Additionally, the study only assessed dogs presented for postmortem at a referral institution. Dogs with diseases that have similar clinical signs to pancreatitis (e.g., intestinal foreign body, acute gastroenteritis) are more likely to be treated at a general veterinary practice or survive their illness. This, combined with a lack of a noninvasive gold standard, makes it extremely difficult to assess the true clinical specificity of cPL in a large population of dogs with acute gastrointestinal signs.
The dogs in the current study with false-positive results had a number of underlying causes of death or euthanasia, and none was considered likely to have pancreatitis as a primary problem. That being said, it is possible that the inflammation score determined in the present study did not accurately reflect changes throughout the pancreas. Previous studies have identified that histologic changes in the pancreas are not uniformly distributed throughout the organ. 12 The current study assessed samples from the left and right lobes, as well as from the body of the pancreas. Although the entire pancreas was not sectioned, the authors felt this was representative of an overall inflammatory assessment. Other possible reasons for the false-positive results include cross-reactivity with other lipases (which seems unlikely based on previous work), excessive production of pancreas-specific lipase by the pancreas in the absence of pancreatic inflammation, or production of this isoenzyme of lipase in an organ (or organs) other than the pancreas. It is not possible from the current information to postulate on the most likely cause.
The current study did not include any dogs with renal failure, and increased total lipase has been identified in dogs with renal failure.8,24 Further work assessing cPL and pancreatic inflammation in dogs with renal failure is required before conclusions can be made regarding this particular aspect.
Recent papers have established similar sensitivities for measurement of serum canine pancreatic elastase-1 (cPE-1) 9 to what has previously been reported for cPL. 21 Again, with both analytes, the sensitivity increases when more severe forms of pancreatitis are assessed. The current study actually reported a much lower sensitivity for cPL (33–58%) than what had previously been reported; however, caution should be exercised in overinterpreting this aspect due to the very small numbers of animals with true disease. The dogs in the present study were presented for postmortem evaluation and were not necessarily considered likely to have pancreatitis. In a recent study, the specificity for cPE-1 was also reported to be approximately 92%, 9 similar to the result reported for cPL concentration in the present study.
The specificity identified in the current study is similar but slightly lower than another study published assessing the histologic and gross appearance of the pancreas. 11 The slightly lower value in the present study may be due to only sick dogs being assessed, while almost two-thirds of the dogs without pancreatitis in the referenced study were clinically healthy. 11 To date, the current sensitivity and specificity for clinical suspicion combined with imaging findings to diagnose pancreatitis in dogs is not known. It can certainly be extrapolated that no single laboratory test will replace good clinical acumen and imaging of the abdomen but, rather, can serve to enhance it.
In the current study of pancreatic histology obtained postmortem in dogs, cPL concentration had a specificity ranging from 80% to 90%, dependent on which value (200 µg/l and 400 µg/l, respectively) was used as the lower limit in the analysis. The sensitivity for this test ranged from 33% to 58% (using 400 µg/l and 200 µg/l, respectively), which is less than previously reported. The authors recommend that additional testing, especially abdominal imaging, should aid in the diagnosis of the primary problem in dogs presenting with vomiting and/or abdominal pain.
Footnotes
Acknowledgements
The authors would like to thank all clinical staff at Murdoch University Veterinary Hospital who assisted in management and recruitment of cases, and the staff of the Clinical Pathology and Anatomical Pathology Departments at Murdoch University in the collection, preparation, and handling of samples.
a.
IDEXX Laboratories, Brisbane, Queensland.
b.
MedCalc 11.6.1, MedCalc Software, Mariakerke, Belgium.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.