
Abstract
Chronic kidney disease (CKD) is the most common metabolic disease of domesticated cats, with most affected cats being geriatric (>12 years of age). The prevalence of CKD in cats exceeds that observed in dogs, and the frequency of the diagnosis of CKD in cats has increased in recent decades. Typical histologic features include interstitial inflammation, tubular atrophy, and fibrosis with secondary glomerulosclerosis. In contrast to people and dogs, primary glomerulopathies with marked proteinuria are remarkably rare findings in cats. Although a variety of primary renal diseases have been implicated, the disease is idiopathic in most cats. Tubulointerstitial changes, including fibrosis, are present in the early stages of feline CKD and become more severe in advanced disease. A variety of factors—including aging, ischemia, comorbid conditions, phosphorus overload, and routine vaccinations—have been implicated as factors that could contribute to the initiation of this disease in affected cats. Factors that are related to progression of established CKD, which occurs in some but not all cats, include dietary phosphorus intake, magnitude of proteinuria, and anemia. Renal fibrosis, a common histologic feature of aged feline kidneys, interferes with the normal relationship between peritubular capillaries and renal tubules. Experimentally, renal ischemia results in morphologic changes similar to those observed in spontaneous CKD. Renal hypoxia, perhaps episodic, may play a role in the initiation and progression of this disease.
Keywords
Chronic kidney disease (CKD) is the most common metabolic disease of domesticated cats. Reflecting differences in patient populations, such as age and diagnostic criteria, estimates of the overall prevalence of feline CKD have ranged from 1% to 3% 9,165 to 50%. 138 Although many cats with CKD would be expected to die of nonrenal causes, in a necropsy study renal disease was the cause of death in 4% of cats dying at 1 to 5 years of age and in 17% of cats dying at ≥11 years of age. 90 In a study of longevity in companion animals in the United Kingdom, mortality was attributed to renal disorders in 12.1% of cats, with this diagnosis being the most frequently (13.6%) identified cause of mortality at or after 5 years of age in cats. 153 In a Swedish study of cats that were insured up to 13 years of age, disorders of the kidneys or ureters were the most commonly identified cause of mortality, with an age-standardized mortality rate of 713 per 10 000 cat-years at risk. 63 Feline CKD is a frequent diagnosis in clinical practice and the most common metabolic disease in cats presented to a veterinarian for evaluation. 132 The prevalence in cats is higher than that observed in dogs, 160 with a recent estimate of apparent prevalence of CKD of 0.21% in dogs. 154 Interestingly, in another member of the Felidae family (captive populations of cheetahs), CKD is also a common finding. 19,149,150
Although there are limited data on the prevalence of CKD in cats, studies have identified 2 consistent trends in the prevalence of feline CKD. First, as in dogs, 9,160 congenital disease causes a transient increase in prevalence of CKD in animals <3 years of age, and the prevalence of CKD increases with advancing age from 5 to 6 years onward. Estimates of the prevalence of CKD in geriatric cats have ranged from 35% 9,118 to 81%. 138 When data in dogs and cats were similarly obtained, the prevalence of CKD in geriatric cats exceeded that observed in geriatric dogs by 2-fold or more. 160 A second trend is the increasing prevalence of the diagnosis of CKD in cats during recent decades. Data from the Purdue Veterinary Medical Database suggests that the overall prevalence of feline CKD increased from 0.04% in the 1980s to 0.2% in 1990s to 1% by the 2000s. 131,165,167 Whether this increase is a reflection of increased awareness with enhanced diagnostic acumen, an increase in the median age within cat populations, 21,63 or a true increase in prevalence is unknown.
Clinical Findings
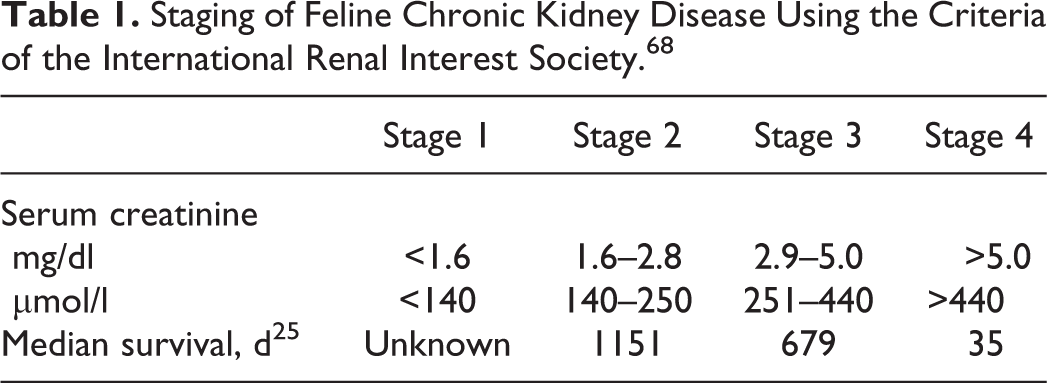
The severity of CKD in cats varies and may be staged according to recommendations of the International Renal Interest Society (IRIS; Table 1). 68 In general, the prevalence of CKD-associated complications (ie, hyperphosphatemia, secondary renal hyperparathyroidism, hypokalemia, anemia, proteinuria, systemic hypertension, metabolic acidosis, and uremia) rises with advancing stage 68 such that the treatment 68 and the prognosis 25 vary with IRIS CKD stage. With few exceptions, these manifestations are common to all causes of CKD in cats, are similar to those observed in other species, and have been the subject of recent reviews. 9,159,165
Staging of Feline Chronic Kidney Disease Using the Criteria of the International Renal Interest Society. 68
Pathologic Findings
Although primary glomerular diseases, such as immune complex glomerulonephritis 83,151 and amyloidosis, 7,24 are described in cats and may result in chronic tubulointerstitial lesions (Figs. 1, 2), the majority of geriatric cats with CKD do not have histologic evidence of primary glomerular disease. 47,130,143 Instead, in the majority of cats with CKD, the primary lesions are within the tubulointerstitial compartment with only mild, presumed secondary, sclerotic lesions occurring within glomeruli. 47,143 Grossly, kidneys from cats with CKD are decreased in size with surface pitting (Fig. 3). Histologically, renal lesions are multifocal to segmental (Fig. 4) and include interstitial mononuclear cell inflammation, tubular degeneration and atrophy, interstitial fibrosis, mineralization of Bowman's capsule and tubular basement membranes, interstitial lipid, and glomerulosclerosis. 47,143
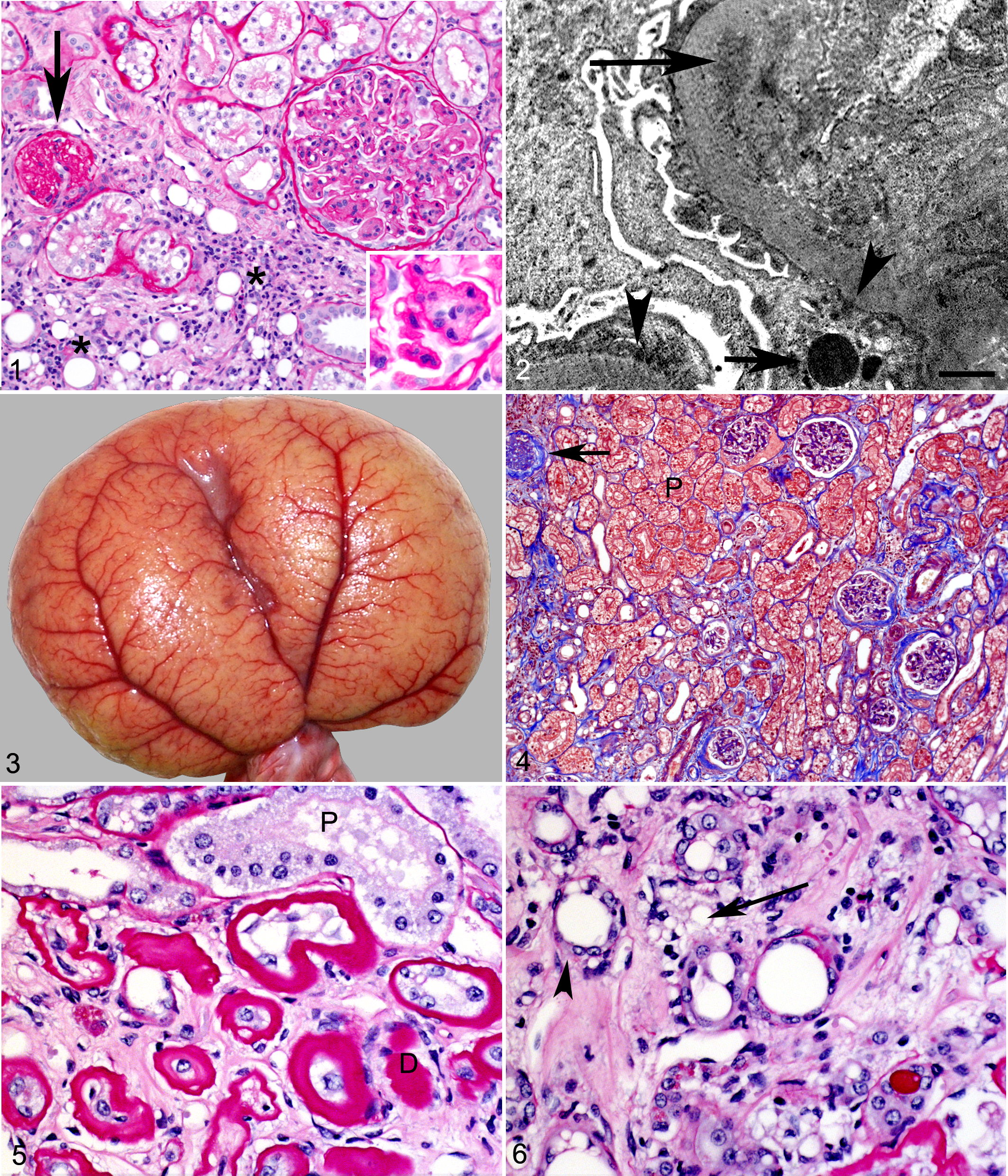
While tubular atrophy, interstitial inflammation, and fibrosis are present in all cats with CKD, they are more severe in more advanced disease. 47,143 The inflammatory infiltrate typically consists of lymphocytes, which may be the sole inflammatory cell type present in IRIS CKD stage 1 143 or may be admixed with plasma cells and macrophages and are typically present within the interstitium surrounding atrophic tubules. Atrophic cortical tubules often occur in clusters, are decreased in size, and exhibit basement membrane thickening and wrinkling (Fig. 5) or thinning (Fig. 6). Interstitial lipid accompanied by granulomatous inflammation is common in IRIS CKD stages 2 to 4 and may be secondary to tubular ischemia and rupture, 143 with release of intraepithelial lipid (Fig. 6). Interstitial fibrosis accompanies the interstitial inflammation and tubular atrophy, is correlated with the severity of the azotemia, 47 and is most severe in cats with IRIS CKD stage 4. 143
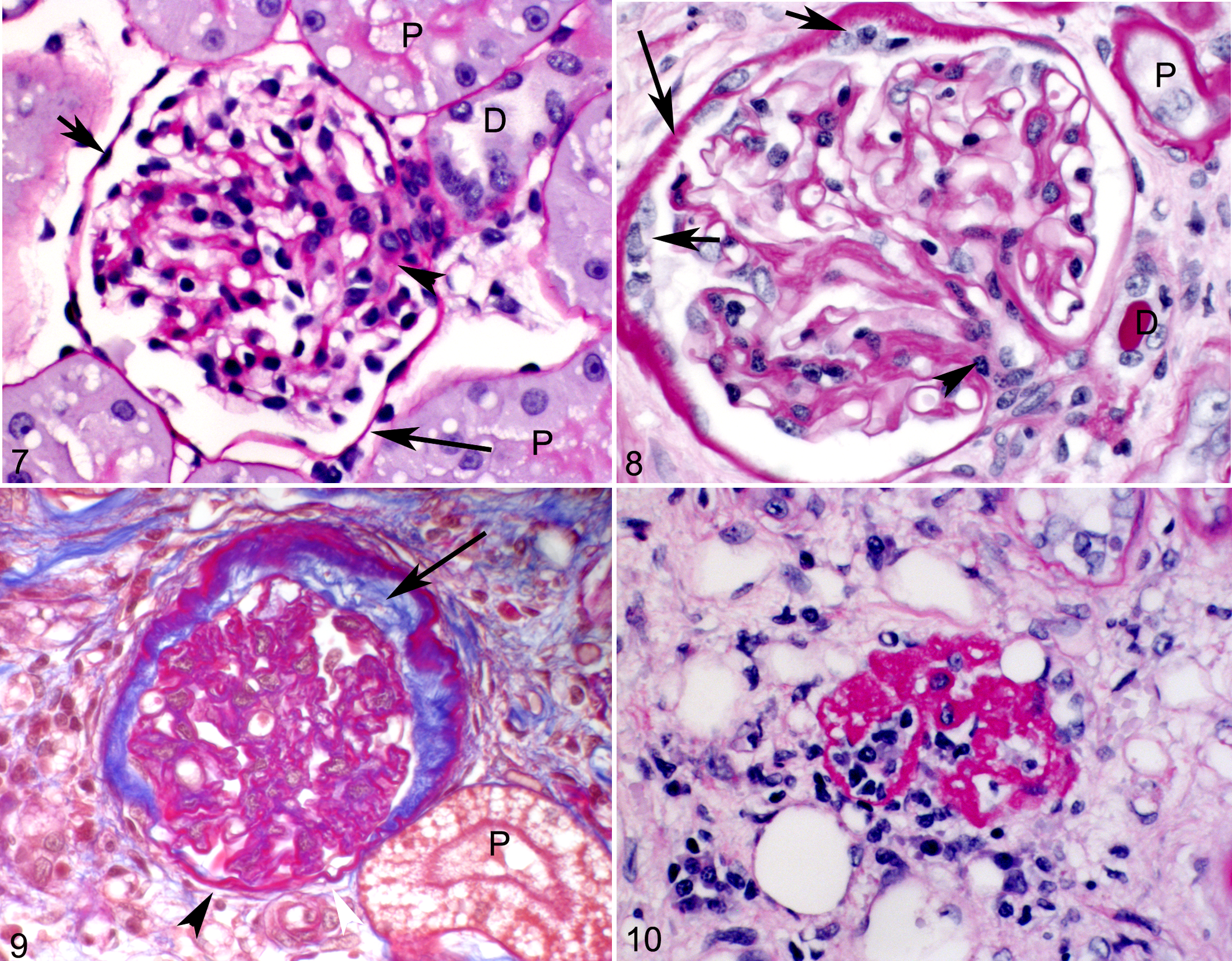
Within affected kidneys, glomeruli often are increased in size (glomerular hypertrophy) and may exhibit mild expansion of the mesangial matrix (glomerulosclerosis; Figs. 7, 8). 47 In cats with more profound nephron loss, hyperperfusion of enlarged glomeruli 33 may cause podocyte damage and loss, resulting in the lesion of focal segmental glomerulosclerosis. Compared with dogs, 40,74,75 secondary glomerulosclerosis in the remnant kidney model is comparatively mild in cats 73 and in spontaneous feline CKD focal segmental glomerulosclerosis, when present, similarly affects relatively few glomeruli and only a small portion of the capillary tuft. 47 Varying proportions of glomeruli in cats with CKD are decreased in size and are globally sclerotic or obsolescent. While global glomerulosclerosis appears to be a normal aging change in geriatric cats, it is also a pathologic change that increases significantly in severity in progressive stages of CKD. 143 In cats with CKD, globally sclerotic glomeruli may exhibit thickening and wrinkling of the glomerular basement membrane, collapse of the capillary tuft, and fibrosis within the urinary space (Fig. 9). These changes are more consistent with ischemic glomerular obsolescence rather than progression of focal segmental glomerulosclerosis. 96 Shrunken globally sclerotic glomeruli may be difficult to discern within the fibrotic interstitium (Fig. 10).
Pathogenesis of Feline CKD
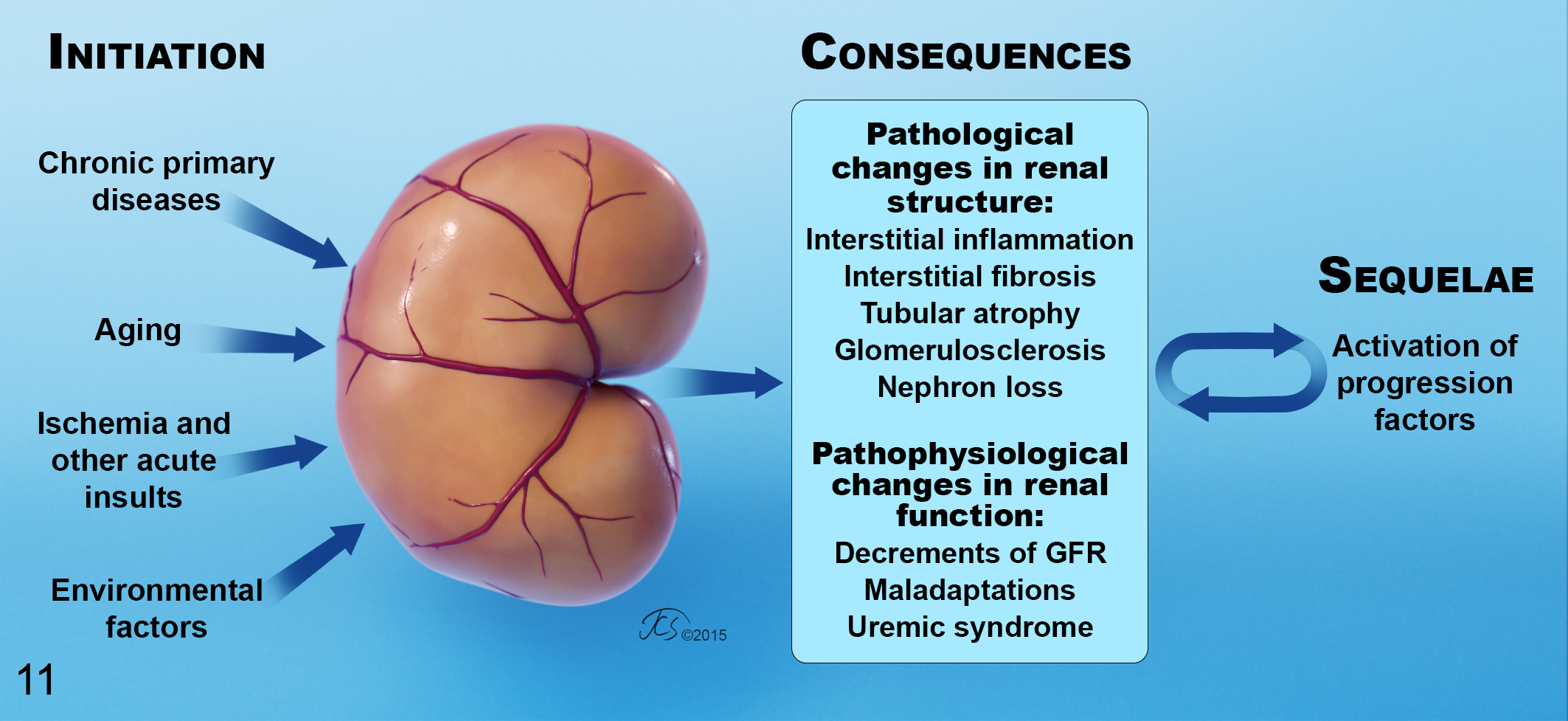
The traditional view of the course of CKD 26,38 is that an initiation phase precedes a progression phase. In this scenario, a primary renal disease (eg, diabetic nephropathy, immune complex deposition) initiates the damage to the kidneys, resulting in nephron loss in early CKD. Eventually, enough nephrons are lost such that other factors, intrinsic to the affected animal, produce self-perpetuating renal injury in what is termed inherent or intrinsic progression. This scenario, with initiation and subsequent activation of progression factors, is presumed to be the situation in cats with CKD (Fig. 11).
Chronic Primary Renal Diseases
In other species, it is generally thought that a primary renal disease serves as the initiating factor for the CKD, and this primary disease is often referred to as the “cause” of the CKD. A variety of primary renal diseases that can cause CKD have been identified in cats:
With the exception of AKI, most of these known primary renal diseases affect only specific breeds of cats (eg, amyloidosis, renal dysplasia, polycystic kidney disease), are believed to affect a very small number of animals (eg, unbalanced diets, immune complex glomerulonephritis), or produce histologic changes (eg, amyloidosis, lymphoma, polycystic kidney disease) that are inconsistent with the pathologic changes of CKD 47,61,143 that are usually observed in the kidneys of affected cats. Some of these chronic renal diseases, such as bacterial infection and uroliths, might be expected to produce histologic changes consistent with typical observations in affected feline kidneys. For example, bacterial urinary tract infections are relatively more common in cats with CKD, 142 and upper tract infection would be expected to produce tubulointerstitial changes. However, antibiotic treatment of cats with CKD with a concomitant bacterial urinary tract infection does not affect survival, 200 and most cats with CKD have sterile urine. 142 Ureteroliths and nephroliths are observed in some cats with CKD, but these typically are unilateral. Furthermore, most cats with unilateral ureteroliths have a small contralateral kidney, 122 suggesting that the CKD was preexisting. 165
Viral infections have been considered as possible initiating causes of CKD in cats. In people, human immunodeficiency virus–associated nephropathy is predominantly a glomerular disease that is accompanied by less specific tubulointerstitial lesions. 55 A similar virus occurring in cats, feline immunodeficiency virus (FIV), is associated with mild proteinuria, 11 and both glomerular amyloidosis and presumed immune complex glomerulonephritis have been described in FIV-positive cats. 158 In addition to these glomerular lesions, nonspecific tubulointerstitial changes were noted in FIV-positive cats. However, in comparing FIV-infected and FIV-noninfected cats in the clinical setting, the incidence of azotemic renal disease was similar in both groups, suggesting that FIV may not be a significant cause of CKD in cats. 11
A recent report described the isolation of a paramyxovirus, feline morbillivirus, from 56 (12%) of 457 feral cats in China and suggested an association between tubulointerstitial renal disease and viral infection. 204 Necropsies performed on 12 virus-positive and 15 virus-negative feral cats revealed nonspecific tubulointerstitial nephritis in 7 and 2 cats, respectively. Distinguishing these changes from relatively common spontaneous CKD renal lesions is difficult, and further investigation into this potential association between paramyxovirus infection and tubulointerstitial nephritis is warranted.
In people 2,117,181 and dogs, 54,115,173,190 a variety of primary and secondary glomerulopathies, including immune complex glomerulonephritis, are initiating diseases in many, perhaps most, cases of CKD. The common primary chronic renal diseases in people (ie, hypertension, diabetes, immune complex glomerulonephritis) 210 involve the glomerulus as a primary target with significant proteinuria as a hallmark. In cats, while proteinuria is an important predictor of progression 48 and mortality 184 as in other species, marked proteinuria and primary glomerular disease are uncommon. Furthermore, diabetes does not lead to significant renal structural or functional changes in cats, 212 and in contrast to those of people, glomerular lesions secondary to feline hypertension are comparatively mild. 47
While it is widely accepted that the presence of CKD enhances the susceptibility of the kidney to toxic or ischemic insults, clinical observations support the notion that an AKI can initiate CKD in people 50 and dogs. 8 Tubulointerstitial changes similar to those observed in feline CKD, particularly interstitial inflammation and fibrosis, occur during the recovery phase of an AKI, 109 and have been observed in cats following experimental renal ischemia. 171 After an AKI, these repair mechanisms may become maladaptive, leading to CKD. 69 The importance of AKI as an initiator of spontaneous CKD in cats has not been well studied.
While the specific renal diseases cited above are causative in some cats with CKD, in contrast to dogs and people with CKD, the majority of cats with CKD lack an apparent initiating cause. 47 It is unlikely that the tubulointerstitial changes observed in cats with CKD simply represent the final common pathway of renal destruction 38 even when observed in IRIS CKD stage 4, since these same lesions are observed in early feline CKD, 47,143 albeit to a lesser extent. The presence of similar tubulointerstitial changes in early and advanced stages of feline CKD is consistent with the proposal that ≥1 primary tubulointerstitial insults are critical initiation factors in feline CKD. While it is tempting to speculate that a single, previously unknown primary disease such as an infectious or genetic 17 etiology will be uncovered, it seems more likely that a combination of intrinsic (animal) factors, environmental factors, and/or repeated intermittent acute kidney insults (AKI) act in concert as initiating or causative factors.
Aging as an Initiation Factor
An abundance of evidence supports a link, perhaps causal, between aging and feline CKD: Increased prevalence of sclerotic glomeruli in kidneys from geriatric cats
143
Shortened telomere length in aged cats with CKD
162
Enhanced susceptibility of geriatric people to renal insults
172,195,196
Alterations in antioxidant defenses in feline CKD
111,120,209
Increased prevalence of comorbid conditions in older cats, particularly those known to affect the kidneys, such as hyperthyroidism, systemic hypertension, dental disease, and inflammatory bowel disease
Since (1) the prevalence of CKD is greatest in geriatric populations in all species, (2) the majority of cats have an idiopathic disease, and (3) at least one other group of felids (captive cheetahs) has a similarly high prevalence of CKD, 19,149,150 it is tempting to suggest that CKD is part of the aging process in domesticated cats in particular or felids in general. However, this high prevalence in aged cats does not, by itself, establish a role for aging in the initiation of feline CKD. A portion of this increase in prevalence in geriatric cats reflects persistence of CKD rather than a rise in incidence with advancing age, as CKD is not readily reversible and, once acquired, it rarely resolves. The rising prevalence of CKD in people as they age is at least partly due to the accumulation of chronic renal diseases. 210 In a species such as cats 48,73 in which CKD progresses slowly or is the cumulative result of multiple intermittent acute insults over time, a greater prevalence of CKD would be expected in older animals.
Despite intense study, whether an aged kidney is prone to the development of CKD, whether it has heightened susceptibility to acute insults, and whether aging is itself a primary renal disease remain unproven hypotheses. When physiologic, morphometric, and imaging techniques were used to mathematically model glomerular filtration rate (GFR) and its determinants in a group of older (≥55 years) vs younger (≤45 years) human living kidney donors, 186 there was an observable decline in GFR in older donors attributable to glomerulopenia. Clearly, there are similar age-associated changes in feline kidneys. For example, the prevalence of globally sclerotic glomeruli is greater in older (>7 years) vs younger (<5 years) cats. 143 Shortening of telomere length with aging is a genetic factor that could be associated with this glomerular and nephron senescence. When telomere length was assessed in kidney, liver, and skin from 12 cats with naturally occurring CKD, 12 young normal cats, and 6 older normal cats, there was evidence of shortened telomeres and increased cellular senescence in renal epithelium from cats with CKD. 162 However, in this study, age alone did not appear to result in significant telomere shortening, as shortened telomeres were not present in the kidneys, skin, or liver of older normal cats or in the skin or liver from cats with CKD.
As further evidence that CKD is not an inevitable consequence of aging in people and cats, one-third of elderly human beings have a normal GFR, 210 and 19% to 65% of geriatric cats exhibit no clinical evidence of CKD. 9,118,138 Therefore, aging by itself does not initiate CKD. It is plausible, however, that age-associated changes enhance susceptibility to the development of CKD. Aging changes in human kidneys seem to predispose them to injury from a variety of insults, including ischemia, nephrotoxicity, and inflammation, 195,196 and renal function is less likely to recover following kidney damage in aged human beings. 172 Renoprotective systems, such as antioxidant defenses, may be affected in aged cats with CKD. 111,120,209 However, antioxidant defense mechanisms are not exhausted in aged cats, even those with IRIS stage 4 CKD. 120 There are other well-known effects of aging on the kidney. These include mitochondrial dysfunction, heightened intrarenal inflammatory response, and increased cellular senescence. 161 Furthermore, there is an age-associated reduction in Klotho gene expression in people, 211 which is believed to have an adverse effect on vascular regulation and endothelial cell health. 136,139 Any similar, age-associated compromise of protective or reparative systems in cats would be expected to play a role in the response to other insults.
Extrarenal diseases that are more common in aged cats may adversely affect their kidneys. Examples include hyperthyroidism, dental disease, systemic hypertension, and inflammatory bowel disease. In other species, hyperthyroidism increases renal blood flow and GFR and causes hyperplasia and hypertrophy of tubular epithelium, 191 and there is indirect evidence 1,59,88,202,203 that the same kinds of changes occur in the kidneys of hyperthyroid cats. Hyperthyroidism contributes to renal injury in certain settings in rats, 148 but whether hyperthyroidism could cause tubulointerstitial disease in cats remains uncertain. While hyperthyroidism enhances feline renal blood flow, 1 the consequences of this hyperperfusion and the direct effects of excess thyroid hormone on feline tubular cells are not well understood. Hyperthyroidism might be expected to directly—or indirectly, as a result of an increase in GFR 1 —result in disordered nephron enlargement, including podocyte hypertrophy. 119 Podocyte hypertrophy, along with glomerular enlargement, would be expected to result in podocyte loss and focal segmental glomerulosclerosis. However, convincing evidence is lacking, as most cats with CKD do not have overt hyperthyroidism, and the glomerulosclerosis observed in cats with CKD is mild and nonobliterative. 47
In cats, an association between dental disease and CKD has been suggested. 70,89 In people, periodontal disease is a risk factor for the development of CKD 76 and is associated with declining renal function and mortality, 52 perhaps through enhancement of the systemic inflammatory burden. 76,168 Worsening of oral health and periodontal disease have been shown to occur as CKD advances in dogs 84 and in people, 185 indicating that this is a complex, perhaps bidirectional, 77,193 relationship.
A role for systemic hypertension 14,72,179 and intraglomerular hypertension 27,34,35,39,41,94 in the initiation and progression of CKD has been proposed in other species. While systemic hypertension is common in cats with CKD, 65,105,182 it is usually not clear if the high pressures precede or are coincident with the initiation of CKD. If present, increases in blood pressure with advancing age could play a role in the initiation of feline CKD. Although not all studies have found an age-associated change in blood pressure in cats, 176 a longitudinal study demonstrated that blood pressure increases with age in cats, whether they have CKD or are otherwise healthy, 15 and a second study demonstrated a correlation between age and feline blood pressure. 18 However, the importance of the kidneys in the regulation of blood pressure is well known in other species, and a more plausible explanation is that the CKD precedes the hypertension, which then establishes a vicious cycle, contributing to further renal damage as a progression factor and so on. Given the prevalence of CKD and the difficulty of establishing a diagnosis of the early stages of feline CKD, the presence of subclinical CKD, which compromises the ability of the kidneys to regulate blood pressure, would be expected to occur in a population of geriatric cats.
People with inflammatory bowel disease may exhibit tubular dysfunction 79 and tubulointerstitial nephritis. 4,137 Feline inflammatory bowel disease, 107,189,194 particularly long-standing, might be expected to enhance the systemic inflammatory burden and permit access to the kidney for molecules normally retained in the intestinal tract. Either of these changes could contribute to renal injury. However, the nephropathy in people with inflammatory bowel disease is typically mild, and it is difficult to determine if the renal changes are due to the inflammatory disease, drug therapy, or both. 4,157 Whether there is a relation between inflammatory gastrointestinal disease and feline CKD is an interesting, unsubstantiated hypothesis. 197
Ischemia and Other Acute Kidney Insults as Initiation Factors
It has been suggested that renal tubular hypoxia is an important factor in the development and progression of CKD in people. 175 In kidneys, cortical perfusion is much higher than medullary perfusion. As a result, within normal kidneys, the tissue pO2 is approximately 45 mm Hg in the cortex but falls progressively to ∼10 mm Hg in the medulla. 156 The S3 portion of the proximal tubule and the medullary thick ascending limb within the corticomedullary junction are simultaneously metabolically active and comparatively hypoxic, even in normal kidneys; thus, these segments are quite susceptible to hypoxic injury. A single bout of renal ischemia induces chronic structural changes within the feline kidney that mirror findings in feline CKD, specifically tubular atrophy, interstitial fibrosis, and mononuclear inflammation. 171
In this study, 171 the renal artery and vein of 1 kidney were clamped for 60 minutes, and renal changes attributed to this ischemic event were followed over time. Severe lesions of AKI, including tubular epithelial coagulative necrosis and epithelial regeneration, predominantly affected the straight portion of the proximal tubules and thick ascending limb of the loop of Henle within the corticomedullary junction. As expected, the S3 portion of the proximal tubules were affected by this hypoxic insult. 16 These early changes were followed by chronic changes of interstitial fibrosis, tubular atrophy, and mononuclear cell inflammation both diffusely within the corticomedullary junction and as linear foci within the cortex, similar to those seen in cats with naturally occurring CKD (Fig. 12). Increased smooth muscle actin expression, indicative of myofibroblast activation in profibrotic conditions, is present in kidneys from cats with experimental 171 and naturally occurring CKD. 170,207 This study provides evidence that AKI, specifically ischemic AKI, initiates changes that mimic CKD in cats, 171 consistent with the suggestion that maladaptive repair mechanisms following an AKI can lead to CKD. 69
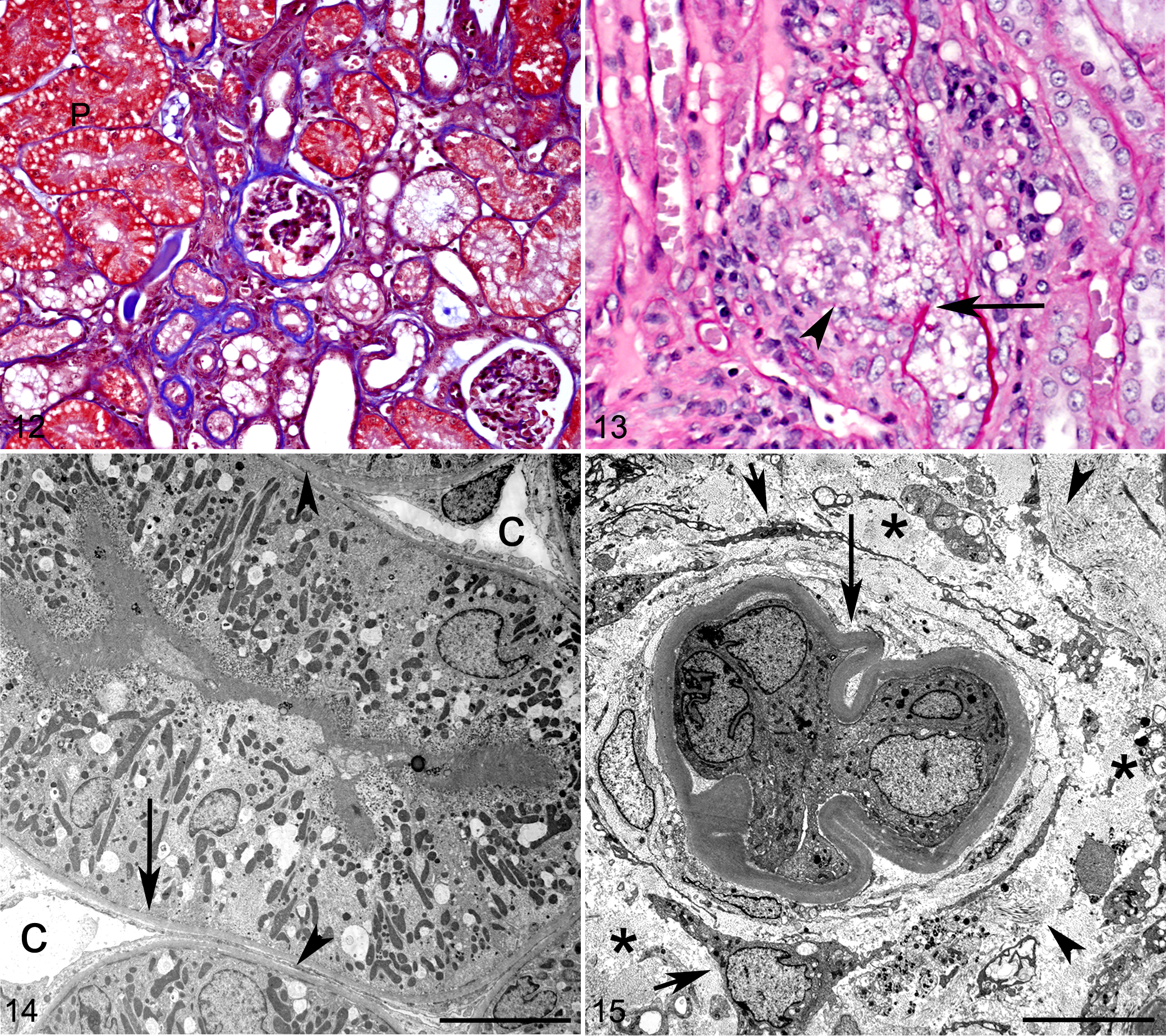
Following acute damage to the kidney, remnant tubular epithelial cells dedifferentiate, proliferate, and replace lost epithelial cells to restore tubular structure. 22 An intact basement membrane plays a crucial role in this regenerative process, providing a scaffold along which regenerating epithelial cells can spread and migrate. 127 Ischemic, in contrast to toxic, insults may be associated with disruption of the tubular basement membrane (ischemic tubulorrhexis). Tubulorrhexis occurs in cats following experimentally induced renal ischemia (Fig. 13). 171 Following tubular rupture, free lipid in the interstitium, presumably derived from tubular epithelial cells, is associated with chronic granulomatous inflammation. Similarly, foci of free lipid and granulomatous inflammation are commonly observed in cats with spontaneous CKD (Fig. 6), which may similarly represent foci of past ischemic tubulorrhexis. In a recent study, most IRIS CKD stage 2 cats and all stage 4 cats had interstitial lipid and associated inflammation 143 as well as tubular degeneration, interstitial fibrosis, and glomerular obsolescence. The changes were significantly more severe in advanced stages 143 and could represent the cumulative effects of multiple ischemic insults.
Inflammation plays a major role in the pathophysiology of ischemic AKI in other species. 23 Endothelial cells, particularly within the outer medulla, are activated after ischemia, resulting in upregulation of leukocyte adhesion molecules. Endothelial injury also results in cell swelling and decreased vessel patency, further contributing to regional ischemia. In addition, proximal tubular epithelial cells contribute to the inflammatory response through their generation of proinflammatory and chemotactic cytokines, such as TNF-α, monocyte chemoattractant protein 1, TGF-β, and IL-6. 23 A reduction in the density of the microvasculature following an ischemic AKI has been hypothesized to play a role in the development and progression of CKD in other species. 10 Chronic hypoxia induced by loss of peritubular capillaries may stimulate tubulointerstitial fibrosis through upregulation of profibrotic factors, such as TGF-β and extracellular matrix genes. As inflammation worsens and interstitial fibrosis separates tubules from peritubular capillaries (Figs. 14, 15), resultant tubular hypoxia would be expected to increase fibrosis, creating a maladaptive positive feedback loop.
Environmental Factors as Initiators of Feline CKD
Besides phosphorus, other dietary factors could play a role in the initiation of feline CKD, as dietary modification has a beneficial effect, apparently to slow the rate of renal damage, in cats with IRIS CKD stages 2 and 3. 167 While important as a progression factor, whether dietary phosphorus intake plays a role in the initiation of feline CKD remains unknown. Similarly, there is evidence for an effect of high dietary sodium intake as a progression factor in established feline CKD 114 but not as an initiation factor in healthy aged cats. 164 Other husbandry factors, such as ad lib feeding of high-protein diets, could play a role in the initiation or progression of feline CKD, as has been hypothesized in people, 27 but evidence that dietary protein intake plays a role is lacking in this species. 73
Certainly unintended consequences of food additives have been shown to cause severe AKI in cats. 28,29,208 Indeed, a relationship between dietary additives, such as ethoxyquin, 91,152 and renal injury in cats has been hypothesized but never established. Potential risks to the health of people from exposure to genetically modified (GM) plants have been discussed, 6,20,180 but we are not aware of any studies of their impact on the kidney of any species. While controversial, there is some evidence that exposure to glyphosate, a herbicide commonly used in GM agriculture, may have toxic renal effects at levels found in the environment and in food 145,146 and that exposure to environmental glyphosate can contribute to the development of CKD in people. 102 We are not aware of any studies in cats that address either the safety of ingestion of GM plants or environmental exposure to glyphosate. In human health, this topic remains politicized, commercialized, speculative, and controversial. 62
The increased prevalence of feline CKD in recent decades might, in part, be attributable to alterations in other environmental factors, such as changes in feeding, housing, or vaccination patterns. Routine vaccination has been hypothesized to be an initiating factor of tubulointerstitial disease and CKD in cats. Vaccine viruses typically have been grown in the Crandell Rees feline kidney (CRFK) cell line. Cats inoculated with CRFK cell lysates or with vaccines grown on CRFK cells develop antibodies against CRFK cells, and these antibodies react with feline renal cell extracts. 125 Putative target antigens have been identified, 201 and lymphocytic-plasmacytic interstitial inflammation has been observed in some cats chronically inoculated with CRFK cell lysates. 124 However, not all of the cats that were hyperimmunized with CRFK cell lysates developed interstitial nephritis, and mild interstitial inflammation was present in some cats before inoculation. In an epidemiologic study of feline CKD, the development of CKD was linked to vaccination frequency. 70 Speculatively, the inflammatory response to rupture of tubular cells, whether from apoptosis, senescence, toxicity, or ischemia, might be more severe in vaccinated cats. While vaccination could be an initiation (or progression) factor for CKD in cats, further studies are needed.
In cats, stress has been linked to diseases of the skin 3 as well as the gastrointestinal, 177 respiratory, 187 and urinary 44,45,198 systems. Confinement, cofeeding, litterbox sharing, and cohabitation with other animals (eg, cats, dogs, people) have been variously suggested as causes of stress for domesticated cats. The loss of predictability and control of its environment might lead to chronic overactivation of a cat’s sympathetic nervous system and hypothalamic-pituitary-adrenal axis. 3,198 The prevalence of CKD in captive, but not free-ranging, cheetahs 19,149,150 could in part reflect a similar effect of environmental stress.
Potential Causes of Renal Hypoxia in Cats
The morphologic sequelae of an experimental ischemic insult 171 mirrors the typical appearance of CKD in cats, suggesting that renal hypoxia could be an initiation factor in cats. This is consistent with the view in other species that AKI can serve as an initiator of CKD. It is thought provoking to speculate about the potential causes of renal hypoxia in cats. A variety of host factors and conditions could contribute to acute or chronic bouts of renal hypoxia in aging cats (Fig. 16):
Stress and overactivation of the sympathetic nervous system
Aging
Tubular hypermetabolism causing relative ischemia (high tubular metabolic activity exceeding delivery of oxygen)
Anemia
Transient insults to renal hemodynamics, such as episodes of systemic hypotension, sympathetic nervous system overactivity, or activation of the renin-angiotensin-aldosterone system
Subclinical exposure to compounds with effects on the renal vasculature or tubular epithelium (eg, nonsteroidal anti-inflammatory drugs or melamine)
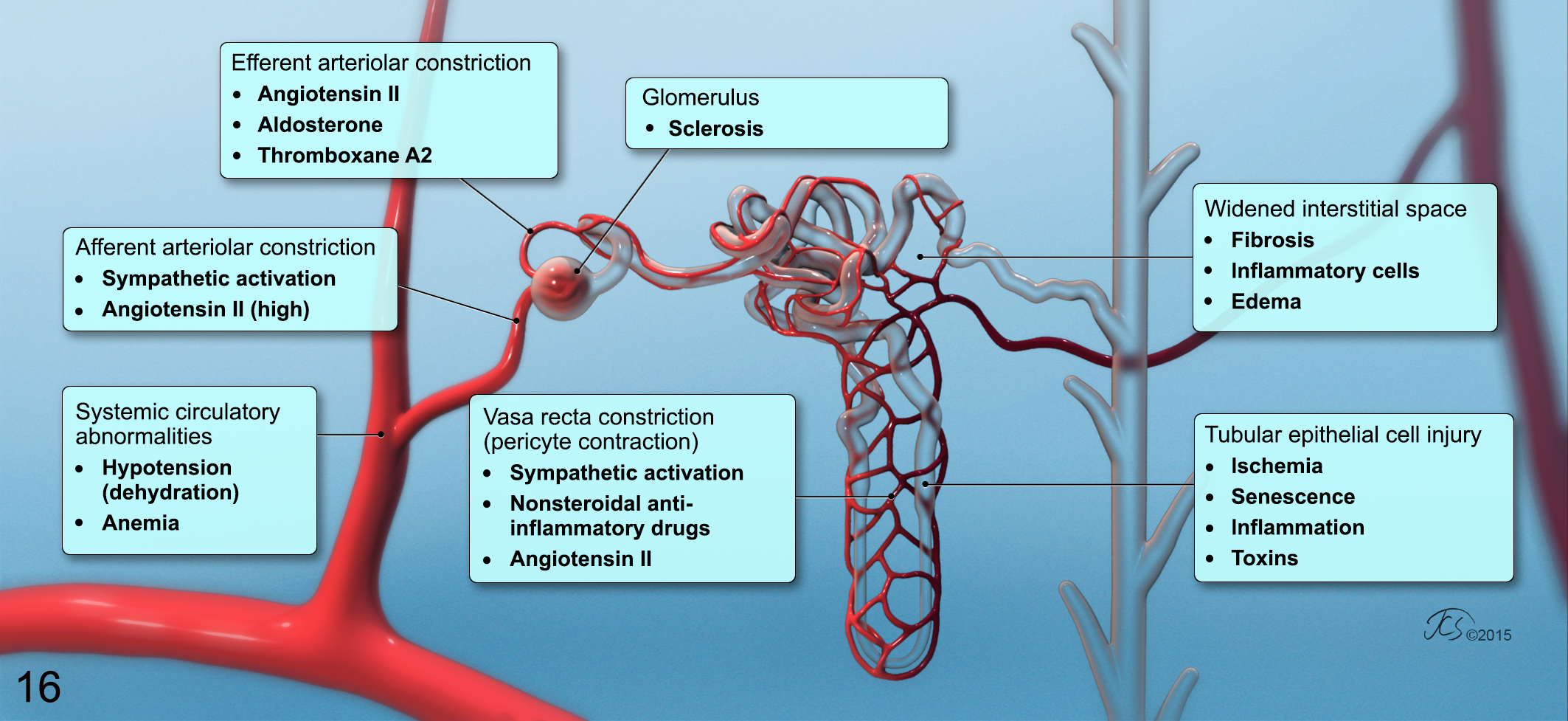
Environmental stress associated with chronic overactivation of the sympathetic nervous system could contribute to renal injury in cats by several mechanisms. Since renal sympathetic stimulation constricts the afferent arterioles of nephrons in other species 51,78 and reduces the flow within the descending vasa recta by inducing contraction of pericytes that encircle these vessels, 56 increased sympathetic system activity would be expected to produce reductions in renal blood flow, particularly in the medulla. Concurrent dehydration and activation of the sympathetic nervous and renin-angiotensin-aldosterone systems synergistically compromise the renal microcirculation in rats 116 due in part to pericyte-mediated constriction of the vasa recta capillaries (induced by angiotensin II and catecholamines) 56 but also due to arteriolar constriction mediated by angiotensin II 36 and aldosterone. 121 The presence of other vasoconstrictors, such as thromboxane A2 or endothelin, 46 could augment this vasoconstriction, leading to segmental tubular hypoxia. This may be relevant to the initiation (and progression) of CKD in cats, since dehydration 159 and stress are common findings in aged cats, particularly those with CKD. Other stress-associated changes could have an impact on renal perfusion. For example, stress-associated activation of the sympathetic nervous system contributes to blood pressure variability in people. 86 Changes in feline blood pressure associated with the environmental stress of a simulated visit to a veterinary clinic included transient bouts of marked hypertension and hypotension. 13 Although a role for primary hypertension as an initiator of CKD in cats remains tenuous, cats were shown to have particularly labile systemic arterial blood pressure, 13,42,163,188 with the observed changes in blood pressure patterns persisting as long as several months after a psychosocial stress regimen in cats.
The study linking hypoxia to chronic tubulointerstitial changes in feline kidneys 171 was conducted in young adult cats. A number of the changes associated with aging discussed above, including mitochondrial dysfunction, cellular senescence, increased oxidative stress, and reduction in Klotho gene expression, would be expected to either enhance the likelihood or worsen the consequences of hypoxia in the kidneys of aging cats. Aging aggravates the magnitude of renal injury from ischemic episodes in rats. 206 If aging similarly predisposes feline kidneys to hypoxic injury, particularly to normotensive renal ischemia as hypothesized to be the case in people, 196 then renal hypoxia could be an important initiator of CKD in cats.
In certain settings, such as the glomerulopenia of aging, the metabolic demands on tubular cells are increased. This so-called tubular hypermetabolism is believed to produce cellular injury by a variety of mechanisms, including oxygen free radical generation. 93,174 The restriction of dietary intake of some nutrients, including phosphorus, 93 diminishes the metabolic activity of tubular cells and lessens renal damage in rats. 93 Plasma phosphorus concentration at the time of diagnosis of CKD is positively associated with progression of IRIS CKD stage 3 in cats, 48 and efforts to control hyperphosphatemia are renoprotective in the remnant kidney model in cats 166 and in spontaneous feline CKD. 66 In the remnant kidney model of feline CKD, phosphorus overload induces changes similar to those observed in spontaneous feline CKD, specifically tubulointerstitial fibrosis, mononuclear infiltrates, and nephrocalcinosis. 166 The mechanisms contributing to these changes are poorly understood, but tubular hypermetabolism and hypoxia from relative tubular ischemia could be factors in this injury. Furthermore, if a “normal” aspect of aging in cats is loss of nephrons, 126 then the resultant interstitial inflammation, edema, and/or fibrosis could expand the interstitial space, limiting oxygen delivery to remaining nephrons. If senescent nephrons are prone to the development of glomerulosclerosis, then the postglomerular segments of affected nephrons would be expected to become hypoxic. This injury could be exacerbated by transient, subclinical exposure to nephrotoxins (eg, melamine or nephrotoxic antibiotics) or by inflammation induced by feline vaccines. 125
In established feline CKD, anemia that is primarily attributable to decreased erythropoietin production develops in 30% to 65% of affected cats. 49 Consistent with the hypothesis that feline kidneys are susceptible to hypoxic injury, the presence of this low red cell mass is a predictor of progression of CKD in cats. Age-associated changes in red cell mass are incompletely characterized in cats, but anemia is a common problem in elderly human beings 144 and, if present, would be expected to predispose aging cats to renal hypoxia. In cats with anemia, other systemic disturbances, such as dehydration or systemic hypotension, would be expected to synergistically affect renal tubular epithelium. This would be especially true for certain medullary segments of the nephron (S3 and medullary thick ascending limb), as these tubular segments are metabolically active but reside in a comparatively hypoxic region, even in normal kidneys. 156
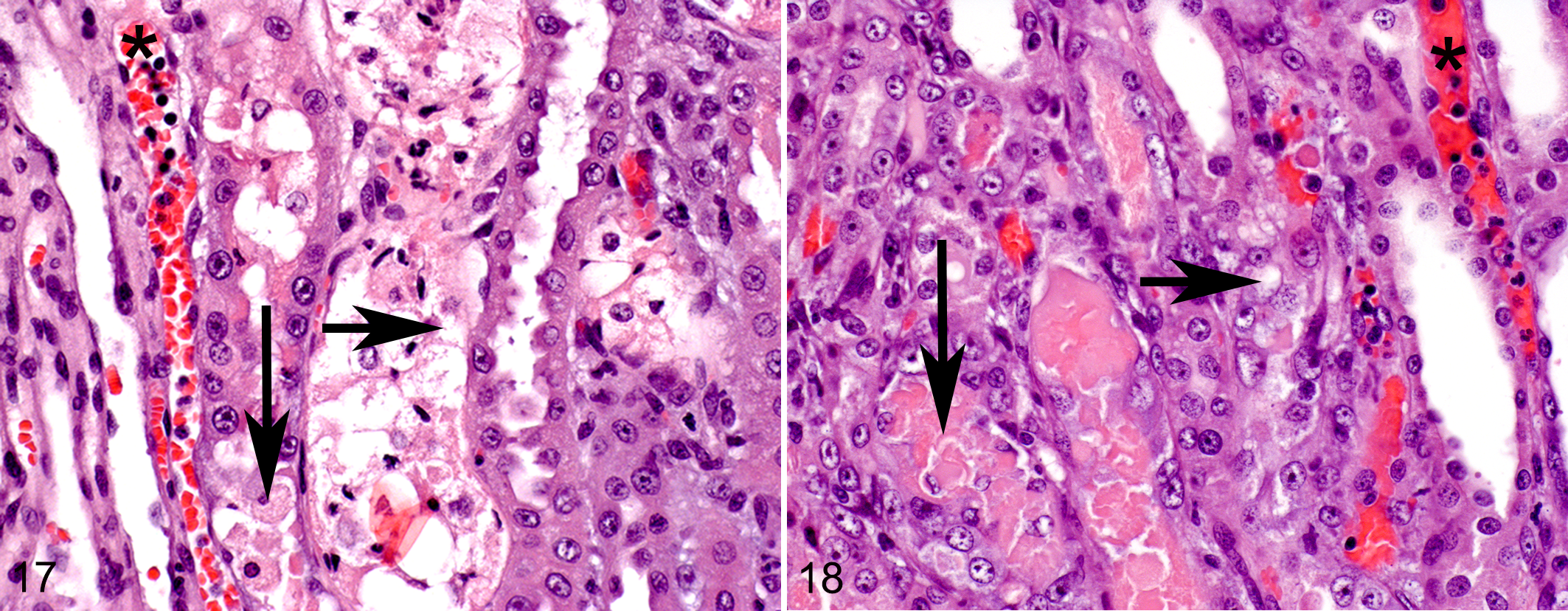
The control of the renal vasculature is complex. As noted above, acute hypoxic insults to the kidneys could result from imbalances between intrarenal vasodilatory and vasoconstrictive factors, as is suspected to be the case in cats with nephrotoxicosis from nonsteroidal anti-inflammatory drugs (NSAIDs). 97 Inhibition of cyclooxygenase enzymes within the kidney is thought to decrease the production of vasodilatory prostanoids, which normally help to maintain renal blood flow in the face of vasoconstrictors. 112 In particular, both cortical and medullary blood flow can be reduced by the administration of NSAIDs, 85 and NSAID-induced nephropathy is characterized by papillary necrosis and interstitial nephritis. Acute tubular injury from NSAID-induced nephropathy is similar to that seen in cats with an experimental ischemic insult of the kidney (Figs. 17, 18), involving the S3 portion of the proximal tubules. 16 In domesticated cats, factors that alter the control of renal hemodynamics, such as NSAID administration, are often coupled with stressful events, such as painful stimuli or hospitalization, which activate the sympathetic nervous system. Affected cats may be dehydrated or hypotensive, which would increase systemic and intrarenal generation of angiotensin II with its effects to constrict the efferent arteriole and vasa recta pericytes. Such combinations would be expected to result in medullary hypoxia and tubular injury. As there are no clinical indices for the direct detection of medullary injury, the importance of these types of interactions in the initiation (and progression) of feline CKD are speculative but deserve further attention.
Progression Factors in Feline CKD
Based on laboratory studies in rats 27 and dogs 37 and clinical studies in people 57,95 and dogs, 98 –100 it has been assumed that feline CKD is an inherently progressive disease. However, it is difficult to demonstrate progressive deterioration of renal function (GFR) in laboratory models of feline CKD. 73,166 Similarly, analysis of serial measurements of serum creatinine concentration demonstrate that spontaneous feline CKD is often slowly progressive or nonprogressive, 48 although this is highly variable. While some cats with spontaneous CKD progress more rapidly, these cases are more difficult to study. Despite the absence of specific therapeutic interventions, a large proportion of cats with CKD (53%) did not exhibit progressive increases in serum creatinine concentration in 1 year. 48 Upon necropsy evaluation, cats without readily identifiable causes for their CKD tend to be older, suggesting that idiopathic CKD is often a slowly progressive or nonprogressive disease. 47
Beyond persistence of an initiating primary renal disease, a number of additional factors have been implicated in the progressive decrements of GFR observed in CKD in a variety of species.
38,110
In these other species, progression factors (Fig. 11) operate independently of the primary disease, are activated by adaptive changes in the animal or through secondary effects of reduced renal function, and are held to be responsible for what is commonly termed inherent or intrinsic progression of CKD.
38
Several factors have been associated with progression of feline CKD: Phosphorus intake Proteinuria Anemia Systemic hypertension Intraglomerular hypertension Activation of the renin-angiotensin-aldosterone system Sodium intake Tubular hypoxia
Progression or mortality in cats with CKD is associated with some of the implicated factors, including disorders of phosphorus homeostasis, 48,64,81,82 proteinuria, 48,67,183,184 and anemia. 48 In cats in IRIS stages 2 and 3, a number of dietary manipulations, including phosphorus restriction, reduced the incidence of uremic episodes and renal-related deaths. 167
As noted previously, systemic hypertension is observed in many cats with CKD 15,65,182 and is associated with the development of target-organ injury,* proteinuria, 105,184 and azotemia 104 in cats. Because the risk of high blood pressure to target organs in cats has been recognized for >2 decades, 129 placebo-controlled clinical trials of the effects of hypertension on progression of feline CKD are difficult to design. As a consequence, the importance of hypertension as a progression (or initiation) factor in feline CKD is uncertain.
Intrarenal hemodynamic changes that may contribute to progression have been studied in cats. Based on micropuncture studies in a model of feline CKD, glomerular capillary hypertension and glomerular hyperfiltration develop as adaptive changes in response to reductions in renal function or nephron loss. 33,36 These hemodynamic changes are arguably a maladaptation 32,94 that contributes to proteinuria in cats. 33 Studies in uninephrectomized aged dogs 74 and in older human kidney donors 186 demonstrate that aged kidneys exhibit adaptive hyperfiltration and renocortical hypertrophy. Thus, if nephron loss occurs as a general phenomenon in aging cats or as a consequence of other insults, it is likely that these same maladaptive intraglomerular changes would occur in remnant feline nephrons, and if so, these alterations could contribute to future decrements in renal function. In other species, there is evidence that glomerular hypertension and proteinuria lead to damage to the kidneys through nephron destruction. In particular, inhibitors of the renin-angiotensin system, which would be expected to reduce intraglomerular pressure and proteinuria, seem to be renoprotective in dogs 39,43,80,87 and people. 101,192 Micropuncture studies demonstrate that inhibition of angiotensin-converting enzyme lowers intraglomerular pressure in remnant feline nephrons, 36 and this approach reduces proteinuria in cats with spontaneous CKD. 113 However, it was not possible to demonstrate an overall beneficial effect on survival or renal function in the latter study. 113 While increased plasma aldosterone concentrations have been documented in cats with CKD, plasma renin activity is usually either normal or low. 103,106 Unlike dogs, there was no relation between intrarenal expression of renin and angiotensin II and interstitial fibrosis in cats. 147 Although secondary hyperaldosteronism remains of interest, it may be that the systemic and intrarenal renin-angiotensin systems and changes in glomerular blood pressure are less important in feline CKD than in the CKD of other species. Interestingly, high-sodium diets have been associated with an enhanced rate of CKD progression 114 but in long-term trials (2 years) had no adverse effects on blood pressure 53 or renal function 164 in normal cats.
In cats with reduced renal mass, there is marked and preferential dilation of the afferent arterioles, 41 which is responsible for the glomerular hypertension and hyperfiltration observed in remnant nephrons. Given the large increase in tubular oxygen demands associated with processing this large filtered load per nephron, 41 it has been suggested that intermittent tubular hypoxia and oxidative injury may be present in affected people. 174 Evidence suggests that antioxidants delay progression in people with predialysis CKD 108 and in a laboratory model of CKD in dogs. 31 There is evidence of altered antioxidant status in cats with CKD 111,120 and a beneficial systemic effect of antioxidants, 209 which would support the hypothesis that relative, or absolute, hypoxia plays a role in the progression of feline CKD.
Interstitial Fibrosis: Friend or Foe
Interstitial fibrosis is present in early feline CKD and becomes more severe with advancing disease, 47,143 suggesting that renal fibrosis is important in the progression of feline CKD. However, this fibrosis is generally viewed as occurring secondary to injury, not as a primary event. Many of the factors implicated in progression of CKD in cats—including proteinuria, systemic hypertension, chronic inflammation, anemia, hypoxia, aging, and hyperphosphatemia—are viewed as promoters of fibrosis. 127 In other species, renal injury is marked by elevated levels of the phosphaturic hormone, fibroblast growth factor 23, and a deficiency of its coreceptor, Klotho. 92,155 These changes promote renal fibrosis. 128 Elevated fibroblast growth factor 23 levels predict the development of azotemia in geriatric cats 71 and the likelihood of progression and mortality in cats with azotemic CKD. 81 It seems likely that this axis contributes to the progression of renal injury and fibrosis in established CKD in cats, but it is unclear whether this axis plays a role in the initiation of renal injury in this species.
The characterization and origin of the cells that produce interstitial fibrosis have been extensively studied. These cells—referred to as myofibroblasts based on smooth muscle actin expression and fibroblastic morphology—are derived primarily from activation of resident interstitial fibroblasts. Other plausible precursors of myofibroblasts include circulating bone marrow–derived cells or, rarely, transdifferentiation from epithelial or endothelial cells. 134 Epithelial-mesenchymal transdifferentiation is a proposed mechanism whereby tubular epithelial cells transform into mesenchymal cells, migrate into the interstitium, and produce collagen. While this transition is found in the context of embryonic development and in adult cancer cells associated with tumor invasion and metastasis, there are conflicting data concerning its existence in vivo, and if present at all, the contribution of this transdifferentiation to fibrosis is almost certainly less significant than previously thought. 134 In the normal kidney, interstitial fibroblasts play a crucial role in homeostasis of the extracellular matrix through the production of matrix and matrix-degrading proteases. 127
Regardless of the origin of myofibroblasts in the feline kidney, increased interstitial connective tissue certainly could contribute to renal injury. In the kidneys, residual peritubular fibrosis can disrupt the close association between interstitial capillaries and tubules, leading to tubular ischemia and tubular atrophy (Figs. 14, 15). Thus, fibrosis as a cause of ischemia could contribute to progression of feline CKD. As noted above, if nephron senescence is a normal part of aging in cats, 126 then the resultant fibrosis could act as an initiator of progressive CKD by contributing to regional tubular hypoxia. However, the presumption that renal fibrosis is universally detrimental is likely an oversimplification. Following an acute insult, for example, the course of renal fibrosis can be divided into multiple phases, with varying implications for intervention. 134 In particular, early after renal damage, fibrosis might play a beneficial role in repair by providing structural integrity to injured tubules during regeneration. Defining the role of renal fibrosis in inducing hypoxic renal injury and/or progression of CKD in cats requires further study.
Future Directions
Many, perhaps most, aged cats exhibit clinical or pathologic evidence of CKD. The pathologic changes observed in the kidneys of cats with CKD suggest that nephron loss, inflammation, and fibrosis are important features of this disease. A number of factors have been implicated in progression of established CKD in cats, including hyperphosphatemia, proteinuria, anemia, systemic hypertension, aging, and tissue hypoxia. Unfortunately, except for hypoxia and aging, there is a paucity of direct evidence to suggest that these progression factors play a role as an initiator of CKD in this species. Instead, the primary causes of this disease, the initiators, remain unknown or hypothetical (eg, aging and renal hypoxia). Solving this mystery will require studies that define the cellular and molecular events that contribute to tubular cell death, intrarenal inflammation, and interstitial fibrosis in cats.
Footnotes
Notes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.