
Abstract
Two horses euthanized for neurologic deficits were diagnosed with hamartomatous myelodysplasia of the spinal cord. One was a 5-week-old Holsteiner colt exhibiting spasms of muscle rigidity in the extensor muscles of the limbs and epaxial muscles, and the other was a 3-year-old Thoroughbred colt exhibiting progressive ataxia and hypermetria in the pelvic limbs. Each had focal disorganization of the white and gray matter of the spinal cord forming a mass interspersed with neurons, glial cells, and disoriented axon bundles. In the Holsteiner colt, the mass was at the level of C5 and included islands of meningeal tissue contiguous with the leptomeninges. The mass occluded the central canal forming hydromyelia cranial to the occlusion. In the Thoroughbred colt, the mass was at the level of L1 on the dorsal periphery of the spinal cord and did not involve the central canal.
Congenital defects of the central nervous system are rarely reported in horses. Most of these lesions have been reported as syringomyelia or syringohydromyelia. 3,5,7 However, 1 text reported a single case of “combined hamartoma and myelodysplasia” as an incidental finding in the thoracic spinal cord (T6–T8) of a foal with no neurologic deficits. 8 We herein report 2 cases of similar hamartomatous myelodysplasia in horses euthanized for clinical neurologic signs, suggesting that this is a rare, unique lesion seen in horses with widely variable clinical presentation.
Case 1
A 5-week-old Holsteiner colt was presented to the University of Florida Veterinary Teaching Hospital for muscle rigidity and spasms. The colt was born with premature placental separation at delivery and had been slow to suckle. Initially the colt was stiff in all limbs and exhibited progressive difficulty in becoming recumbent. The colt developed extensor muscle rigidity particularly in the proximal thoracic and pelvic limb muscles, epaxial muscles, and strap muscles of the neck. Severe muscle spasms could be induced by stimulation (ie, handling, loud noise, bright light, menace response tests) causing lordosis and extension of the limbs and leading the colt to fall over backward. Such spasms could last >20 seconds. Mentation was appropriate, and electromyography showed no abnormalities. An electroencephalogram suggested abnormal discharges. While muscle spasms were initially responsive to phenobarbital treatment, repeated increases in the dose were necessary, and clinical response diminished. Based on progression and quality-of-life concerns, the colt was euthanized.
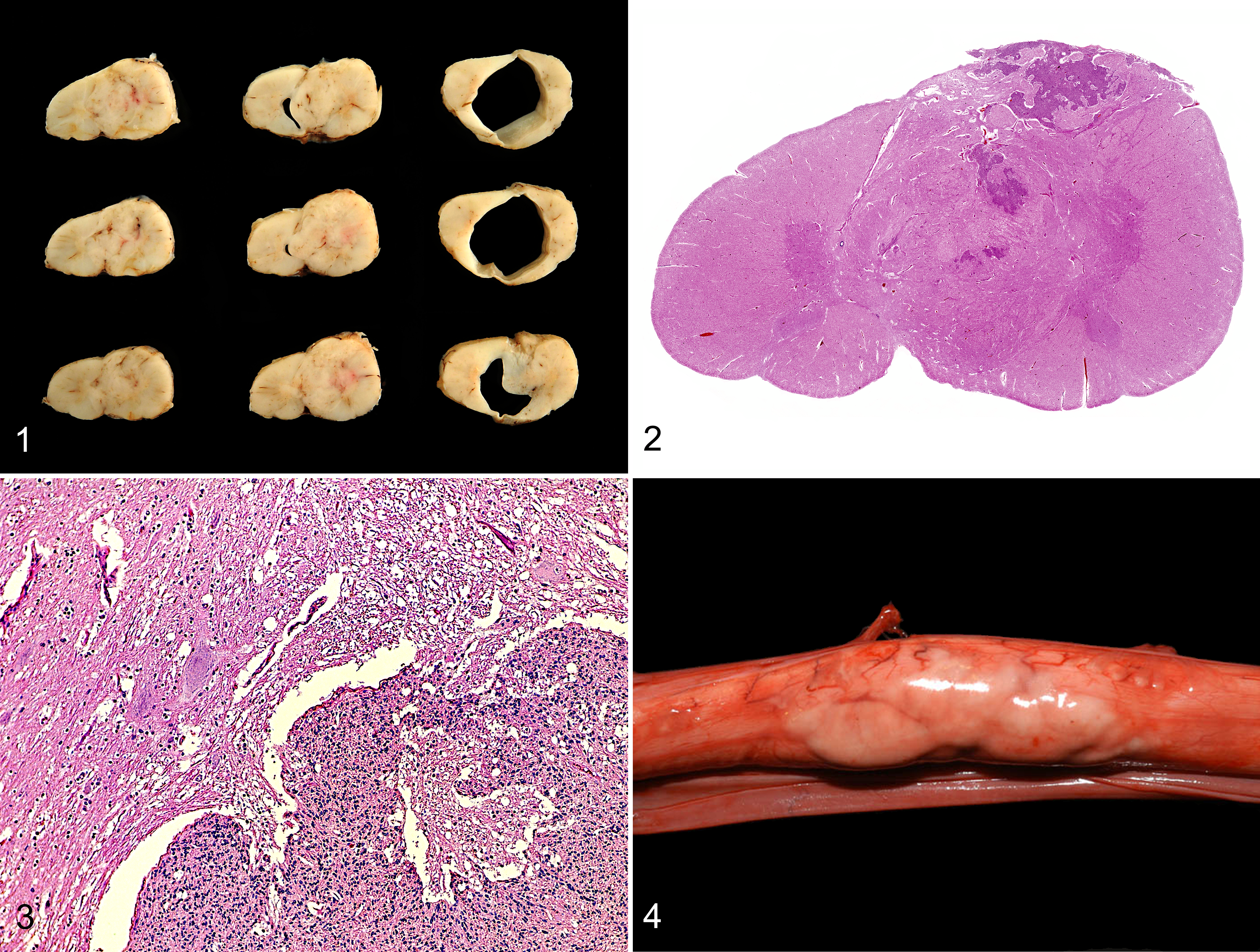
Postmortem examination revealed, at the level of the fifth cervical vertebra (C5), a 4.5-cm-long fluctuant dilation of the spinal cord, which was 2.9-cm diameter at the widest and was filled with cerebrospinal fluid. On section, the dilated area was cavitated with a smooth and glistening internal surface, and the white matter was markedly thin. At the caudal end of the dilation, there was a mass composed of relatively normal-appearing but redundant spinal cord tissue extending from the dorsolateral region of the spinal cord ventromedially separating the horns of the gray matter and completely occluding the central canal (Fig. 1). The mass was firmly adhered to the overlying dura mater. A smaller, 1-cm-long soft region of the spinal cord was also noted at the level of C4, which on section was shown to be a small round cavitation in the white matter dorsal to the central canal. Histologically, the spinal cord dilation at C5 was a marked dilation of the central canal with compression and vacuolation of the immediately surrounding gray and white matter. The mass was composed of 3 tissue types haphazardly intermixed (Figs. 2, 3). The most prominent tissue—which largely extended from the dorsolateral surface of the spinal cord and was contiguous with the leptomeninges—was markedly cellular with spindle-shaped and stellate cells forming random streams and bundles. Tortuously intermixed with this tissue was gray and white matter with haphazardly arranged prominent axons forming crisscross patterns among prominent and redundant vasculature and randomly scattered neurons and glial cells. No mitotic figures were seen. The cavitations cranial to the mass and at C4 were partially lined by variably attenuated ependymal cells. Focally, there was a narrow defect in the dorsal wall of the central canal, which appeared to be contiguous with the C4 cystic space (syringohydromyelia).
Case 2
A 3-year-old Thoroughbred colt presented for ataxia after training. On neurologic examination, the colt exhibited ataxia in both pelvic limbs and the left thoracic limb. Moreover, both pelvic limbs exhibited hypermetria, which was slightly more prominent in the right pelvic limb. When backing, the left thoracic limb would drag along the ground before flexing. Mentation was appropriate. Despite treatment for equine protozoal myeloencephalitis, the ataxia progressively worsened. The colt was eventually deemed dangerous and was euthanized.
Postmortem examination revealed, at the level of L1, a multinodular tan mass (3 × 1 × 0.7 cm) protruding from the left dorsal surface of the spinal cord (Fig. 4). On section, the mass mildly compressed surrounding spinal cord parenchyma but did not extend to the central canal (Suppl. Fig. 1). Histologically, the mass was composed mostly of disarranged white matter with large disoriented bundles of axons but contained a few islands of gray matter on the periphery, in which were interspersed numerous neurons and glial cells. No mitotic figures were seen. Within the immediately adjacent compressed gray matter, there were a small number of shrunken hypereosinophilic neurons. No abnormalities were noted in the central canal. There was also no evidence of equine protozoal myeloencephalitis.
In case 1, the clinically noted muscle rigidity and spasms may be a manifestation of spastic hypertonia, which is occasionally seen in spinal cord injury in humans, and the cervical location of the spinal mass is consistent with this. In case 2, however, while the hypermetria in the hind limbs may be explained by the lumbar mass, the toe dragging of the left thoracic limb is unexpected. It is possible that a second lesion either related or unrelated was missed at the time of necropsy.
A previous report documented a spinal cord lesion similar to that seen in case 1. 8 During postmortem examination of a foal with no reported neurologic deficits, the authors found in the spinal cord at T6–T8 an enlargement that was characterized by a fluctuant syrinx and a firm portion that was composed of “disorganized spinal cord parenchyma.” A second report described syringomyelia at C7–T7 in a 6-month-old Thoroughbred foal euthanized due to abnormal posture with a wide-based stance and gait, which included pelvic limb hopping and difficulty turning to either side. 3 At T6–T8, the caudal-most aspect of the lesion, there was reported to be a mass effect created by “disorderly arrangement of white and grey matter,” and the gray matter reportedly extended to the external surface of the spinal cord, blending into the meninges. The authors briefly refer to this lesion as myelodysplasia. While the second report emphasized the syringomyelia, 3 we believe that these 2 previously published cases describe a similar lesion to those that we describe above for cases 1 and 2.
While syringohydromyelia and a congenital intra- and extraspinal cyst have also been reported in a number of other horses (ranging from 6 days to 8 years old), there is no discussion of disorganized spinal cord tissue forming a mass effect in these cases. 4,5,7 Therefore, it is not clear whether the lesions seen in these cases are similar or different.
Given the absence of syringomyelia or hydromyelia in case 2, in which there was no compression of the central canal, we suspect that the cerebrospinal fluid-filled spaces seen in case 1 and the previously described cases 3,8 may be secondary to the focal deformity of the spinal cord. Based on the previous description, 8 we herein refer to this deformity, characterized by disorganization of spinal cord tissue and occasionally meningeal tissue forming a mass, as hamartomatous myelodysplasia. This is also to differentiate it from the midline spinal cord hamartoma, a rare and often congenital and asymptomatic lesion seen in humans, which is composed of a wide array of different tissues, including nerves, adipose, muscle, cartilage, bone, blood vessels, glands, and urothelium. 2,6 Given similar gross and histologic findings in the 4 cases of horses, each ≤3 years old, we suspect that this is a rare and unique congenital lesion with a wide range of locations along the spinal cord and markedly variable clinical presentation.
Footnotes
Acknowledgements
We thank Dr Luis Benitez of Teigland, Franklin & Brokken for referral of cases to the University of Florida Large Animal Hospital and Dr Claus Buergelt, emeritus faculty of the University of Florida Department of Infectious Diseases and Pathology, for case consultation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.