
Abstract
Cartilaginous tumors of the larynx and trachea are uncommon in the dog. The authors describe 10 cases diagnosed between 1995 and 2014 and review 16 cases in the literature. Seven of our cases were tracheal and 3 were laryngeal. Two of the laryngeal tumors were chondromas, which have not been previously reported in this site. The third laryngeal tumor was a myxochondroma. Of the 7 tracheal tumors, 6 arose from the ventral tracheal wall, including 2 that were extraluminal. Tracheal tumor types included chondrosarcoma (n = 3), chondroma (n = 2), and osteochondroma (n = 2). All of the laryngeal tumors and 5 of 7 of the tracheal tumors occurred in adult dogs (aged 5–11 years). The 2 tracheal osteochondromas were in young dogs (3–4 months) and were intrathoracic, while the remaining tracheal tumors were cervical. Surgical excision had a good outcome in most cases. Combining our 10 cases with the 16 previously reported cases showed that 6 (27%) of the affected dogs were Arctic breeds (Alaskan Malamute or Siberian Husky) suggesting a predisposition in this type of dog.
Primary neoplastic disease of the larynx is rare in domestic animals. 29,31 The most common types of primary laryngeal tumors are squamous cell carcinoma, oncocytoma, and rhabdomyoma. 7,10,26,31 Mast cell tumor, 7,15,31 melanoma, 22,31 undifferentiated carcinoma, 7 leiomyoma, 20 rhabdomyosarcoma, 17 lipoma, 29 plasmacytoma, 16 granular cell tumor, 28 and osteosarcoma 5 have also been reported. Primary tracheal neoplasia is even more uncommon. Adenocarcinoma, 7 undifferentiated carcinoma, 18 plasmacytoma, 9 leiomyoma, 3 fibrosarcoma, 21 mast cell tumor, 7,15 rhabdomyosarcoma, 34 and osteosarcoma 5 have been reported.
Neoplastic disease of the cartilaginous component of the larynx and trachea are rare and described only in single-case reports or brief communications including a few cases. A total of 16 cases have been described in the dog in the veterinary literature in English language, among 13 publications.* Veterinary pathology textbooks describe them only briefly. 8,32 Myxochondroma and chondrosarcoma are the only cartilaginous neoplasms described in the larynx. Chondroma, osteochondroma, and chondrosarcoma have been reported in trachea. The present article describes the clinical and pathologic features of 10 additional cases and compares them to those previously reported.
Material and Methods
Our records were reviewed for dogs with a diagnosis of primary tracheal or laryngeal neoplasia. The search produced a series of 10 dogs with cartilaginous neoplasms diagnosed between 1995 and 2014. All cases had been fixed in 10% neutral buffered formalin, processed routinely, and embedded in paraffin wax. We confirmed histologic diagnoses by reexamination of archived specimens. Paraffin blocks were sectioned at 3 μm and stained with hematoxylin and eosin and with Alcian blue (pH 2.5 for acid mucopolysaccharides) for routine histopathologic study. When available, signalment, history, clinical signs, radiographic findings, response to treatment, and follow-up information were obtained through e-mail and telephone interviews with the referring clinicians.
A review of the peer-reviewed scientific literature was performed in the Medline database (National Library of Medicine, PubMed) and Google Scholar database up to September 2014 using different associations of the following keywords: cartilage, cartilaginous, neoplasia, tumor, trachea, tracheal, larynx, laryngeal, chondroma, osteochondroma, chondrosarcoma, dog, canine. The search was focused on the clinical, macroscopic, and histologic characteristics.
Results
Clinical Features
Ten cases of cartilaginous tumors were included in the study and are summarized in table 1.
Signalment, Tumor Type, Clinical Features, Treatment, and Follow-up for 10 Dogs With Tracheal or Laryngeal Tumors.
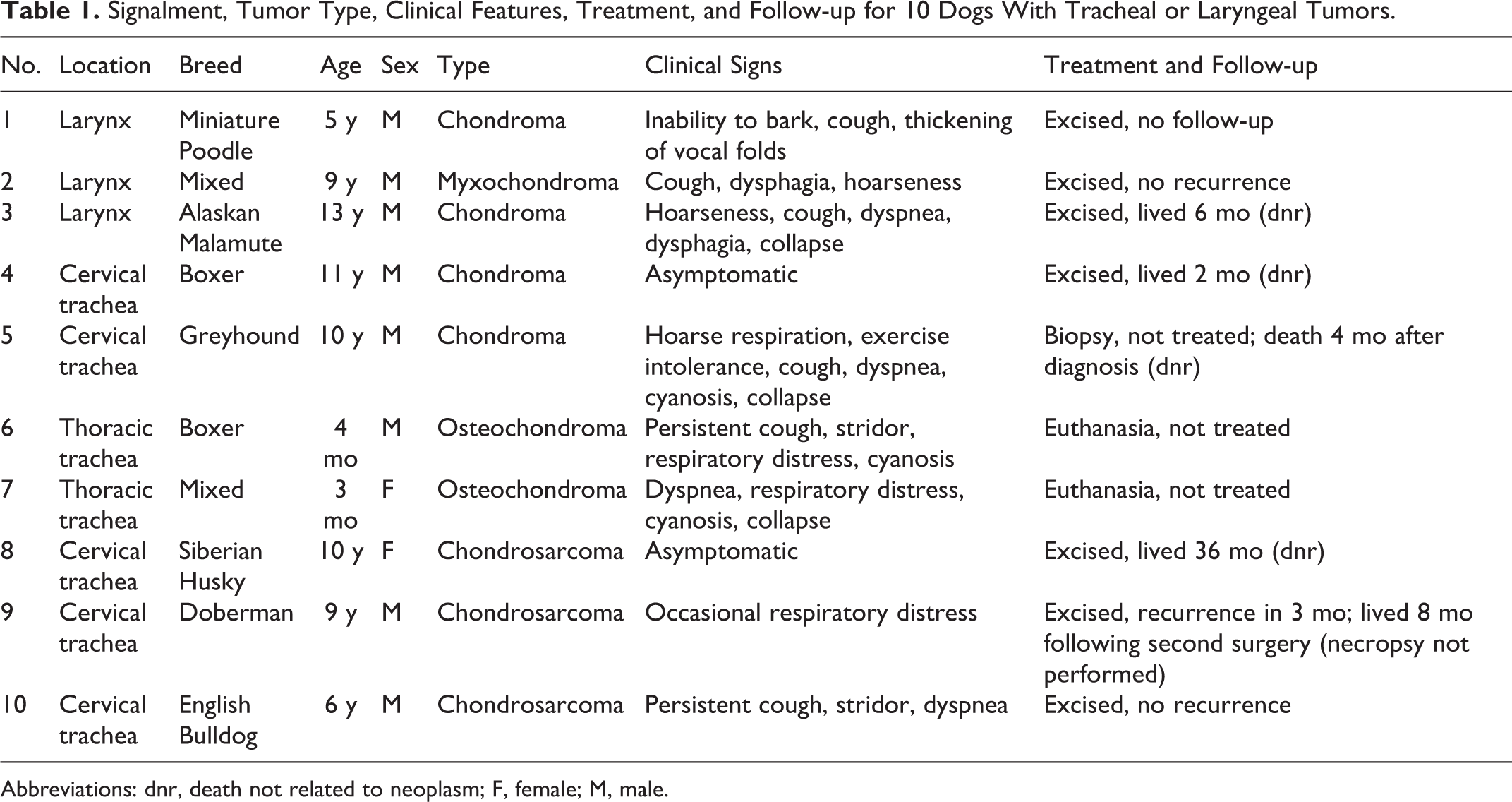
Abbreviations: dnr, death not related to neoplasm; F, female; M, male.
Three of 10 cases in our series had laryngeal tumors. All were benign and had been diagnosed as chondromas. After reexamination, case No. 2 was reclassified as myxochondroma based on histologic features. The ages of the 3 dogs were 5, 9, and 13 years. All 3 were males. The most frequent clinical sign was persistent cough. Other signs included hoarseness, inability to bark associated with thickening of vocal folds, and variable grades of dysphagia. Case No. 3 was the largest lesion in the series (1.5 cm in diameter) and caused dyspnea, respiratory distress, and occasional collapse. The lesions were confined caudally to epiglottis and were covered by mucosa. Complete blood count and biochemical analyses were normal in the 2 cases in which they were performed. Radiographs were obtained only for case No. 3, which showed a single, well-circumscribed nodule arising from the ventral larynx. There was no perilaryngeal tissue involvement. Surgical resection of all 3 lesions was performed with an uneventful recovery for case Nos. 2 and 3; follow-up information was not available for case No. 1.
Seven of 10 cases were tracheal tumors and presented either as extraluminal growths infiltrating cervical soft tissues (n = 2) or as intraluminal masses (n = 5). The extraluminal growths included 1 chondroma and 1 chondrosarcoma. Intraluminal tumors included 1 chondroma, 2 osteochondromas, and 2 chondrosarcomas. Both osteochondromas occurred in young dogs (3 and 4 months of age). The mean age of the remaining patients with tracheal tumors was 9.2 years. Five of 7 dogs were male. The most common clinical signs were dyspnea, cough, respiratory distress, and cyanosis. Occasionally, syncope was reported. The 2 patients with extraluminal masses were asymptomatic and were presented for a palpable growth in the neck. Intraluminal growths were not visible or palpable externally. Six of 7 lesions arose from the ventral wall of the trachea. The complete blood count and serum biochemical parameters were within the reference intervals for the 4 cases in which they were performed. Radiographs were obtained in 3 patients (case Nos. 6, 7, 9). A distinct intratracheal mass containing mineralized foci and occupying two-thirds of the tracheal lumen in the carina characterized the lesions in case Nos. 6 and 7. Case No. 9 was an ill-defined extraluminal mass of cartilaginous appearance without evident mineralization. Tracheoscopy was done in 1 dog (case No. 10) and revealed multiple small polypoid growths protruding from the tracheal mucosa into the lumen. Surgical resection was performed in 4 cases. Three patients had an uneventful recovery. One chondrosarcoma (case No. 9) recurred 3 months later and required 2 surgical procedures to eradicate the disease. Two patients (case Nos. 6 and 7; both young dogs with intrathoracic osteochondromas) had no treatment and were euthanized because of poor prognosis. Metastases were not reported in any case.
Gross Pathology and Histopathologic Findings
Laryngeal Chondroma: Case Nos. 1 and 3
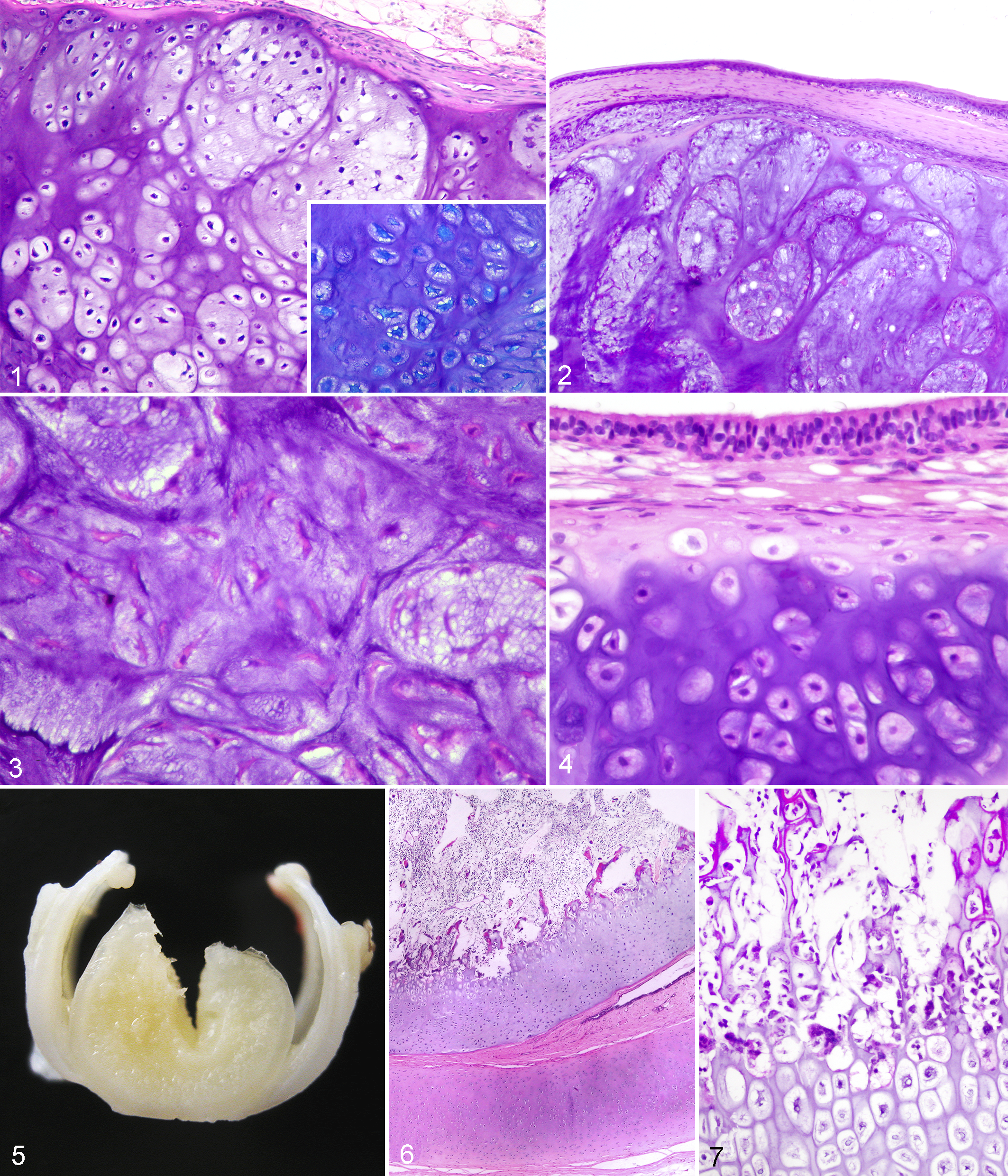
Grossly, lesions were firm to hard, blue-white to milk-white nodules (1 to 1.5 cm in diameter) with evenly contoured borders and covered by a thin fibrous capsule. Microscopic examination of these masses revealed a thin capsule of dense collagen overlying multiple irregular lobules of alcian blue–positive, normal-appearing hyaline cartilaginous tissue (Fig. 1). Case No. 3 had a fibrous stroma with small areas of loose organization. Cells in these lobules were uniform in size and shape and had small hyperchromatic nuclei. Anisokaryosis was minimal. No mitoses were seen.
Laryngeal Myxochondroma: Case No. 2
This was a roughly spherical mass 1 cm in diameter. Histologically, the lesion was characterized by a noncircumscribed, lobulated, variably cellular proliferation of fusiform to stellate cells with no atypia in a fibromyxoid background with areas showing distinct stromal basophilia and a chondroid appearance (Figs. 2, 3). Scattered foci of mineralization were within the matrix. Cartilaginous matrix was alcian blue positive. No mitoses were noted.
Tracheal Chondroma: Case Nos. 4 and 5
Case No. 4 was a firm, well-demarcated oval mass (3 × 2 × 2 cm) attached to the trachea. The small biopsies submitted for histopathologic examination consisted of fragments of hyaline cartilage composed of small, well-differentiated chondrocytes with no atypia. No mitoses were seen. Case No. 5 was a firm and slightly lobulated well-demarcated mass (1.5 × 1.7 cm). It was histologically composed of plump cartilage cells (Fig. 4) immersed within an alcian blue–positive cartilaginous matrix that was separated into lobules by indistinct fibrous connective tissue septa with no ossification or evidence of marrow cavity development.
Tracheal Osteochondroma: Case Nos. 6 and 7
These tumors were spherical masses measuring 1 cm in diameter that extended into the tracheal lumen from the ventral aspect of a tracheal ring and were attached by a wide base. Cut section of the masses revealed a bony central portion surrounded by a discontinuous outer zone of cartilage (Fig. 5). Microscopic examination showed that the tumors were located subjacent to the tracheal epithelium and consisted of a cap or outer zone of alcian blue–positive hyaline cartilage contiguous with the adjacent tracheal ring, with endochondral ossification forming the central bony tissue containing variable amounts of marrow elements (Figs. 6, 7). Cells in the cartilaginous component were small, with inconspicuous cytoplasm and small dark nuclei. No mitoses were noted.
Tracheal Chondrosarcoma: Case Nos. 8–10
Case Nos. 8 and 9 were firm to hard masses (2 and 4 cm in diameter, respectively) with a convoluted surface and indistinct borders. They were attached to the ventral wall of the trachea by a wide stalk. Growth was extraluminal for case No. 8 and intraluminal for case No. 9. On cut section, the tumors were composed of variably sized multiple nodules or lobules of translucent to grayish-white or shiny-gray appearance with small areas of gelatinous consistency. Microscopically, they were characterized by areas of interconnected lobules of alcian blue–positive hyaline cartilage divided by dense fibrous connective tissue with ill-defined foci of basophilic myxomatous matrix (Fig. 8). In these areas, lacunae usually contained single chondrocytes, but groups of 1–4 chondrocytes per lacuna were occasionally present. The cells were round to stellate and variable in size. Nuclei were round, variably sized, and often hyperchromatic, with a single nucleolus and coarse chromatin (Fig. 9). Mitotic index was low (0–2 mitoses/400×) in these areas. Other zones in the tumors were highly cellular and composed of round, plump, spindle, or stellate cells with large cytoplasmic processes and hyperchromatic large nuclei with marked anisokaryosis and frequent mitoses (2–4 mitoses/400×; Fig. 10). Nuclear pleomorphism and bi- or multinucleated giant cells were also noted. Small random foci of coagulation necrosis were also present. Small foci of mineralization were present in case No. 8. No evidence of vascular invasion was observed in the histologic sections.
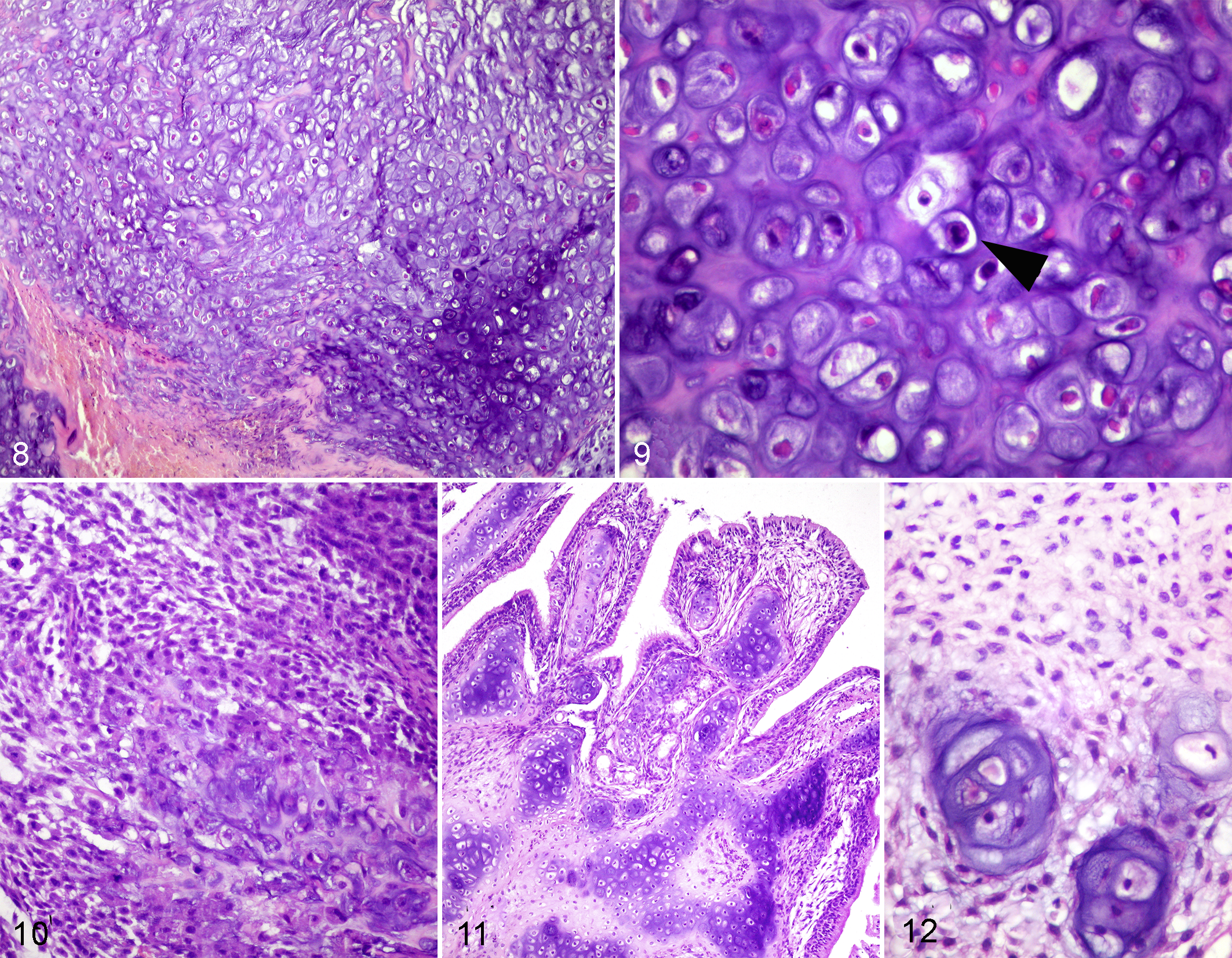
Case No. 10 consisted of multiple irregularly shaped, firm polypoid formations (0.2–1 cm) growing into the tracheal lumen. They were composed of soft to moderately firm tissue with small foci of white cartilage. Histologically, areas of moderately cellular sarcomatous tissue composed of spindle to stellate cells with moderate anisokaryosis alternated with areas of basophilic and alcian blue–positive cartilaginous tissue composed of round or stellate cells with small hyperchromatic nuclei with low atypia (Figs. 11, 12). Mitotic figures were rarely detected (0–1 mitosis/400×).
Discussion
The types of tracheal and laryngeal cartilaginous tumors identified in our series were similar to those reported previously (Table 2). In addition, 2 laryngeal chondromas were identified in our case series.
Tracheal and Laryngeal Cartilaginous Tumours Previously Reported in the Dog (n = 16).
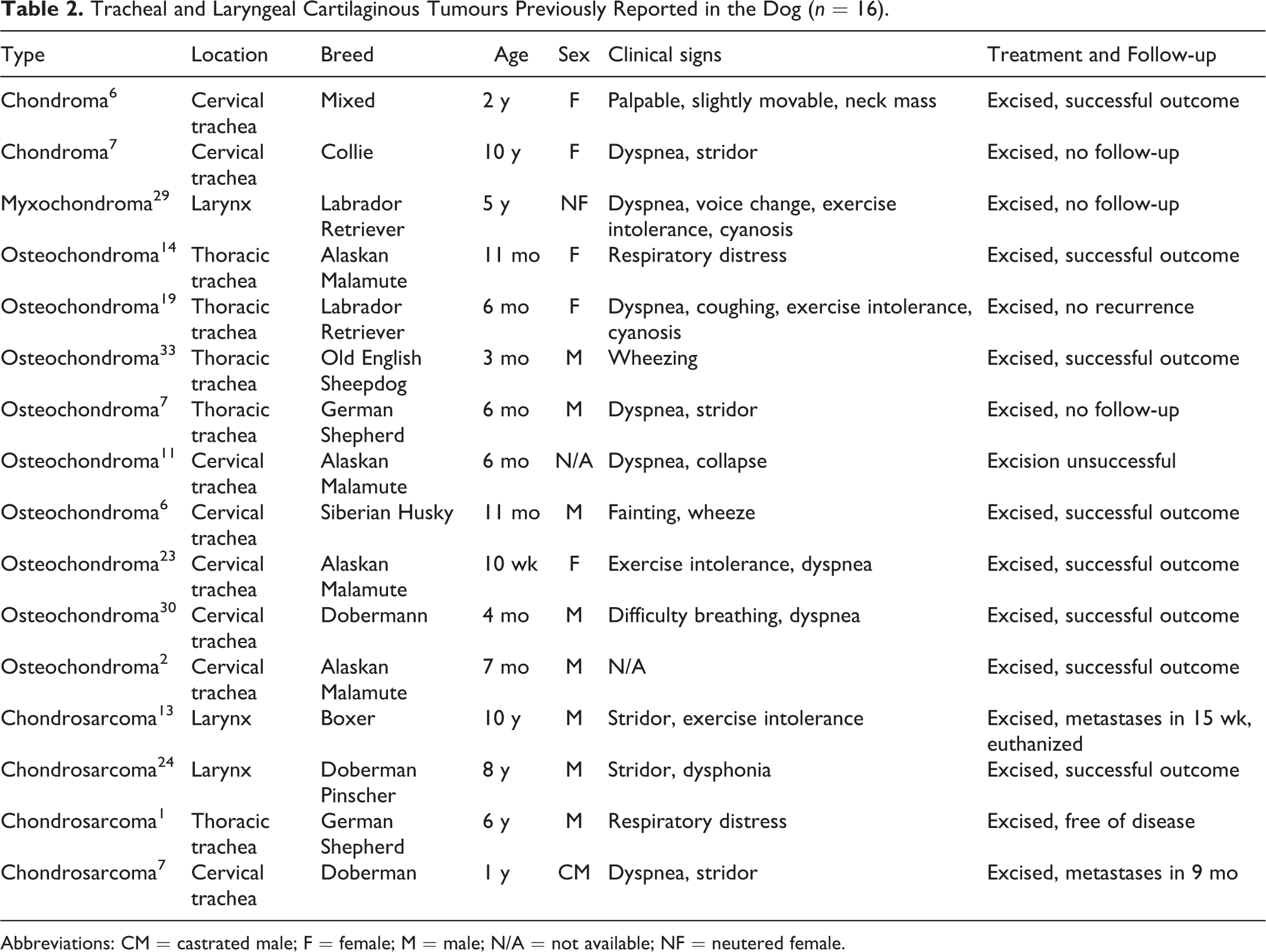
Abbreviations: CM = castrated male; F = female; M = male; N/A = not available; NF = neutered female.
Considering the 16 cases reported in the literature and the 10 cases described herein, there have been 26 primary cartilaginous tumors of the larynx and trachea reported in the dog. † Tracheal tumors appear to be more common than laryngeal tumors (20 vs 6), and benign forms are more frequently found than malignant forms (19 vs 7; Tables 1, 2). Tracheal osteochondroma is the most frequent cartilaginous neoplasm reported, representing 42.3% of all tumors described, followed by tracheal chondrosarcoma (19.2%), tracheal chondroma (15.4%), laryngeal chondroma (7.7%), laryngeal myxochondroma (7.7%), and laryngeal chondrosarcoma (7.7%). The ages of affected animals in our series were very similar to those previously reported in the literature. 6,7 Osteochondromas occur in younger dogs (10 weeks to 11 months), and all other types of tumor occur in adult dogs. Clear sexual predisposition is not observed for tracheal tumors (12 males, 7 females), whereas for laryngeal ones, males outnumbered females by 5 to 1. This value appears to be similar to the sexual predisposition for laryngeal cancer described in human beings, where it is 5 times as common in males as females. 7,25 More frequent breeds affected are Alaskan Malamute, Doberman, and Boxer dogs. Of the 26 affected dogs, 7 (27%) were Arctic breeds (Alaskan Malamute or Siberian Husky), suggesting a predisposition in this type of dog.
No cause has been identified for cartilaginous tumors. The higher incidence in aged people has led to speculation that their development may be related to the ossification of the laryngeal cartilages, which begins most commonly in older individuals. Metaplasia secondary to chronic inflammation and chondroplastic predisposition of connective tissue cells arising from branchial tissue have been also postulated. 25
Clinical signs in patients described herein were typical of airway obstruction and similar to those previously reported, including loss or changes in vocalization (barking), coughing, noisy respiration, progressive dyspnea, stridor, cyanosis, and collapse in some cases. ‡ Pulmonary hyperinflation, an expected sequel to airway obstruction, was documented in only 1 patient. 19 There is little information in the literature on the radiographic appearance of canine laryngeal tumors. 7 Either this information was not included, or it was stated that radiographs were not made because the tumor was visible upon gross examination of the larynx through the glottis. Most tracheal tumors appear radiographically as a solitary distinct mass. Mineralization is unlikely except for osteochondromas. 2,6,7,19,23 Note that it is not possible to differentiate between inflammatory processes and benign or malignant neoplasms radiographically. Cysts or abscesses can show similar radiographic features. 7 Therefore, when abnormal densities are detected radiographically within the larynx or trachea, additional measures (eg, laryngoscopy, endoscopic biopsy) are required to obtain a definitive diagnosis.
Needle biopsy or cytology by fine-needle aspiration can reveal large plump cells with single and, occasionally, double nuclei suggestive of cartilaginous origin, 6,8 but it is not possible to definitively differentiate malignant or benign character. Excisional biopsy provides the most rapid and accurate means of final diagnosis 6 –8,29,32 and relieves the clinical signs for intraluminal tumors. A cartilage tumor is considered to be malignant when the following features are found, even in small scattered fields: many cells with plump nuclei, more than an occasional cell with 2 nuclei, and especially giant chondrocytes with single or multiple nuclei and clumps of chromatin. 25,32 Other cellular features of malignancy, including prominent nucleoli and irregularly shaped nuclei, also support a diagnosis of chondrosarcoma. 32 The absence of mitotic figures does not rule out malignancy, since cell division in chondrosarcomas may be amitotic. 25 It has been suggested that even a single mitotic figure strongly supports a diagnosis of malignancy in these tumors. 32
Laryngeal and tracheal chondromas in the dog appear to be identical to those in the skeletal system. Chondromas lack nuclear atypia, mitotic figures, necrosis, and invasive character. 6,7 The differentiation between chondroma and well-differentiated chondrosarcoma can be very difficult and is often a matter of personal interpretation. A diagnosis of chondroma should never create a false sense of security for the pathologist or surgeon, not only because chondroma-like areas can be present in the biopsy of a chondrosarcoma but because the clinical behavior of chondroma is often indistinguishable from a low-grade chondrosarcoma.
Osteochondromas are cartilaginous nodules with central endochondral ossification as a distinctive feature. They are the most commonly reported tumor in the trachea and only in young dogs (<1 year). || Tracheal osteochondromas can be differentiated from intraluminal tracheal chondromas: the latter do not contain marrow spaces, are entirely composed of cartilage, are usually pedunculated and attached to the tracheal ring by a cartilaginous pedicle, and occur in adult dogs. 8,32 It has been argued that osteochondromas represent a syndrome related to dysplasia of cartilage ring formation and so should be classified as osteochondromatous dysplasia, but the term osteochondroma is well established and more clearly conveys the tumorlike form. 6,8,11,32 Osteochondromas may be of sporadic occurrence (monostotic osteochondroma) or may be associated with osteochondromatosis (polyostotic osteochondromas or multiple cartilaginous exostosis). 2,6,14 Osteochondromatosis is a well-defined heritable syndrome in dogs, characterized by multiple benign cartilage growths that undergo endochondral ossification developing mainly in vertebrae, ribs, and long bones but also in the trachea. 2 It is plausible that the osteochondromas in our series were a component of osteochondromatosis, but this could not be confirmed from the data available. Because juvenile tracheal osteochondroma can occur in osteochondromatosis, an examination of the skeleton should be performed. Nontracheal osteochondromas in the dog can undergo malignant transformation into osteosarcoma. 27 In addition, osteosarcoma has developed in the tracheal bifurcation, the same area where osteochondromas frequently occur. 5 It is therefore possible that tracheal osteochondroma may also undergo malignant transformation.
Chondrosarcoma is a malignant tumor characterized by tumor cells that produce cartilage, not bone. 13,32 In human chondrosarcoma of bone, a relationship between histologic grading and biologic behavior is recognized. 12 In the dog, a similar relationship has been suggested. 4,32 The microscopic features of tracheal chondrosarcoma reported in our series—including presence of mitoses, areas of moderate to high cellularity, increased nuclear size, and chromatin variability—were most consistent with low- (case No. 10) and high-grade (case Nos. 8 and 9) chondrosarcomas. Rate of metastasis in cartilaginous tumors of larynx and trachea in human beings has been established around 8%, usually via hematogenous routes to the lungs, kidneys, or cervical spine, with occasional lymph node involvement. 25 Of the 7 laryngeal and tracheal malignant tumors reported in dogs, including cases presented herein, metastasis to the lung was confirmed only in 2 animals. 7,13 Histologic grade was specified only in 1 case as medium-grade chondrosarcoma. 7 Metastatic potential in cartilaginous tumors of larynx and trachea in the dog is therefore difficult to predict, because the number of cases described is insufficient to obtain statistically definitive conclusions.
As with any entity that occurs so sporadically, it has been difficult to identify the most effective treatment for these tumors. The opinion that conservative surgical removal of these tumors is the most appropriate treatment is widely held. 6,18,24,25,29,33 Other modes of treatment, such as radiotherapy, chemotherapy, and immunotherapy, have been shown to have little effect in humans. 25 Complete resection of large laryngeal tumors without total laryngectomy is impossible in some cases. 13 Managing patients after total laryngectomy is difficult because of the requisite permanent tracheostomy. 10 The prognosis should be guarded for those patients with large laryngeal tumors. Tracheal chondromas and osteochondromas may be amenable to complete resection. 2,6,7,19,23 However, the location in tracheal lumen may cause severe impairment of respiratory function and increase the risk of surgery. Two patients with intrathoracic osteochondromas in our series (case Nos. 6 and 7) were euthanized because of this. Osteochondromas of the appendicular skeleton cease growth with skeletal maturation. 2 If tracheal osteochondromas act similarly, then the lesion would not be expected to recur, and no regrowth has been noted in the cases reported. Carlisle et al 7 suggested that the prognosis for malignant tracheal tumors is poor, especially if the tumor involves the adventitial surface of the trachea. However, the other previous case report 1 and the cases presented herein, including those with extratracheal growth, indicate that the prognosis for cartilaginous tumors is better than previously suggested. Low-grade and easily accessible chondrosarcomas in the trachea may have a good prognosis.
Footnotes
Notes
Acknowledgements
We are grateful to the referring clinicians for their cooperation in this study. We also would like to acknowledge technicians of HISTOVET Pathology Diagnostic Laboratory (Barcelona, Spain) for their excellent technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.