
Abstract
Lymphoma is the most common feline upper respiratory tract (URT) tumor. Primary nasal and nasopharyngeal lymphomas have been evaluated as distinct pathological entities; however, data on their differing clinical behavior are missing. A total of 164 endoscopic- guided URT pinch biopsies were formalin fixed and routinely processed. Imprint cytological specimens were stained with May Grünwald-Giemsa. Immunohistochemistry for anti-CD20, CD3, FeLVp27, and FeLVgp70 was performed. Prognostic significance of clinicopathological variables was investigated by univariate and multivariate analysis. Lymphoma was diagnosed in 39 cats (24%). Most cats with lymphoma were domestic shorthair (32 [82%]), were male (F/M = 0.56), and had a mean age of 10.3 years (range, 1–16 years). Lymphomas were primary nasal in 26 cats (67%), nasopharyngeal in 6 (15%), and in both locations (combined lymphomas) in 7 cats (18%). Neoplastic growth pattern was diffuse in 35 cases (90%) and nodular in 4 (10%). Epitheliotropism was observed in 10 cases (26%). Tumor cells were large in 15 cases, were small and medium in 11 cases each, and 2 had mixed cell size. Submucosal lymphoplasmacytic inflammation was observed in 23 cases (59%). Cytology was diagnostic for lymphoma in 12 of 25 cases (48%). A B-cell origin prevailed (34 [87%]). Feline leukemia virus (FeLV) p27or gp70 antigen was detected in 21 lymphomas (54%). URT lymphomas were aggressive, with survival varying from 0 to 301 days (mean, 53 days). Epitheliotropism in 8 B-cell lymphomas (80%) and in 2 T-cell lymphomas (20%) correlated with prolonged survival. Age younger or older than 10 years had a negative prognostic value. Lymphoplasmacytic inflammation and FeLV infection may represent favoring factors for URT lymphoma development.
Lymphomas are among the most common feline malignancies, representing more than 50% of all tumors in cats. 18 Feline lymphoma prevalence rates are approximately 1.6% of cats in the general population and 4.7% of hospitalized sick cats. 18
The most common sites of occurrence are intestinal and mediastinal, 18 while primary nasal or nasopharyngeal lymphomas represent a rare manifestation, 18 accounting for less than 1% of all feline tumors. Nasal lymphomas seem more common in male cats, 12,14,25 presumably because of behavioral characteristics that make transmission of feline leukemia virus (FeLV) more efficient. The upper respiratory tract (URT) is considered a relatively rare site of lymphoma development; however, lymphoma represents still approximately 50% of primary URT mesenchymal tumors 1,14,16,18,25 and is the most common primary feline nasal tumor. 1,6,14,16,22 URT lymphomas originate more frequently in the solitary nasal location, 1,6,14,16,22 while 10% are found in the nasopharynx and 8% affect both anatomical compartments. 22 In previous studies, microscopic, immunophenotypical features 5,14,25 and the role of cytology in the diagnosis of feline primary URT lymphomas have been assessed. 22 However, the evaluation of the 3 distinct presentations of URT lymphoma (nasal, nasopharyngeal, or lymphoma simultaneously developing in both locations [combined lymphomas]) 22 as distinct clinicopathologic and prognostic entities seems unavailable. On the contrary, in human medicine, primary nasal and nasopharyngeal lymphomas are considered 2 clinically distinct diseases since nasal lymphoma bears a more frequent T-cell phenotype with poor response to chemotherapy and higher relapse rates. 21
The aim of this study was the evaluation of cytological, histological, phenotypical FeLV tissue antigen expression and follow-up data of 3 different URT lymphoma presentations—nasal, nasopharyngeal, and combined tumors—to find a possible significant prognostic role of the different clinical and pathological variables.
Materials and Methods
Case Selection
Pinch biopsies from all cases of nasal or nasopharyngeal feline disease were retrospectively collected from the surgical pathology archives of the Anatomical Pathology Section of the School of Veterinary Medicine of Milan between 2000 and 2012. All tissue samples were obtained by anterograde or retrograde endoscopic biopsy. The retrograde endoscopic technique was applied for nasopharyngeal tissue samples. A total of 39 (24%) of 164 cats undergoing nasal biopsies between 2000 and 2012 were diagnosed with lymphoma, representing 50% of nasal tumors diagnosed. Other tumors were carcinomas in 25 cats (15%) and mesenchymal tumors in 14 cats (9%).
For each cat with lymphoma, signalment, presenting complaints, clinical signs, diagnostic imaging, rhinoscopic appearance, multiple endoscopic pinch biopsies, histopathology, and, when available, cytology were collected.
Histological and Cytological Evaluation
All biopsy samples were fixed in 10% neutral-buffered formalin, routinely processed, and stained with hematoxylin and eosin (HE).
In cats with URT lymphomas, a number of biopsies varying from 4 to 14 (mean, 6) were collected by endoscopy. For primary nasal and for combined lymphomas, biopsies were performed from both (left and right) nasal cavities, even when a space-occupying lesion was not detected during endoscopic examination. Biopsy sampling was repeated to check for disease progression or to confirm the preceding diagnosis in selected cases. During scheduled clinical check-ups, the cat Nos. 5, 31, and 32 were reevaluated clinically and by endoscopy. Biopsies were taken after 3 and 9 months in cat No. 5 and after 1 and 3 months in cat Nos. 31 and 32.
For lymphomas, cytological samples from impression smears, fine-needle aspirates, and brushings were air dried and stained with May-Grünwald Giemsa.
To reduce inappropriate diagnostic interpretation, all the cytological and histological slides were blindly and independently submitted to pathologists with a different degree of experience, including 1 resident (S.S.F.) and 2 board-certified pathologists, with 1 more experienced in histopathology (R.P.) and 1 more experienced in cytopathology (C.M.). Only those cases that were classified in the same way by the 3 readings were included in the caseload. URT lesions were grouped in the following diagnostic categories: lymphomas, other neoplasms, inflammatory or degenerative lesions, and miscellaneous lesions. Cases of lymphomas were selected and subsequently classified on the basis of their anatomical location (nasal/nasopharyngeal/combined), growth pattern (follicular, nodular, diffuse, epitheliotropic), and cell type and grade, applying the modified World Health Organization (WHO) classification for lymphomas. 33 Mitotic index was evaluated counting the number of mitoses at a 400× magnification in 10 fields using the same microscope.
Immunohistochemical Staining
For all cases of lymphoma, cell phenotype and FeLV antigen expression were assessed. Unstained 5-μm sections from paraffin-embedded biopsy specimens were mounted onto Superfrost Plus Slides (Menzel Glasser; Gerhard Menzel, Glasbearbeitungswerk GmbH & Co, Braunschweig, Germany). For phenotypic and FeLV antigen expression evaluation, samples were stained with primary antibodies listed in Table 1. For all antibodies, antigen retrieval was achieved by heating slides in citrate buffer at pH 6.0 in a commercial pressure cooker Decloaker (Biocare Medical, Walnut Creek, CA) for 10 minutes. Endogenous peroxidase was quenched for 30 minutes with 3% hydrogen peroxide. Sections were stained using an avidin-biotin-peroxidase technique as previously described. 15 Omission of the primary monoclonal antibody or application of an isotype-matched nonspecific monoclonal antibody anti-canine CDH5R was used as a negative control. Formalin-fixed specimens from a reactive lymph node and from a FeLV-positive cat were used as positive controls. The immunoreaction was visualized with amino-9-ethyl-carbazole chromogen (AEC; Vector, Burlingame, CA). Sections were counterstained with Mayer’s hematoxylin and mounted with glycerine.
Panel of Primary Antibodies Used to Characterize Primary Feline Upper Respiratory Tract Lymphomas.
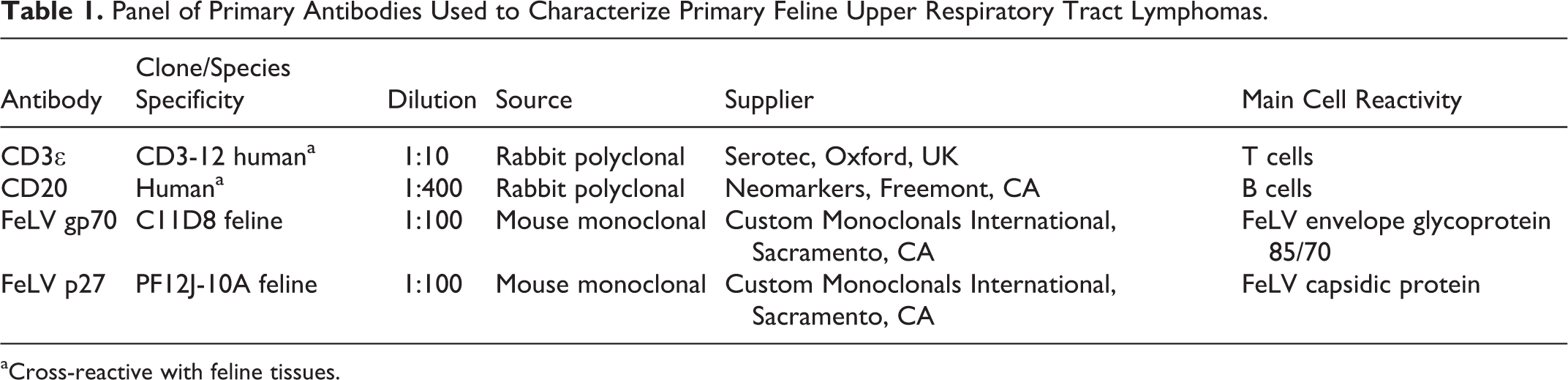
aCross-reactive with feline tissues.
Follow-up
Follow-up was performed when possible by the oncologists at the same institution and consisted of a clinical examination every 3 months. When this was not feasible, follow-up consisted of telephone interview with the owner or the referring veterinarian to collect clinical information, type of treatment, and time and cause of death.
Statistical Analysis
Statistical analysis was performed following when possible the guidelines of the American College of Veterinary Pathologists’ Oncology Committee. 37 The end point considered for each cat with lymphoma was time to death, calculated as the time elapsed from the date of diagnosis to the date of death for any cause, or to the date of last clinical information for cats that were alive at the study closing date (right-censored times). 37 Median follow-up was estimated by the reverse Kaplan-Meier method. 29 Overall survival probability curve was estimated by the Kaplan-Meier method. First, the putative prognostic role of the considered variables (age, sex, breed, anatomical site, size of lymphomatous cells, neoplastic phenotype, FeLV status, mitotic index, and epitheliotropism) was investigated, including each single variable in a Cox regression model (univariate analysis). Aiming to evaluate the adjusted prognostic role in Cox multivariable regression models, the maximum number of variables that can be included to avoid unreliable results depends on the number of observed deaths. According to the caseload included in the study, a ratio of 1:5 was considered, as previously suggested. 36 Since it was not possible to include all the above-mentioned variables, only a subset of variables were jointly analyzed in multivariable regression models (mitotic index, age, FeLV status, phenotype, and epitheliotropism). These variables were selected according to the specific clinical experience of the authors. A model containing only variables with the greatest prognostic role was then obtained by a backward selection procedure based on the Akaike information criterion (AIC). 35 Continuous variables (age and mitotic index) were analyzed according to their original measurement scale in such a way as to maintain their maximum possible prognostic information. Potential nonlinear relationships between continuous variables and logarithm of the hazard in the Cox model were evaluated by restricted cubic spline transforms. 13
Results are reported in terms of estimated hazard ratios (HRs) with 95% confidence intervals (CIs). For categorical variables, one of the modalities was chosen as reference. Thus, for each of the remaining modalities, the HR is the ratio between the hazard of death for this modality and the hazard of death of the reference. The null hypothesis of each regression coefficient equal to zero was evaluated by the Wald test, and the prognostic contribution of the variable to the model was evaluated by likelihood ratio test. For continuous variables, model estimates in terms of HRs cannot be easily interpreted in the case of a nonlinear relationship between the variable and model response. Thus, after identifying the value of the variable corresponding to the minimum hazard of death (reference), selected hazard ratios for values of the variable greater and lower than reference were provided to describe the prognostic behavior.
Results
URT Lymphomas: Signalment and Clinical Findings
Signalment and major clinical complaints divided for the 3 different URT lymphoma presentations are summarized in Supplemental Table S1. In cats with URT lymphoma, median age was 10.3 years (range, 1–16 years) with a female/male ratio of 0.56 and a majority of domestic short-haired (DSH) cats (32/39 [82%]). Other breeds included 3 Siamese, 2 Chartreux, 1 Persian, and 1 Devon Rex. FeLV and feline immunodeficiency virus (FIV) serology were available in 7 cats (18%); all except 1 (cat No. 29) were FeLV negative, while two cats were FIV positive (cat Nos. 1, 27). Major clinical complaints for cats with lymphoma were nasal discharge (30/39 [77%]), sneezing (26/39 [67%]), stertor (18/39 [46%]), dyspnea (9/39 [23%]), epiphora (8/39 [21%]) or ocular discharge (4/39 [10%]), epistaxis (8/39 [21%]), and anorexia (7/39 [18%]).
Skull radiographs (11 [28%]) or computed tomography (CT) scans (8 [21%]) were performed prior to rhinoscopy in some cats with URT lymphoma. Based on diagnostic imaging and rhinoscopy, 26 of 39 (67%) lymphomas were primary nasal, 6 of 39 (15%) were nasopharyngeal, and 7 of 39 (18%) had both a nasal and nasopharyngeal location and were termed combined lymphomas (CLs).
By rhinoscopy, lymphomas were described as exophytic, pale pink to whitish, cerebroid, and friable space-occupying lesions in 28 of 39 (72%) cases. No masses were evident in 11 cats (28%), where a rough thickened mucosa was documented.
Cytological Findings in URT Lymphomas
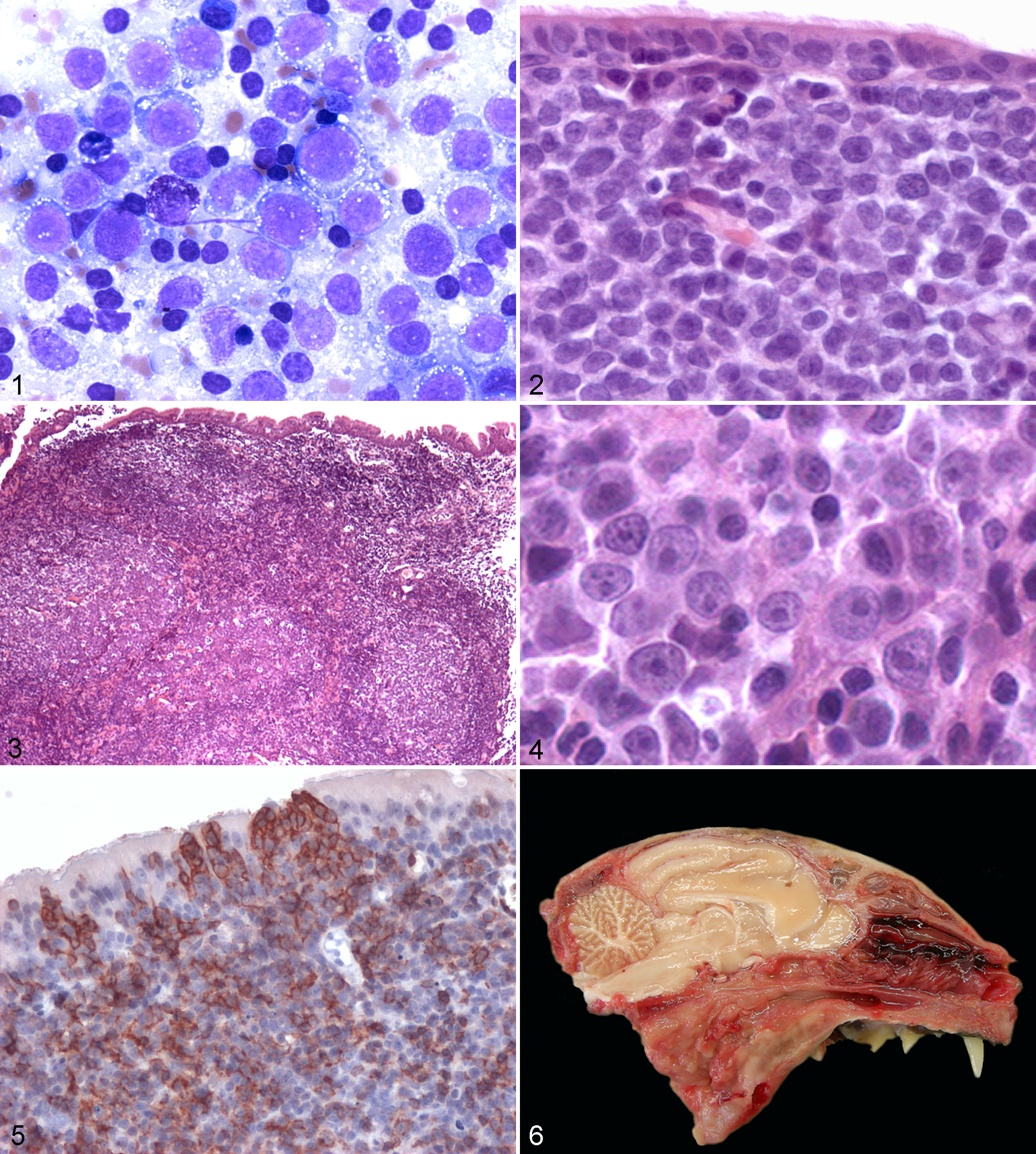
Cytological specimens were available in 25 of 39 cases (64%) and were obtained by impression (16 [64%]), brushing (6 [24%]), or fine-needle aspiration (3 [12%]). A diagnosis of lymphoma was attained by cytology in 12 of 25 (48%) cases, while for 11 cases (44%), a false-negative diagnosis of lymphoplasmacytic rhinitis was achieved. An inconclusive cytology was recorded in 2 cases (8%). All cytological samples, with the exception of the 2 inconclusive cases, exhibited good cellularity; small lymphocytes admixed with plasma cells, neutrophils, or macrophages were often observed in association with the neoplastic population (Fig. 1). Less frequent findings included hyperplastic to dysplastic respiratory epithelium, necrosis, and presence of occasional osteoclasts.
Pathology and Phenotype of URT Lymphomas
Microscopic features, lymphoma classification, and phenotype are summarized in Supplemental Table S2. The incidence of lymphoma cell type based on tumor location is summarized in Table 2.
Incidence of Cell Type Based on Tumor Location.

Histological growth pattern was diffuse (Fig. 2) in 35 URT lymphomas (90%) and nodular (Fig. 3) to follicular in 4 cats (10%). Comparing the differing anatomical distributions, primary nasal lymphomas were diffuse in 25 cases (96%) and nodular in 1 cat (4%). Five cases (83%) of nasopharyngeal lymphoma had diffuse cell growth, and 1 (17%) was nodular. Combined lymphomas were observed in 7 cats (18%) and were characterized by diffuse growth in 5 cats (71%) and nodular growth in 2 cats (29%).
Comparing the cell type, 11 cases (28%) were diagnosed as small cell lymphoma, including lymphocytic (6 [55%]), prolymphocytic (4 [36%]), and plasmacytic (1 [9%]). Medium-sized cell lymphomas were diagnosed in 11 cases (28%); 8 of 11 (73%) were medium sized, not otherwise specified (NOS); 2 were plasmacytomas (18%); and 1 was a peripheral T-cell (PTCL)–like lymphoma (9%). Two follicular center cell lymphomas were observed, one grade I and one grade II. Large cell lymphoma (Fig. 4) was diagnosed in 15 cats (38%), with 13 cases having an immunoblastic morphology (87%). Of the primary nasal lymphomas, 11 were large (42%), 7 were intermediate (27%), and 8 (31%) were small cell cases. Nasopharyngeal lymphomas were large immunoblastic in 2 cats (33%), intermediate (including 1 plasmacytoma) in 3 cases (50%), and 1 case of mixed cell size (17%) diagnosed as follicular center cell lymphoma grade II. Combined lymphomas were large cell in 2 cases (29%), intermediate in 1 case (14%), and small cell in 3 cases (43%), and 1 mixed cellularity (14%) was diagnosed as a follicular center cell lymphoma grade I. Regardless of the anatomical location, in 23 cases (59%) of URT lymphomas, variable degrees (mild to severe) of submucosal plasmacytic to lymphoplasmacytic inflammation were evident.
Additional histopathological findings included multifocal mucosal ulceration with secondary neutrophilic and catarrhal inflammation, cystic dilation of mucous glands, edema, fibroplasia, and bone remodeling. Concurrent hyperemia, edema, and abundant catarrhal to purulent exudate were detected in 24 of 39 cats (61.5%).
A B-cell phenotype was identified in 34 of 39 URT lymphomas (87%). Of these, the largest number was represented by diffuse large cell lymphomas (15 [44%]), followed by small cell lymphomas (8 [24%]), intermediate cell NOS (7 [21%]), plasmacytomas (2 [6%]), and follicular lymphomas (2 [6%]). In 3 of 39 cases (8%), a T-cell phenotype was identified, comprising 2 diffuse small cell lymphomas and 1 PTCL-like lymphoma. In 2 of 39 cases (5%), 1 small cell lymphoma and 1 intermediate cell lymphoma, neoplastic cells were negative for T-cell and B-cell markers. Epitheliotropism (Fig. 5) was observed in 10 cases (26%), specifically in 8 cases of B-cell lymphomas (80%) and in 2 T-cell lymphomas (20%).
Phenotypic distribution in nasal lymphomas was characterized by a predominance of B-cell tumors (22 [85%]), with 2 cases (8%) of T-cell and 2 cases (8%) of the non B–non T-cell phenotype. All nasopharyngeal lymphomas displayed a B-cell origin. Combined lymphomas were B cell in 6 cases (86%) and T cell in 1 cat (14%).
Immunohistochemical Expression of Viral Antigens in URT Lymphomas
FeLV antigen expression in conjunction with anatomical distribution of URT lymphomas is listed in Supplemental Table S2. FeLV p27 and FeLV gp70 antigen expression either singly or in conjunction was detected by immunohistochemistry in a total of 21 of 39 cases (54%). Expression of FeLV p27 was observed only in 17 of 39 (44%), while gp70 only was observed in 12 of 39 cases (31%). Concurrent positivity for FeLV antigens was detected in 8 of 39 cats (21%). These cats were considered productively FeLV infected. Expression of either antigen in conjunction with lymphoplasmacytic inflammation was observed in 12 of 39 cats (31%).
Therapy and Follow-up
Five cats were lost to follow-up at 7, 7, 10, 43, and 54 days after diagnosis. Combination chemotherapy and/or radiation therapy were always offered but refused by owners in all but 1 cat that received radiation therapy (cat No. 5).
According to the reverse Kaplan-Meier method, median follow-up was 301 days, the first quartile (25%) was 60 days, and the third quartile (75%) was 381 days. The survival probability at 30, 60, and 300 days after surgery was 0.793 (95% CI, 0.6751–0.932), 0.375 (95% CI, 0.2422–0.581), and 0.153 (95% CI, 0.0595–0.396), respectively.
Major causes of death were euthanasia (21 cats) due to the severity of respiratory obstruction caused by the disease. At the end of the study, 6 cats were still alive, with 1 cat affected by a small B-cell lymphocytic lymphoma treated with radiation therapy surviving for 1293 days (cat No. 5).
In 4 cats, lymphoma was confirmed by full necropsy (cat Nos. 1, 27, 28, 33). Multiorgan involvement was found in 3 cases (cat Nos. 1, 27, 33), with renal (cat Nos. 27, 33) and myocardial infiltration (cat No. 27) and contiguous central nervous system (CNS) involvement by ethmoidal bone lysis (cat Nos. 1, 33). In 1 case (cat No. 28), lymphoma was limited to the nasopharyngeal location (Fig. 6). In this cat, severe monolateral dysplasia of the bronchial walls was also evident.
Statistical Analysis
In univariate analysis, concerning age, a nonlinear relationship was considered because the fit of a 3-knots spline function was better than the fitting by only a linear term (likelihood ratio test for the model with spline = 3.25, P = .1972; likelihood ratio test for the model with only the linear term = 0.55, P = .4578; likelihood ratio test for the contribution of the nonlinear term = 2.6958, P = .10). No variables showed a significant prognostic value based on a significance level of .05 (Table 3).
Univariate Analysis.
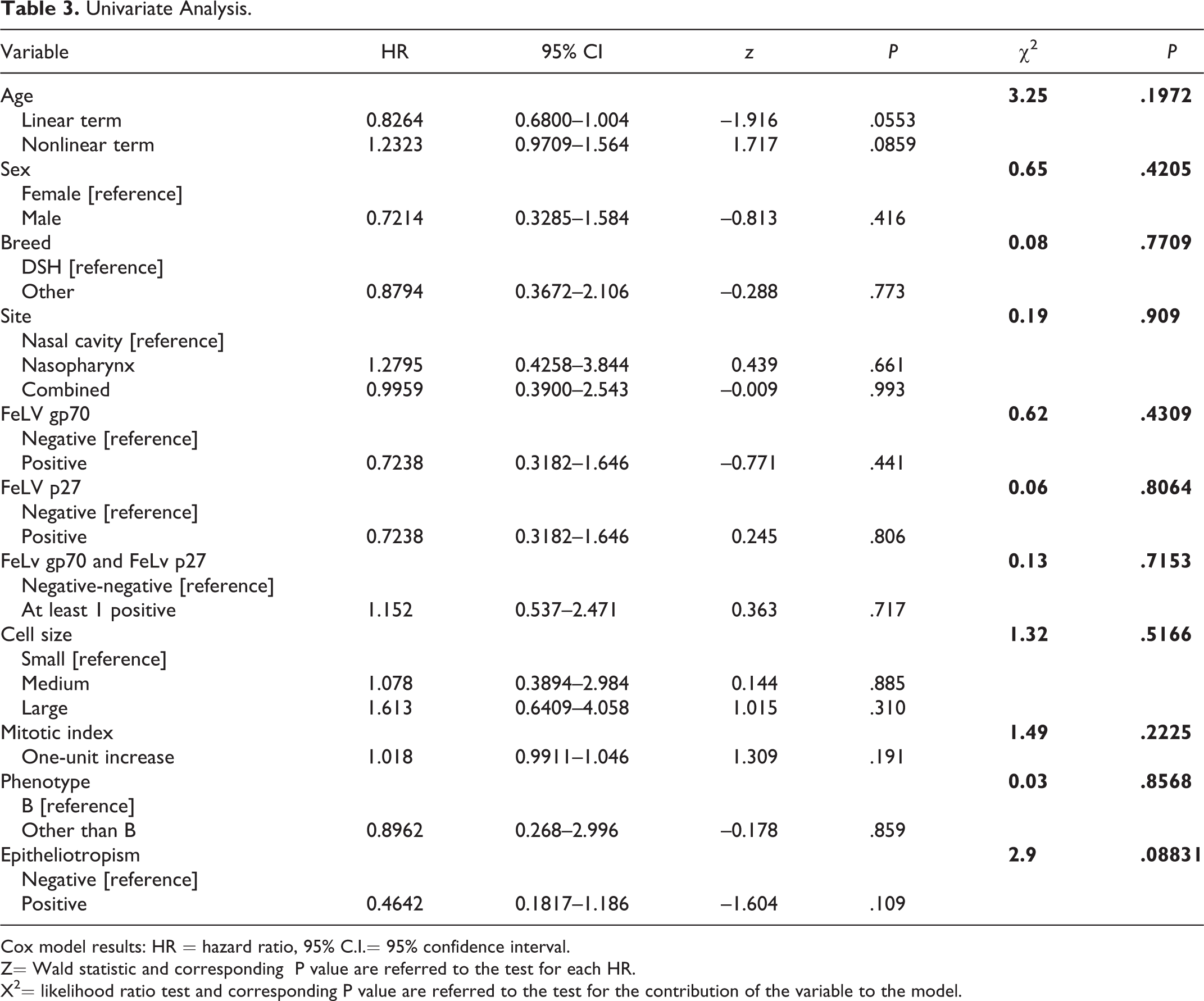
Cox model results: HR = hazard ratio, 95% C.I.= 95% confidence interval. Z= Wald statistic and corresponding P value are referred to the test for each HR. X2= likelihood ratio test and corresponding P value are referred to the test for the contribution of the variable to the model.
When mitotic index, age, FeLV positivity, phenotype, and epitheliotropism were jointly considered in a multiple regression model (Table 4), a significant prognostic role was obtained only for epitheliotropism (likelihood ratio test = 4.5316, P = .03327), where the subjects with negative epitheliotropism showed a greater risk of death than did subjects with positive epitheliotropism (hazard ratio = 0.3115). After applying the backward selection procedure to the above-mentioned model, only age and epitheliotropism were maintained as putative prognostic factors.
Multivariate Analysis.
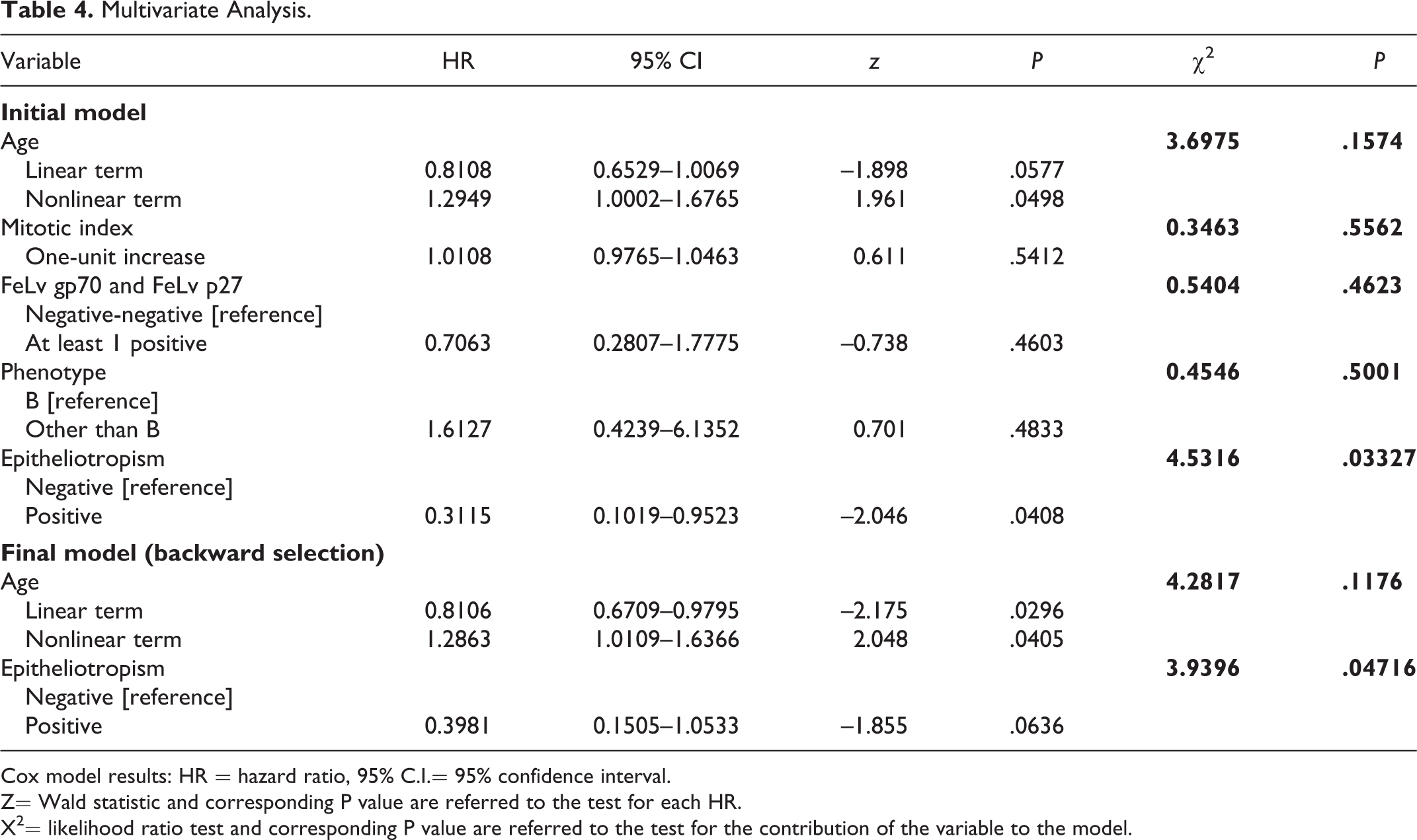
Cox model results: HR = hazard ratio, 95% C.I.= 95% confidence interval. Z= Wald statistic and corresponding P value are referred to the test for each HR. X2= likelihood ratio test and corresponding P value are referred to the test for the contribution of the variable to the model.
Considering 10 years as the reference, a U-shaped behavior of the hazard was observed as a function of age. Thus, the estimated hazards of death of 3-, 5-, and 7-year-old cats are about 1.47, 2.22, and 3.38 times greater than the hazard of death of a cat aged 10 years, respectively, and the estimated hazards of death of 12-, 13-, and 15-year-old cats are about 1.18, 1.47, and 2.46 times greater than the hazard of death of a cat aged 10 years. The hazard of death of subjects with negative epitheliotropism is about 2.5 times greater than the hazard of death of subjects with positive epitheliotropism.
Discussion
This report describes and compares pathological findings, FeLV antigen expression, and survival of feline URT lymphomas by their division into nasal, nasopharyngeal, or combined primary anatomical locations. Nasal or nasopharyngeal tumors have been mostly evaluated separately, 5,12 and lymphomas in the 3 distinct presentations seldom have been compared. 22 Histopathology in conjunction with diagnostic imaging (radiographs and CT scans) resulted in the classification of URT lymphomas into 26 nasal, 6 nasopharyngeal, and 7 combined nasal-nasopharyngeal lymphomas. The predominance of primary nasal lymphomas paralleled the frequency reported previously. 22 No major differences in phenotype, classification, and prognosis were evident. Of particular note were that nasopharyngeal lymphomas always had a B-cell origin and that combined lymphomas did not express FeLV antigens. Also, epitheliotropism was a positive prognostic factor, while age correlated with a poor prognosis.
The 39 cats with lymphoma were drawn from a case series of 164 cats biopsied for nasal lesions. Of these, lymphomas were 24% of all lesions, accounting for 50% of tumors. This distribution resembled frequencies previously reported, with lymphoma being the most common URT tumor. 1,6,14,16,25 Our findings closely paralleled a retrospective study of nasopharyngeal disease in 53 cats reporting that 49% had lymphoma and 28% had polyps. 1
Of 164 nasal biopsies, 163 were diagnostic. The result of the diagnostic accuracy of histopathology was not comparable with other veterinary reports since studies on the diagnostic precision of endoscopic nasal biopsy evaluation seem not to be available. However, this result seems to represent a high success rate compared with what has been reported for the diagnosis of primary nasal carcinoma in humans, in whom 5% percent of cancers are missed at endoscopic biopsy. 20 The diagnostic success rate observed herein may derive from the expertise of the surgeon providing samples of large size and an adequate number of biopsies that ranged from 4 to 14 per single case. In humans, for nasal carcinoma diagnosis, an average of 6 biopsies from both diseased and adjacent apparently healthy nasal tissue are suggested as the minimum number for the correct diagnosis. 20 Also, in this study, depth of biopsies was pivotal since the inclusion of the deep lamina propria and turbinates allowed the evaluation of the distribution and of the infiltrative behavior of tumors. Besides, endoscopic-guided biopsy permitted the visualization of nasal and nasopharyngeal mucosa, assisting in the selection of lesional areas to sample. 20 The success rate of histology contrasted with the poor results of cytology, which was diagnostic only in 50% of lymphomas. The main problem encountered was sample contamination by inflammation, leading to misdiagnosis. Our results parallel the observation that many of the cytological sampling techniques have an unacceptably low yield of diagnostic material for nasal specimens. 2,23 In concordance with previous reports, 2,6 impression smears from biopsies and fine-needle aspiration biopsies detected lymphoma more accurately compared with brushing. Brushing is a technique performed blindly, 2,6 and thus small tumors can be missed and inflammatory findings may be misleading. Also, most lymphomas of this caseload developed in the mid to deep lamina propria, which is not sampled by brushing. Similar problems have been reported for nasopharyngeal masses, 1 since cytology is undertaken without direct visualization of the nasopharyngeal area, leading to an inaccurate diagnosis. 1 Crush cytological specimens have demonstrated a better diagnostic yield. 6 Unfortunately, contrary to imprints, crush sample biopsies need to be sacrificed, reducing the subsequent diagnostic capability of histopathology. Despite a low diagnostic potential, in this report, cytology was extremely useful for lymphoma classification thanks to a better assessment of cell morphology. The correct WHO cytological classification of lymphomas is essential for their prognostication. Thus, for lymphoma diagnosis, cytology should be performed when possible and evaluated in conjunction with histopathology.
Cats developing URT lymphomas were mostly adult to aged males, similar to previous reports, 12,25 but contrasting with findings in other caseloads. 14 The predominance of male cats has been hypothesized to derive from the male territorial behavior that makes transmission of FeLV more efficient. 18 In our caseload, FeLV antigen positivity demonstrated by immunohistochemistry was distributed almost equally among sexes, contrasting with this hypothesis. FeLV serological positivity has been correlated to the anatomical form of lymphoma, with most positive cats having mediastinal lymphoma (90%) and multicentric lymphoma (80%) and less than 10% having cutaneous lymphoma. 18 FeLV serology has been seldom evaluated in URT lymphomas. In this study, most cats were not tested for FeLV, likely owing to their old age; however, 6 of 7 cats tested were negative. FeLV p27 capsid and gp70 envelope immunohistochemical protein expression by neoplastic cells was documented in 54% of our cases, but combined URT lymphomas were always negative. A comparison with other URT lymphoma caseloads was not possible due to the lack of data regarding FeLV tissue antigen expression. The old age of cats developing URT was considered incongruent with a causal role of FeLV since it is well established that FeLV-positive cats generally develop lymphomas at a young age; 17 thus, the finding of FeLV protein expression by neoplastic cells was surprising. Significantly, old seronegative cats may still bear the virus at the genomic level and can transcribe FeLV upon reactivation or neoplastic transformation of infected cells. 7 Noteworthy, FeLV gp70 expression was observed in 12 cats. Expression of FeLV gp70 denotes viral particle assembly, confirming a productive infection. 30 Thus, FeLV might still be involved in feline URT lymphoma development.
A concurrent plasmacytic inflammation was observed in 59% of URT lymphomas. Chronic rhinitis-rhinopharyngitis is considered a consequence of prior infection with either feline herpesvirus type 1 or feline calicivirus. 34 Up to 80% of cats that recover from acute viral URT infections may become chronic carriers, which can lead to persistent clinical signs and inflammation. 10 In addition, viral infection causes injuries that predispose to secondary bacterial disease. 14 Chronic inflammation is considered a risk factor for the development of a variety of cancers, including hematopoietic malignancies in humans. 8,11,28 In humans, B-cell lymphomas developing after longstanding chronic inflammation 4,26,31 seem common, and the association between bacterial and viral infections with lymphoma development is well documented for mucosa-associated lymphoid tissue (MALT) B-cell lymphomas. 8,11,28 Notably, in our caseload, inflammation and FeLV tissue antigen positivity were concurrently documented in 31% of cats. Specifically, chronic persistent rhinitis may favor expansion of virally transfomed B-lymphoid cells, explaining the higher frequency of URT lymphomas with a B-cell phenotype observed in this and other caseloads. 5,22,25
The histological diagnosis of lymphoma was performed using the modified WHO classification. 32,33 In other studies of feline URT lymphomas, the Revised European American Lymphoma (REAL)/ revised WHO classification 5 and the National Cancer Institute working formula classification 22 have been applied. Large cell lymphomas were mostly identified in our series (39%), with a prevalence of immunoblastic morphology, paralleling other studies. 5,22 Interestingly, small cell lymphomas were also frequent (28%). As for these cases, rare lymphoma variants such as plasmacytoid/plasmacytic 22 follicular grade II, 5 as well as anaplastic large and small cell lymphomas, 14 have rarely been described.
Epitheliotropism was unexpectedly identified in B-cell lymphomas of the 3 URT anatomical types. In cats, epitheliotropism usually has been described in cutaneous and gastrointestinal T-cell lymphomas; 3,9,24,27 however, this growth pattern has also been occasionally reported in feline URT lymphomas. 22,25 Human studies have documented epitheliotropism of B cells in tonsillar hyperplasia and in MALT lymphomas. 19 Interestingly, in our study, epitheliotropism was statistically associated with a prolonged survival time of diseased cats. Considering other histological variables, mitotic index, cell size, phenotype, and FeLV antigen expression had no significant correlation with mortality. Epitheliotropism and age, evaluated on a continuous scale, were the only prognostic factors identified; however, lack of statistical evidence of other variables having a significant prognostic impact should be considered with caution. In fact, power of statistical tests may be low, and the reduced sample size did not permit a full evaluation of the joint prognostic role of the considered variables. For a more reliable evaluation, a case series with at least 100 deaths would be needed. Also, an increased number of combined and nasopharyngeal lymphomas are necessary to obtain a representative selection of cases providing a suitable cohort for statistical analysis of potentially significant prognostic variables.
In conclusion, URT lymphomas are aggressive tumors with a prevailing primary nasal B-cell origin. Lymphoplasmacytic inflammation is frequently associated with URT lymphomas and may represent alone, or in conjunction with FeLV infection, a possible favoring factor in lymphoma development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.