
Abstract
A 1-year old female spayed German Shepherd dog was evaluated for acute onset of dyspnea. Pyogranulomatous inflammation and green globoid structures were present on aspirates of the affected lung. Impression smears and histopathology confirmed pyogranulomatous pneumonia, with large amounts of lipid corresponding to the green structures noted cytologically, and identified poorly staining bacterial rods within lipid vacuoles. Special stains confirmed the presence of acid-fast bacterial rods, and polymerase chain reaction and DNA sequencing identified the organism as Mycobacterium fortuitum. M. fortuitum pneumonia is well described in humans and has previously been reported in 4 dogs and 1 cat. Lipid was a prominent cytologic and histologic feature, as is often described in humans and in the single feline case report. Additionally, this case highlights the variable cytologic appearance of lipid, as well as Mycobacterium spp, which are classically nonstaining with Wright-Giemsa.
A 1-year-old female spayed German Shepherd dog presented to the Louisiana State University veterinary teaching hospital and clinic emergency medicine service for a 5-day history of dyspnea (unresponsive to oral amoxicillin/clavulanic acid therapy) and weight loss. On presentation to the hospital, the patient was quiet, alert, and responsive, as well as dyspneic and pyrexic (104.3°F) with pink tacky mucous membranes and delayed capillary refill time (3 seconds). On thoracic auscultation, bronchovesicular sounds were increased in the right lung fields and decreased over the left lung fields. Heart rate was 120 beats per minute with normal sinus rhythm and muffled heart sounds auscultated over the left hemithorax. The remainder of the physical examination was within normal limits. Clinically relevant abnormalities on routine complete blood count and serum biochemistry panel included a moderate mature neutrophilia (20.9 × 103/μl; reference interval [RI], 3–11.5 × 103/μl), lymphopenia (0.7 × 103/μl; RI, 1–4.8 × 103/μl), and monocytosis (1.6 × 103/μl; RI, 0.1–1.4 × 103/μl) consistent with a stress or inflammatory leukogram.
On 3-view thoracic radiographs, there was a lobar sign of the left cranial lung lobe with multiple large air bronchograms and leftward shift of the mediastinum. Additionally, there was an ill-defined alveolar opacity within the left caudal lung lobe with mild retraction from the thoracic wall. Radiologic diagnosis was severe left cranial lung lobe atelectasis, left cranial and caudal lung lobe alveolar disease, and mild focal left-sided pleural effusion. A complete abdominal ultrasonogram identified splenomegaly (considered most likely a breed-related change). An abbreviated thoracic ultrasonogram was performed for cytologic sampling of the lung, followed by bronchoscopy under general anesthesia for airway evaluation and sampling. At the level of the principal bronchi bilaterally and extending down into the lower airways, the mucosa was erythematous and contained a moderate amount of mucopurulent material. Bronchoalveolar lavage fluid was collected and submitted for cytologic analysis. The patient recovered uneventfully and remained in hospital receiving oxygen therapy (oxygen cage at 40%), maintenance intravenous fluids (Plasmalyte, 55 ml/h), intravenous ampicillin sodium/sulbactam sodium (22 mg/kg, 3 times per day), and intravenous anti-inflammatory steroid regiment (dexamethasone sodium phosphate, 0.15 mg/kg, 1 time per day).
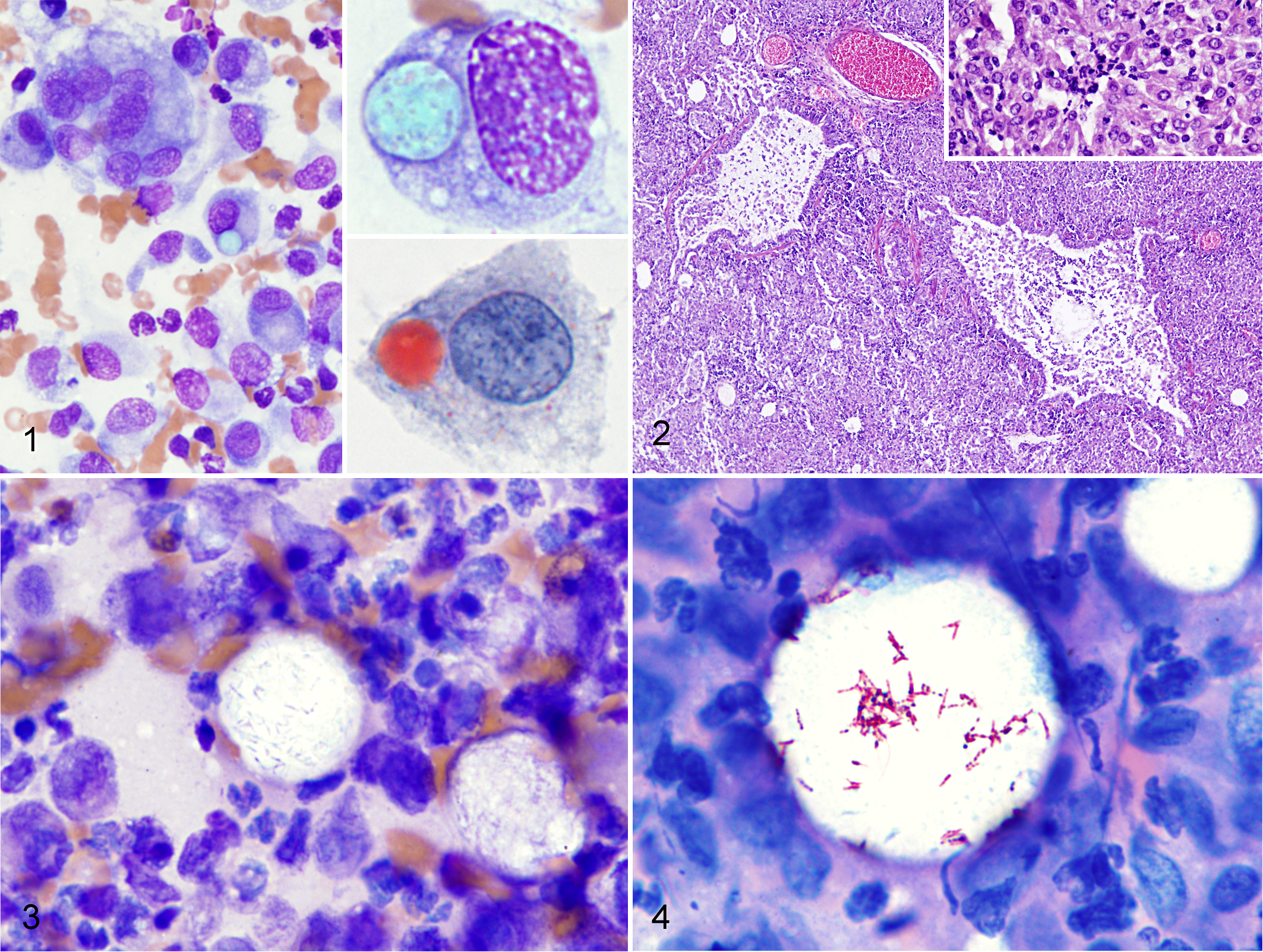
Cytologic preparations from the left cranial lung lobe contained many well-preserved nucleated cells consisting of 54% macrophages, 40% nondegenerate neutrophils, and 6% small lymphocytes (Fig. 1). Macrophages frequently contained 1 or 2 spherical 3- to 5-μm-diameter light green inclusions that lacked internal structures (Fig. 1). These elements were occasionally noted free in the background. While the structures were of unknown identity and significance, fungal spores were considered a possible differential. Cytologic preparations of the bronchoalveolar lavage fluid contained a similar population of inflammatory cells but with a predominance of nondegenerate neutrophils and occasional intrahistiocytic spherical inclusions. The cytologic diagnosis was pyogranulomatous inflammation, and Gomori’s methenamine silver stain did not identify fungal elements.
Differential diagnoses for the pyogranulomatous pneumonia included inhalation of a foreign material or an infection with fungi, protozoa, filamentous bacteria, or Mycobacterium spp. The patient remained in hospital for 3 days without resolution of clinical signs, at which time the owners elected for humane euthanasia.
Postmortem Findings
A partial cosmetic necropsy was performed, and a portion of the affected left cranial lung lobe was sampled. Impression smears of this tissue appeared cytologically similar to previous aspirates from this site with the addition of large numbers of discrete clear variably sized vacuoles present in the background. Oil red O staining demonstrated large amounts of lipid both extracellularly and within macrophages (Fig. 1). Histologically, alveolar spaces were diffusely filled with sheets of epithelioid macrophages, which were also present within bronchioles, admixed with proteinaceous debris and degenerate neutrophils (Fig. 2). Macrophages frequently appeared foamy or contained clear round discrete vacuoles interpreted as lipid. Large clear discrete extracellular lipid vacuoles were also noted. Poorly staining beaded bacterial rods were noted within these extracellular vacuoles, both cytologically and histologically (Fig. 3), and special stains showed them to be acid-fast (Fig. 4), Gram positive, and unstained with Gomori’s methenamine silver (not shown). Frozen tissue was submitted to the University of Georgia–Athens Veterinary Diagnostic Laboratory, and a Mycobacterium spp. was amplified via polymerase chain reaction from samples of the left lung. Sequencing of the heat shock protein gene hsp65 yielded a 419–base pair product with 100% similarity to Mycobacterium fortuitum (GenBank accession No. JX154102.1).
Discussion
M. fortuitum is a nontuberculous, nonlepromatous, rapidly growing mycobacterium isolated from soil and water sources worldwide. 2 In small animals and humans, M. fortuitum is an opportunistic pathogen colonizing the skin or other organs of immunocompetent hosts in the presence of injury, with reports of systemic infection generally limited to immunocompromised individuals. 6
Among small animals and humans, M. fortuitum most commonly causes dermatitis and panniculitis, presenting clinically as chronic nonhealing wounds often with draining tracts. 6 While less common, M. fortuitum pneumonia is well-described in humans and has been documented in 4 other dogs and 1 cat.2,5,6 These small animal cases share similar features, including neutrophilic inflammation in airway wash samples and granulomatous to pyogranulomatous inflammation on aspirates and biopsies of the affected lung. Bacteria were not documented in these reports on Wright-stained cytology specimens when performed, but poorly staining bacteria were often noted histologically on hematoxylin and eosin sections of lung, present in clear vacuoles surrounded by granulomas or pyogranulomas as in the current case. 2,5,6 Clinically, all animals were young (6 months to 4 years of age) with radiologic evidence of alveolar infiltrates. Contributing factors for development of M. fortuitum pneumonia in the documented canine cases is unknown, and all animals were seemingly immunocompetent. In the reported feline case, presumed aspiration of lactulose was thought to be a major contributor, and lipid-laden macrophages and extracellular lipid were prominent histologic findings. 2
In the current case, the patient was also seemingly immunocompetent, although given the breed, an underlying IgA deficiency is one possible consideration. 3 Mycobacterium spp. infection with IgA deficiency has been described in a human case report. 1 While the exact mechanisms by which IgA protects mucosal surfaces remain nebulous, in a murine model, IgA-deficient mice infected with Mycobacterium bovis had abrogated production of interferon gamma, a potent macrophage activator important in clearance of intracellular bacteria. 8 In a case series of canine leproid granuloma, 2 German Shepherd mixed-breed dogs and 1 pure-bred German Shepherd dog were represented out of a total of 7 patients. However, as in our case, no diagnostics were reported to investigate the possibility of an underlying IgA deficiency. 3
The source of lipid in the samples collected is likewise a matter of speculation. While aspiration of exogenous lipid cannot be excluded, the lipid may have been endogenous, from surfactant and/or intracellular release of cholesterol and other lipids. Alveolar lipid accumulation has been reported in both experimentally induced infections in mice and naturally occurring pneumonia in humans infected with Mycobacterium tuberculosis in the absence of aspiration. 4 Furthermore, secondary endogenous lipoid pneumonia has been described under sterile conditions, when cellular necrosis occurs distal to occluded airways. 9 In many of the documented human cases, aspiration of oily substances such as mineral oil and clarified butter are commonly associated with M. fortuitum pneumonia and are postulated to contribute to the growth and pathogenicity of the organism. 2 This association is not surprising considering the central importance of lipid to mycobacterial structure, survival and virulence.
Trehalose 6,6′-dimycolate (TDM) is the most abundant and toxic glycolipid extractable from the surface of M. tuberculosis and is also present in M. fortuitum. 4 TDM is waxy and hydrophobic, requiring a lipid-rich environment for formation of the highly toxic molecular monolayer. The biological relevance of this concept has been demonstrated in mouse experiments in which 30 μg of TDM proved fatal when administered in an oil-water suspension but was non-toxic when administered without oil, even at 1000-fold the original dosage. 4 Along these same lines, mice experimentally infected with delipidated M. tuberculosis mounted a neutrophilic inflammatory response, clearing the infection by 6 days. No granuloma formation was noted in these animals, even when injections were made into adipose tissue, underscoring the important synergy between host and bacterial-derived lipids in mycobacterial infection. 4
An unusual finding in this case was the cytologic appearance of lipid as variably sized green globoid structures. A similar cytologic appearance was noted in a transtracheal wash sample from a dog that aspirated cod liver oil. 7 This appearance is likely not unique to exogenous lipids, however, as similar oil red O–positive material was found in aspirates of a lipoma (author’s unpublished observation).
Another interesting finding was the positive cytologic staining of M. fortuitum. Classically, Mycobacterium spp. are considered negatively staining on Wright-Giemsa cytologic preparations. However, in a retrospective study identifying Mycobacterium spp. in Wright-stained marrow aspirates from HIV-infected patients, Mycobacterium spp. appeared as refractile beaded rods that varied from clear to red. 10 The authors hypothesized that the red color was not intrinsic to the organism or staining technique but imparted by chromatic aberration, as organisms were colorless when viewed with apochromat objective lenses and condensers. 10
The pathologic findings in this case suggest that the relationship between lipoid pneumonia and M. fortuitum infection as documented in humans may be applicable to veterinary patients. It also illustrates the variable appearance that lipid and Mycobacterium spp. may have cytologically, the recognition of which may aid in timely and accurate cytologic diagnosis. We conclude that mycobacterial pneumonia should be considered a clinical differential for small animals with evidence of alveolar lung disease, pyogranulomatous pneumonia, and intrapulmonary lipid accumulation.
Footnotes
Acknowledgement
We thank Dr Britton Grasperge for assistance with photomicrographs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.