
Abstract
Lycoperdonosis is a rare respiratory disease that results from the inhalation of spores released from the Lycoperdon (puffball) mushroom. In the present study, 2 cases of confirmed canine lycoperdonosis are described. The first case presented to the Matthew J. Ryan Veterinary Hospital of the University of Pennsylvania, and the second case was submitted for postmortem examination to the University of Tennessee Veterinary Teaching Hospital. Both dogs presented in respiratory distress, and owners reported that the dogs had been playing or digging in areas with puffball mushrooms prior to the onset of clinical signs. In the initial case, thoracic radiographs revealed a diffuse interstitial and multifocal alveolar pulmonary pattern. Despite aggressive medical treatment and mechanical ventilation, the dog continued to worsen and was euthanized. Postmortem examination revealed firm lung lobes and enlarged tracheobronchial lymph nodes. Histologically, there was a severe diffuse histiocytic and pyogranulomatous bronchointerstitial pneumonia. Throughout the lung and lymph nodes, most commonly within macrophages, were round, 3–5μm in diameter, Gomori methenamine silver—positive structures, consistent with Lycoperdon spores. An approximately 750–base pair DNA fragment was amplified from lung of both cases by polymerase chain reaction using primers specific to yeast ribosomal DNA, and the sequence of the fragment was determined to be most closely related to Lycoperdon pyriforme. Importantly, reexamination of an endotracheal wash from the initial case revealed intrahistiocytic spores, suggesti
Lycoperdon mushrooms, often termed puffballs, are found worldwide, and several species are found throughout North America and are considered edible when they are young and white. However, as they age, the mushrooms dry out, turn brown, and produce trillions of spores that are easily released when agitated, and the fruiting body eventually bursts. 8,9
Lycoperdonosis refers to respiratory disease resulting from the inhalation of Lycoperdon fungal spores. This disease entity has only rarely been reported in human beings. 11 The first 2 reported cases occurred in a child and an adolescent who had intentionally inhaled the spores as a homeopathic treatment for epistaxis. 14 Another case occurred in a 4-year-old after accidental exposure. 6 More recently, 8 teenagers from Wisconsin inhaled Lycoperdon perlatum spores at a party and within 1 week presented to local physicians with varying degrees of respiratory illness. 1 Clinical signs included a cough with shortness of breath, fever, and fatigue. Five of these individuals required hospitalization, and 2 needed to be intubated. Chest radiographs from all reported human cases of lycoperdonosis demonstrated bilateral, often nodular, infiltration of the lung, and lung biopsies from the recent cases revealed inflammation in the lung and structures consistent with Lycoperdon spores. All of the documented human patients with lycoperdonosis recovered after variable lengths of hospitalization, generally with steroid and/or antimicrobial treatment. 1,11
Recently, pneumonitis in a 12-year-old Golden Retriever dog in Canada that responded to corticosteroids was attributed to inhalation of puffball mushrooms. 13 This diagnosis was based largely on a history of the dog playing in a bed of these mushrooms as well as the presence of vacuolated structures within a transtracheal aspirate. The mushrooms in the environment were identified as Lycoperdon pyriforme; however, histopathology and molecular analysis of affected lung were not performed.
In the current report, the clinical progression and histopathology of 2 cases of confirmed fatal canine lycoperdonosis are described. A 1.5-year-old male neutered, fully vaccinated Shih Tzu dog presented to the Matthew J. Ryan Veterinary Hospital of the University of Pennsylvania (Philadelphia, Pennsylvania) due to a 3-day history of worsening respiratory distress despite antibiotic and prednisolone treatment by the referring veterinarian. The owner noted that the dog had been playing in an area with puffball mushrooms before the onset of clinical signs, but the extent of spore exposure was unknown. On presentation, the dog was tachypneic and afebrile with a pulse oximeter oxygen saturation of 78% on room air. The dog had a mild neutrophilia, and chemistry results were unremarkable. Thoracic radiographs revealed a diffuse interstitial pulmonary pattern with a more pronounced alveolar pattern peripherally and cranioventrally. Cytology from an endotracheal wash demonstrated suppurative inflammation and numerous extracellular bacteria, which were interpreted as either procedural contaminants or aspiration pneumonia. The dog was nonresponsive to oxygen therapy, broad-spectrum antibiotics, bronchodilators, mucolytics, and a short course of corticosteroids. After the endotracheal wash, the dog required mechanical ventilation but continued to exhibit severe respiratory decompensation and was, therefore, euthanized due to a poor prognosis.
The second case was a 5-year-old female spayed Cavalier King Charles Spaniel dog who was submitted to the University of Tennessee Veterinary Teaching Hospital (Knoxville, Tennessee) approximately 1.5 hr after death for postmortem examination. The dog presented to the referring veterinarian afebrile with an acute onset of tachypnea and cough. The owner reported that the dog was 1 of 4 dogs in the household with respiratory symptoms and that these 4 dogs were all “diggers” and that none of the “nondiggers” in the house were affected. Thoracic radiographs were attempted; however, the dog became agonal during the procedure and arrested.
Gross examination of the first case revealed a mild amount of serosanguineous fluid in the thoracic cavity and trachea. The lung lobes were dark red to purple and firm, and sections of all lobes sank in formalin. The tracheobronchial lymph nodes were enlarged, measuring approximately 5.0 cm × 1.5 cm × 2.0 cm. Similar lung lesions were observed in the second case; however, thoracic effusion and lymph node involvement were not prominent features. Additional significant gross lesions in the second case included deviation of the right-sided nasal turbinates, moderate tracheal cartilage dysplasia, mild mitral endocardiosis, moderate pancreatic atrophy, and cerebellar herniation with mild occipital dysplasia. On histologic examination, the bronchioles and large regions of the adjacent alveolar interstitium from both dogs were severely infiltrated by numerous macrophages (Fig. 1A, 1B). Although the predominant response was almost exclusively histiocytic, scattered regions had a pyogranulomatous infiltrate. Airway epithelial cells were often sloughed, and there was extensive type II pneumocyte hyperplasia along with frequent hyalinization of alveolar walls. Throughout all sections, macrophages occasionally contained 1–3, round, 3–5 μm in diameter spores. Spores were remarkably uniform and characterized by a thin brown wall and a clear to pale yellow center (Fig. 1B). The spores stained strong with both Gomori methenamine silver (Fig. 1C) and periodic acid—Schiff and were observed primarily within the cytoplasm of macrophages, although they were sporadically present extracellularly.
Bacteria were not observed in the lung of the first case on hematoxylin and eosin—or Gram-stained sections, suggesting that the bacteria observed in the endotracheal wash were an oral contaminant. In fact, reexamination of the cytospin from the wash revealed cytoplasmic spores within macrophages and rare extracellular spores that stained light green with modified Wright—Giemsa and were morphologically consistent with those observed by histopathology (Fig. 1D). The subcapsular and medullary sinuses of the tracheobronchial lymph nodes from the dog in the first case were markedly expanded by draining macrophages, and portions of the cortex were replaced by numerous macrophages and few neutrophils (Fig. 2). Remarkably, macrophages in the lymph node often contained the same spores observed in the lung (Fig. 2). In the second case, severe chronic widespread exocrine pancreatic acinar atrophy was confirmed via histopathology.
The morphology of the spores observed histologically was consistent with descriptions of Lycoperdon spores 2,8 ; however, lung histopathology from the most recent human cases attributed to Lycoperdon was not available for direct comparison. Polymerase chain reaction (PCR) was used to evaluate whether the affected lung tissue from these dogs contained Lycoperdon DNA. DNA was extracted from unstained sections of formalin-fixed, paraffin-embedded tissue, a and PCR was performed with a primer set initially derived from Cryptococcus neoformans that targeted the entire internal transcribed spacer (ITS) region between the large and small ribosomal RNA subunit genes. 7 Lung samples from both cases gave a PCR product of approximately 750 base pairs (bp) with the ITS 4/5 primer set (5′-TTCCTCCgCTTATTgATATgC-3′/5′p-ggAAgTAA AAgTCgTAACAAgg-3′). The PCR products were treated to remove single-stranded DNA and submitted to the University of Tennessee Molecular Biology Resource Facility for sequencing. Sequence reactions were performed with ITS primers in both directions. A BLAST search of the GenBank database (http://www.ncbi.nlm.nih.gov/blast/Blast.cgi) indicated that the best sequence match in both cases was to that of L. pyriforme (AY854075.1, strain AFTOL-ID-48) with nucleotide sequence similarity of 99% over 655 bp for case 1 and 99% over 682 bp for case 2. Other strong matches ranging from 97% to 100% sequence similarity were to shorter portions of sequences (<639 bp) from 12 different strains of L. pyriforme or Morganella pyriformis (current name). The next closest sequence similarities were at 90% or less to other Lycoperdon species.
It remains unclear whether the inflammatory reaction in cases of lycoperdonosis represents a reactive response to the presence of a foreign material, such as the spore, an allergic reaction, a response to an active fungal infection or toxin, or some combination of these processes. Fungal spores, particularly those smaller than 10 μm, are widely deposited in the lung after inhalation, and a study in hamsters demonstrated that spores 3 μm in diameter are displaced by surfactant in a specific manner that likely facilitates phagocytosis by macrophages. 3,4 The prevailing theory is that lycoperdonosis represents a hypersensitivity reaction to the spores and, therefore, has been most commonly termed a pneumonitits. 11 This disease likely shares features with hypersensitivity pneumonitis, also referred to as extrinsic allergic alveolitis, that refers to a bronchoalveolitis caused by repeated inhalation of specific antigens and, in part, involves a combination of type III and type IV reactions. 5,11 Hypersensitivity pneumonitis poses a significant occupational hazard to mushroom workers who are chronically exposed to mushroom spores; however, most reported cases of lycoperdonosis occurred after a single large inhalation, rather than repeated exposure. 10,12
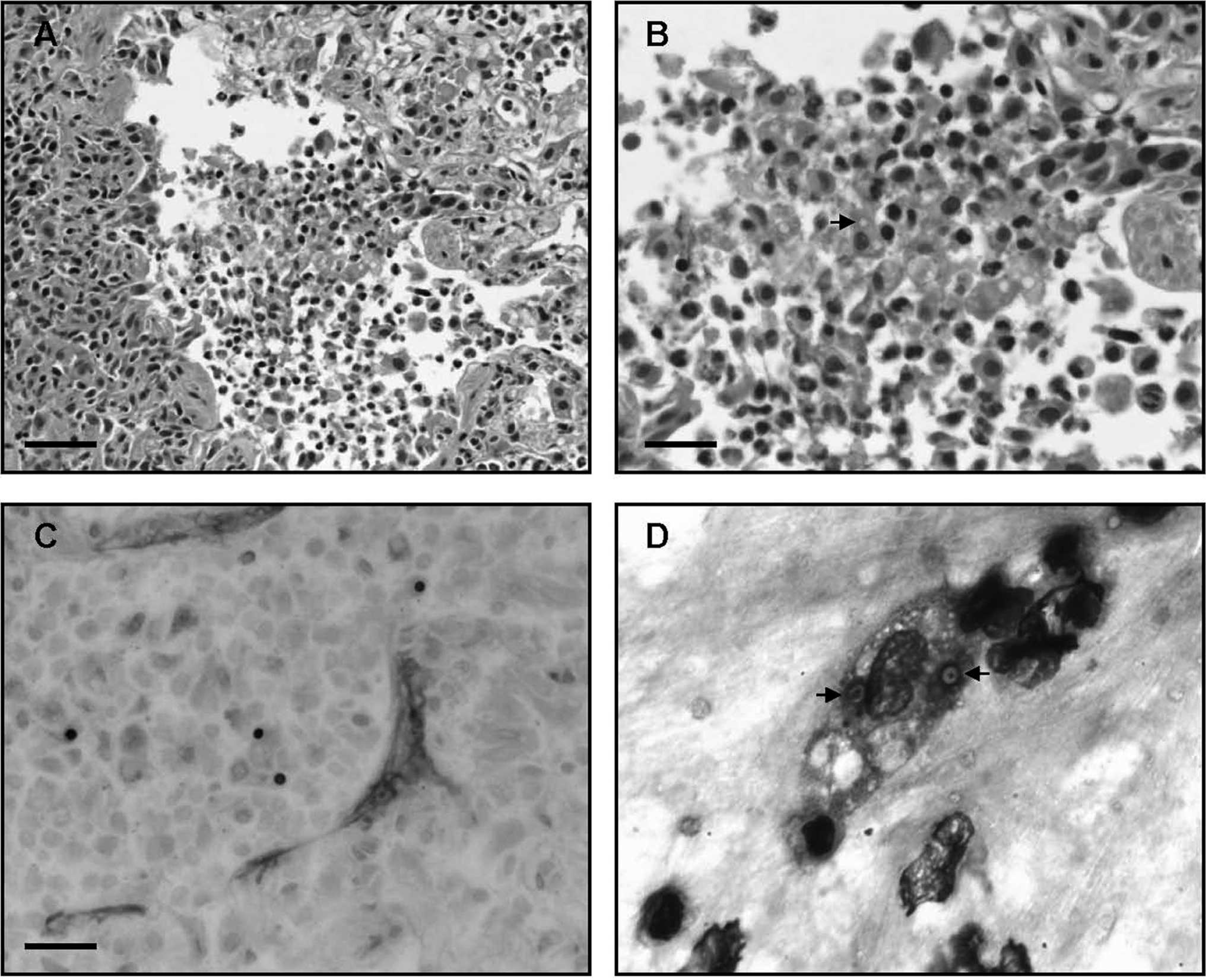
Lung, case 1.
The limited understanding of the nature of the inflammation in lycoperdonosis makes selection of therapeutics difficult. Steroids often exacerbate fungal infections, yet in most of the previously described cases, respiratory improvement was achieved after corticosteroid administration. 1,6,11,13 The effectiveness of steroids is highly supportive of the theory that lycoperdonosis represents a hypersensitivity reaction; however, in some of these cases, antifungals were also administered. 1 Interestingly, Lycoperdon has never been cultured from a reported case, 11 which further supports the likelihood that lycoperdonosis does not represent an active fungal infection. In fact, germination of mushroom fungal elements has never been reported in vivo and, due to warm body temperatures, is not believed to occur. 11
Anecdotal recollection of the level of human exposure suggests that there is a direct correlation between the amount of spores inhaled and the severity of the disease. 11 However, it is unknown to what extent immune status or concurrent disease plays a role in the disease severity. The second dog described herein was 1 of 4 dogs from the same breeder that had been exposed to the spores and had varying degrees of respiratory signs. All of the other dogs recovered without veterinary treatment. It is possible that this dog inhaled more spores, had a predisposition to developing a more severe immune reaction, or was less equipped to overcome the disease, possibly due to the concurrent exocrine pancreatic insufficiency. It is likely that several factors play a critical role in whether inhalation of these spores will be of clinical significance, cause a transient or persistent cough, or result in more severe disease that requires medical intervention or leads to death.
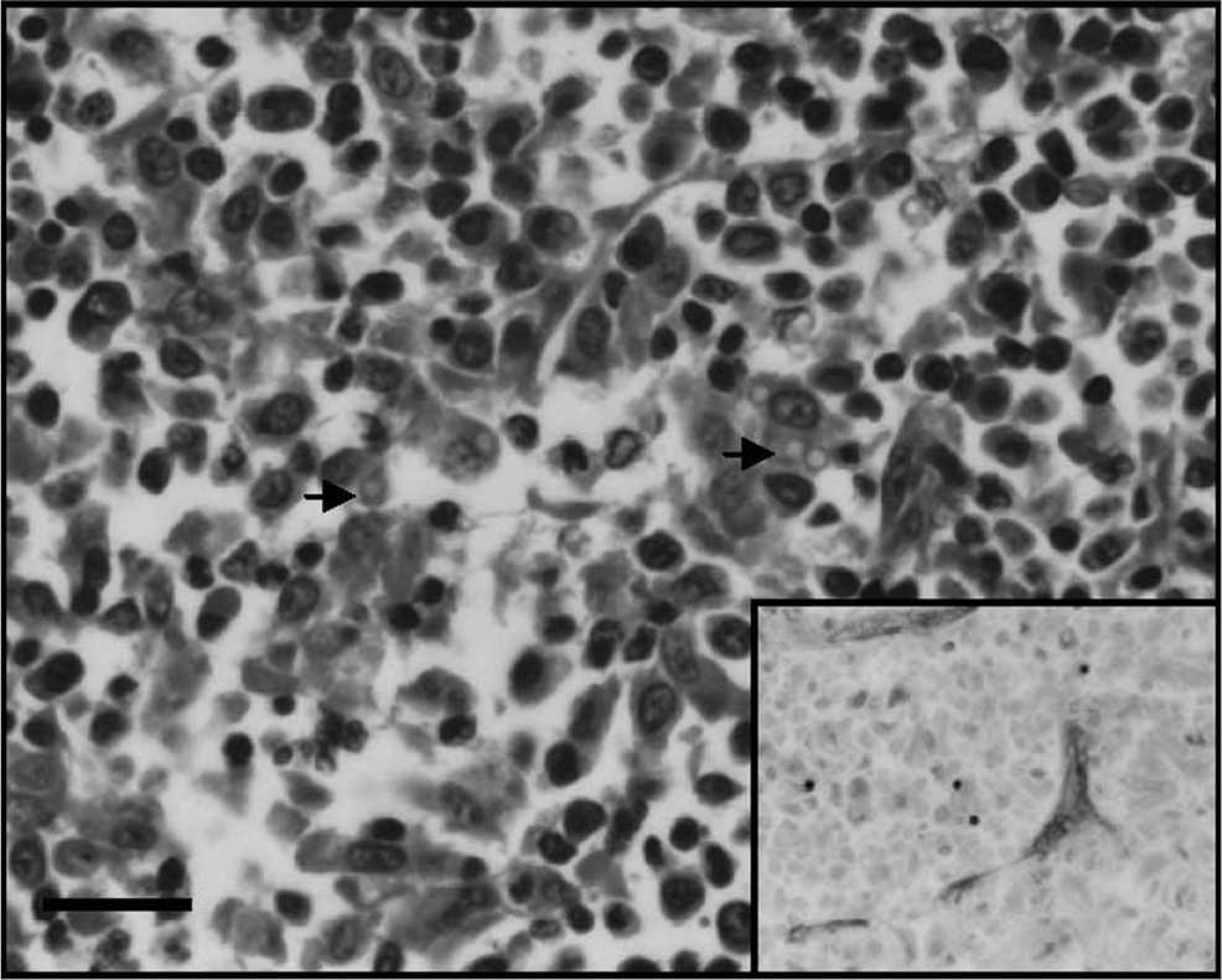
Tracheobronchial lymph node, case 1. Macrophages expand the subcapsular and medullary sinuses and multifocally infiltrate the lymph node. Macrophages in the lymph node often contain intracytoplasmic spores (arrows) with the same morphology as those in the lung. Hematoxylin and eosin. Bar = 25 μm. Inset: Gomori methenamine silver stain of fungal spores.
Due to the scarcity of described lycoperdonosis cases in both human and veterinary medical literature, the relevance and potential severity of puffball exposure may be overlooked. However, puffballs are common worldwide and should be considered as possible causative agents in cases of pneumonia or pneumonitis in domestic animals.
In both of the cases described herein, owners noted that the dogs had been playing or digging in regions known to have mushrooms. When an animal presents with respiratory illness and this type of exposure history, particularly when the patient is not responding to antimicrobials, lycoperdonosis should be considered a significant differential, and airway and biopsy samples should be evaluated closely for spores.
Acknowledgements. The authors are grateful to Rupal A. Brahmhatt for her assistance with the polymerase chain reaction identification.
Footnotes
a.
Qiagen Inc., Valencia, CA.