
Abstract
In humans, diabetes mellitus (DM) is an important cause of renal damage, with glomerular lesions being predominant. In cats, although diabetes is a common endocrinopathy, it is yet unknown whether it leads to renal damage. The aim of the study was to compare renal histologic features and parameters of renal function in diabetic cats against a control population matched for age, gender, breed, and body weight. Thirty-two diabetic and 20 control cats were included. Kidney sections from paraffin-embedded kidney samples were stained and examined with optical microscopy to identify glomerular, tubulointerstitial, and vascular lesions and to assess their frequency and severity. Serum creatinine and urea concentrations were also compared. Glomerular lesions were observed in 29 cats overall, with mesangial matrix increase being more common (19 cats). Tubulointerstitial lesions were observed in 42 cats, including lymphocytic infiltration (29), fibrosis (22), or tubular necrosis (21). Vascular lesions were observed in 5 cases. The frequency and severity of histologic lesions did not differ between diabetic and control cats; however, among diabetics, those that survived longer after diagnosis had more glomerular and vascular lesions. Serum creatinine and urea concentrations were similar between groups; in diabetic cats median creatinine was 109 μmol/l (range, 51–1200) and urea was 12 mmol/l (range, 4–63), and in controls creatinine was 126 μmol/l (range, 50–875) and urea 11 mmol/l (range, 3–80). The results suggest that DM in cats does not lead to microscopically detectable kidney lesions or clinically relevant renal dysfunction. The authors hypothesize that the short life expectancy of diabetic cats may be the main reason for the difference from human diabetics.
Diabetes mellitus (DM) is a frequent endocrine disease in cats. 17 Diabetic cats may develop chronic kidney disease (CKD), but it is unknown whether DM causes renal damage. 4 At our institution, it was observed that 4 of 30 (13.3%) cats with newly diagnosed DM developed CKD during the first 6 months of therapy. 12 In 2 recent investigations, 26% of insulin glargine–treated diabetic cats and 63% of insulin detemir–treated diabetic cats developed CKD during the frame of the study, respectively. 19,20 In survival analyses of diabetic cats, renal failure was diagnosed in approximately 20% at the time of diagnosis 5 and was the cause of death in 17% of cases. 14 Unfortunately, none of these investigations included a control group of nondiabetic cats to identify a possible association between DM and kidney injury.
The only studies comprising control cats reported inconsistent findings. In particular, in 1 study diabetic cats did not have lower glomerular filtration rate, higher proteinuria, or more tubular dysfunction than healthy controls. 16 In another study, diabetic cats were more likely to have microalbuminuria or urine protein to creatinine ratio >0.4. 2 In both studies control groups were matched for age, but it is unknown whether other variables, such as gender, breed, and body weight, were evenly distributed; slight matching variations may have explained the results differences.
With regard to kidney histopathology, we are only aware of a single investigation that has been published on diabetic cats. Of the 6 included cases, documented microscopic findings were increased mesangial matrix in 2, glomerular sclerosis in 1, and tubulointerstitial inflammation in 1 cat. 15
In humans, DM is the most important cause of renal damage. Diabetic nephropathy occurs in approximately 30% of people with either type 1 or 2 DM. 18 The main histological lesions include thickening of the glomerular basement membrane, mesangial expansion, and mesangial nodules, while tubular atrophy and vascular hypertrophy are less frequent. 1,10
Because the association between DM and kidney injury is yet unclear and there is paucity of histopathological data, the aim of this retrospective study was to compare renal microscopic features in diabetic cats against a well-matched control population. In addition, associations between renal lesions and parameters of renal function, including serum creatinine and urea concentrations, were investigated.
Materials and Methods
Cases and Controls
Cats with diabetes mellitus that died at the Clinic for Small Animal Internal Medicine, University of Zurich (Switzerland) between 1997 and 2009 and in which a postmortem examination was performed were included in the study if kidney samples of sufficient size were available. From the same institution and during the same corresponding period, cats that died due to any disease with available kidney samples and similar to diabetic cats for age, gender, breed, and body weight were considered; from this population control cats were randomly selected. In addition, laboratory data regarding serum creatinine and urea concentrations were collected from medical records if they had been measured within a month before death.
Histopathology and Scores
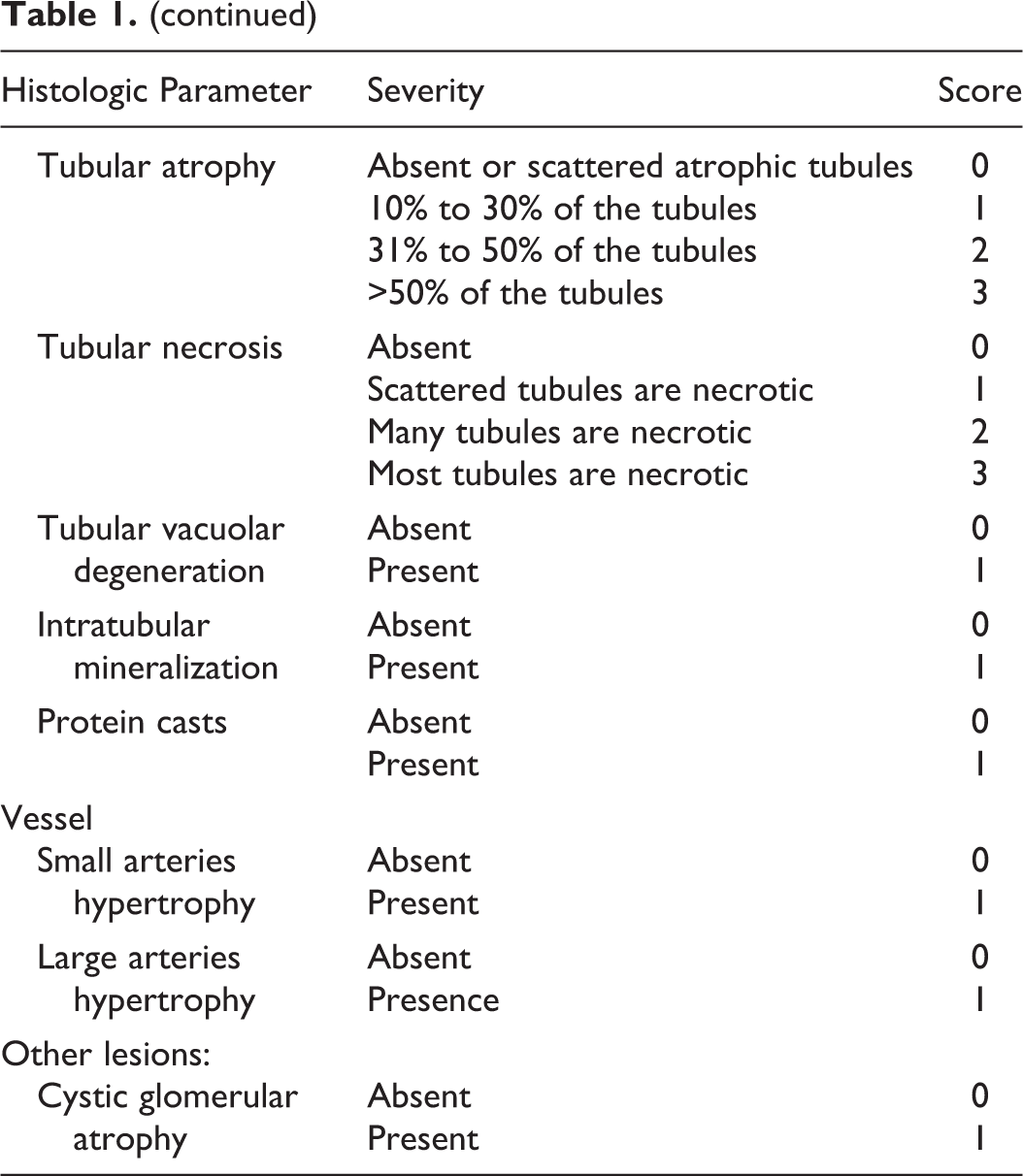
For renal histopathology, 10% neutral buffered formalin-fixed, paraffin-embedded samples of approximately 1.5 cm in width and 1 cm in height were cut to obtain slides comprising cortex and medulla. Five serial 3-µm kidney sections were stained with haematoxylin and eosin (HE), periodic acid-Schiff (PAS), Masson’s trichrome, acid fuchsine orange-g (AFOG), and periodic acid methenamine silver (PAMS). Slides were evaluated using light microscopy for the presence of glomerular, tubulointerstitial, and vascular lesions. For lesions of the 3 compartments, a dichotomous grading system of 0 (ie, no lesion) and 1 (ie, any lesion) or a tie-grade system from 0 to 3 was used, as recently described. 3 Lesions included in the analysis and score definitions are listed in Table 1. In addition, the percentage number of obsolescent glomeruli and the combined glomerular score, as proposed by Chakrabarti and coworkers, 6 were calculated. All kidney sections were assessed by 2 pathologists (L. Aresu, S. Benali) in a blinded fashion without knowledge of the clinical data; any interobserver discrepancy in grading was resolved by consensus.
Histologic Scoring of Renal Biopsy Specimens.
Statistical Analysis
Adequacy of matching of diabetic and control cats was assessed for age, gender, breed, and body weight with Fisher’s exact test and Mann-Whitney test. Comparison between frequencies of glomerular, tubulointerstitial, and vascular lesions in the 2 groups was performed with Fisher’s exact test considering a score of 0 for each parameter if no lesions were observed and a score of 1 if any lesion was documented. The analysis was also performed with r × c contingency tables for parameters with scores from 0 to 3, if sufficiently represented for statistical analysis. Differences between the percentage number of obsolescent glomeruli and the combined glomerular score in diabetic and control cats were evaluated with Mann-Whitney tests. The same test was used to compare concentrations of serum creatinine and of urea in the 2 groups. To compare frequencies of cats with serum creatinine and urea above the reference range, the Fisher’s exact test was used. Furthermore, associations between glomerular, tubulointerstitial, and vascular lesions and between serum creatinine or urea and histologic parameters were tested with contingency tables in all cats grouped together; analyses were performed if a sufficient number of cases per lesion were present. Fisher’s exact test was also used to identify associations between renal lesions and survival of diabetic cats. Significance was considered for P < .05.
Results
Cats
Thirty-two diabetic cats and 20 controls were included in the study. Diabetic cats had median age of 11 years (range, 2–18), 23 (71.9%) were neutered male and 9 (28.1%) spayed female, and median body weight was 4.9 kg (range, 3.8–10.0). Twenty-five (78.1%) cats were cross breed and 7 (21.9%) were pure breed, including 2 Siamese and Maine Coon each and 1 Chartreux, Oriental shorthair, and Russian Blue each. Concurrent disorders at death were recorded in 19 (59.4%) diabetic cats and included 3 each with chronic hepatitis and severe chronic renal failure; 2 each with chronic enteritis, chronic stomatitis, liver lipidosis; and 1 each with acute enteritis, asthma, hyperthyroidism, idiopathic epilepsy, idiopathic hypercalcemia, megacolon, and multicentric lymphoma. Control cats had median age of 12 years (range, 2–17), 14 (70.0%) were neutered male and 6 (30.0%) were spayed female, and median body weight was 4.3 kg (range, 2.5–9.0). Seventeen (85.0%) cats were crossbreeds and 3 (15.0%) were pure breed, including 2 Chartreux and 1 British shorthair. Disorders recorded at death were in 3 chronic hepatitis; in 2 each hypertrophic cardiomyopathy, meningioma, and severe chronic renal failure; and in 1 each acute enteritis, colon carcinoma, fibrosarcoma, hyperthyroidism, immune-mediated anemia and thrombocytopenia, liver carcinoma, liver lipidosis, lung carcinoma, multicentric lymphoma, pneumonia, and restrictive cardiomyopathy. Differences were not observed between the 2 groups for age, gender, breed, and body weight.
Histopathology: General Assessment
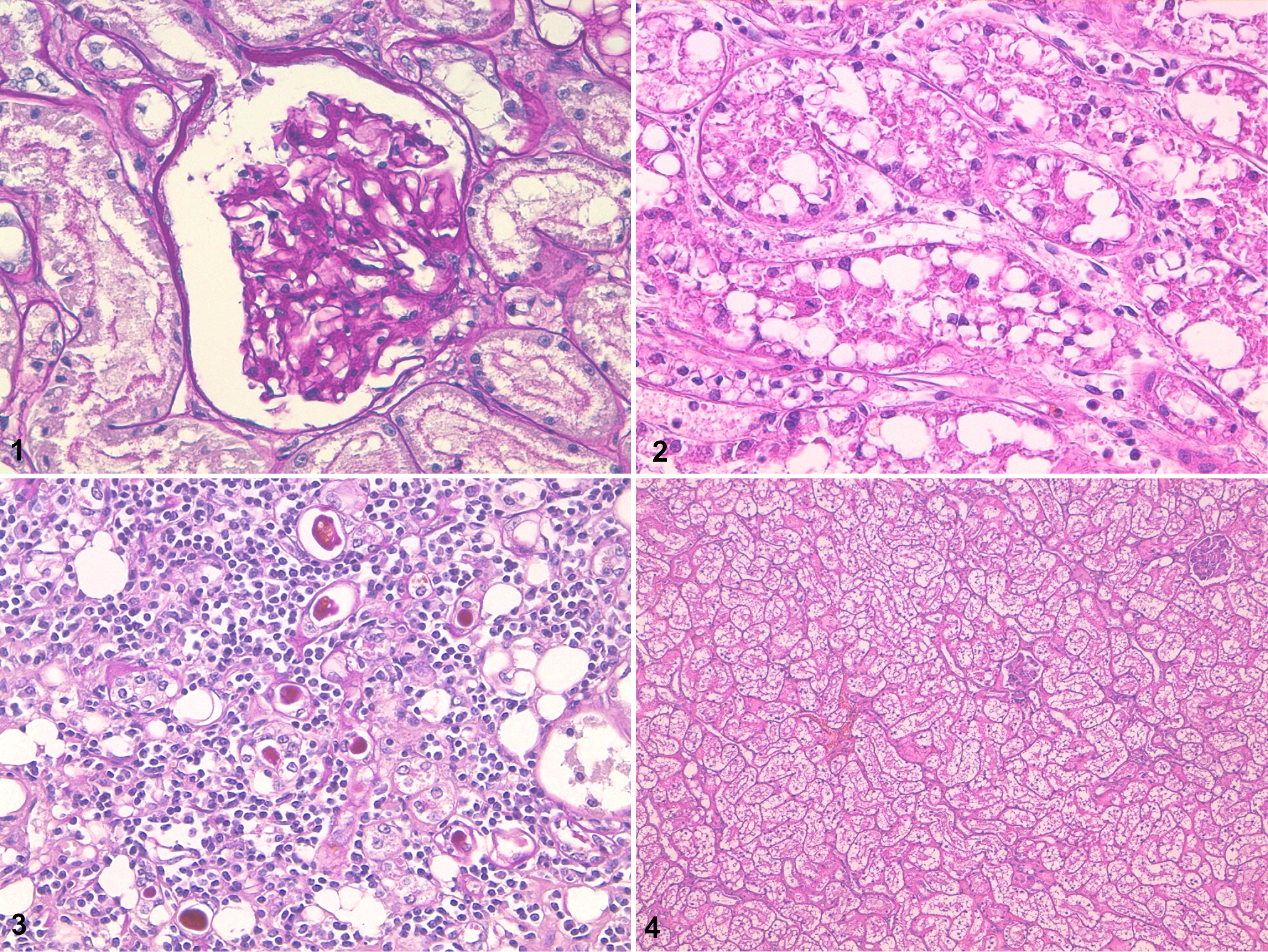
Single or multiple glomerular lesions were observed in 29 cats, including 17 (53.1%) cats with DM and 12 (60.0%) controls. In both groups the most frequent glomerular lesion was segmental to diffuse mesangial matrix increase (Fig. 1), occasionally associated with obsolescent glomeruli (Table 2). Other changes were rarely identified and included thickening of the glomerular basement membranes, mesangial cell interposition, periglomerular fibrosis, thickening of the Bowman’s capsule, mesangial hypercellularity, cystic glomerular atrophy, mesangiolysis, and parietal epithelium and podocytes hypertrophy. Mesangial nodules, or Kimmelstiel-Wilson nodules, typically associated with diabetes in humans were not documented in diabetic cats. 10
Renal Lesions in Cats: Number of Cases and Frequency Comparison.a
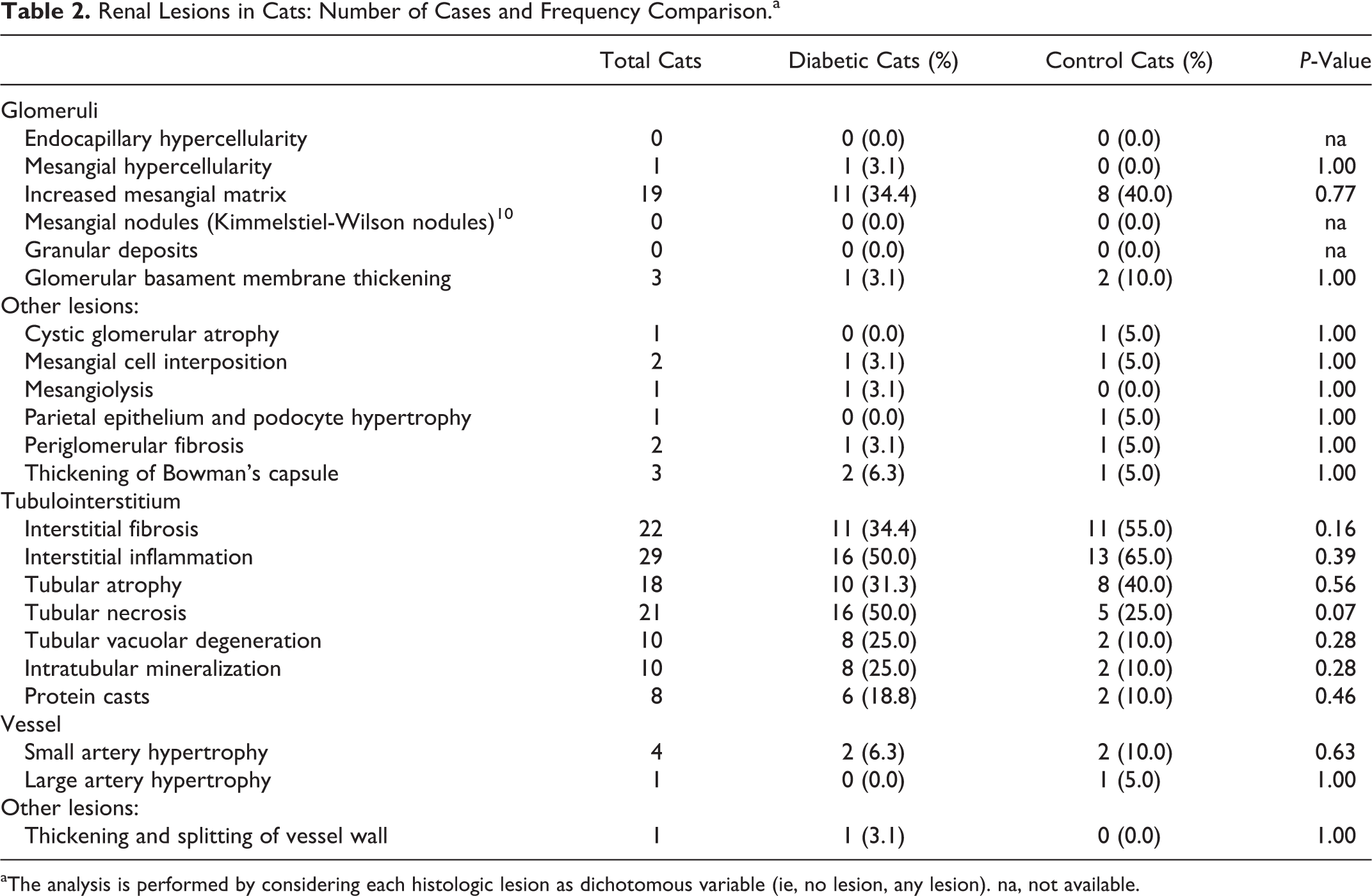
aThe analysis is performed by considering each histologic lesion as dichotomous variable (ie, no lesion, any lesion). na, not available.
The tubulointerstitial compartment was affected in 42 cats, with 26 (81.3%) diabetic and 16 (80.0%) control cats showing lesions suggestive of an acute or chronic process and variable degree of severity. Interstitial lymphocytic infiltration was found in 29 cats (16 diabetics and 13 controls), with 4 of them (2 in each group) also having interstitial plasma cells (Table 2). In 21 cats (16 diabetics and 5 controls), multifocal acute tubular necrosis was identified (Fig. 2), often associated with intratubular dystrophic mineralization. In 22 cases (11 diabetics and 11 controls), the interstitium was mildly to moderately expanded by multifocal proliferation of fibroblasts and collagen deposition (interstitial fibrosis). Occasionally interstitial fibrosis extended radially from the cortex throughout the medulla; within these areas multifocal atrophic tubules were observed (Fig. 3). Tubular vacuolar degeneration was diffuse and markedly severe in 10 cats (8 diabetics and 2 controls) (Fig. 4). In these cases tubular epithelial cells were characterized by a micro- and macrovacuolated light cytoplasm.
Lesions involving the vessels were observed in 5 cases, including 3 (9.4%) diabetic and 2 (10.0%) control cats. Small artery hypertrophy was detected in 4 cats, with 1 of them (control cat) also having large artery hypertrophy; in another (diabetic cat) thickened and split vessel walls were observed (Table 2).
With regard to histologic parameters scored from 0 to 3, their degree of severity was mostly 1 or 2 and in only few cases was 3. The score 3 was given to 1 control cat each for increased mesangial matrix and interstitial inflammation, to 1 cat per group for interstitial fibrosis and tubular atrophy, and to 4 diabetic cats for tubular necrosis.
Histopathology: Comparison Between Groups and Associations Between Lesions
Statistical comparison for each histologic parameter of the glomerular, tubulointerstitial, and vascular compartment considered as dichotomized variable (ie, no lesion vs any lesion) yielded no differences between diabetic and control cats (Table 2). Of note, tubulointerstitial necrosis tended to be more frequent in cats with diabetes, with the lesion observed in 50.0% of diabetic cats and in 25.0% of controls (P = .07). The analysis for histologic parameters with scores from 0 to 3 was performed for increased mesangial matrix, interstitial fibrosis, interstitial inflammation, tubular atrophy, and tubular necrosis. Scores were not differently represented for the listed glomerular and tubulointerstitial lesions. The median of obsolescent glomeruli was 1% in diabetic cats (range, 0–24) and 7% in controls (range, 0–48); statistical analysis showed a trend toward lower values in the former group (P = .06). The combined glomerular score was similar in the 2 groups (diabetic cats: 0, range, 0–2; control cats: 0, range, 0–3; P = .62).
Because of the low frequency of many glomerular and vascular lesions, associations between renal lesions were studied in all cats grouped together. Regarding glomerular lesions, increased mesangial matrix and obsolescent glomeruli were included in the analysis; all tubulointerstitial lesions were included and vascular lesions were not studied. Among tubulointerstitial lesions, an association was observed between the presence of inflammation and fibrosis (94.4% cats with fibrosis had inflammation vs 33.3% cats without fibrosis; P < .001) or tubular atrophy (100% cats with tubular atrophy had inflammation vs 33.3% cats without tubular atrophy; P < .001), between fibrosis and tubular atrophy (93.8% cats with tubular atrophy had fibrosis vs 9.1% cats without tubular atrophy; P < .001), and between tubular necrosis and protein casts (100% cats with protein casts had tubular necrosis vs 35.7% cats without protein casts; P = .02). Associations between glomerular lesions and between glomerular and tubulointerstitial lesions were not documented.
Serum Creatinine and Urea: Comparison Between Groups and Association With Histopathology
Creatinine and urea concentrations did not differ between groups. In diabetic cats, median creatinine concentration was 109 μmol/l (range, 51–1200) versus 126 μmol/l in controls (range, 50–875) (P = .97). Seven of 30 (23.3%) diabetic cats and 6 of 19 (31.6%) controls had creatinine above the reference range (98–163 μmol/l). According to history and physical exam findings, the 13 cats with elevated serum creatinine were diagnosed with chronic kidney disease. Based on IRIS staging of chronic kidney disease (http://www.iris-kidney.com), 11 had mild to moderate increase of creatinine (<440 μmol/l) and 2 had severe increase (>440 μmol/l). None had a diagnosis of acute renal failure. The severity of azotaemia did not help to make distinction between acute and chronic renal failure, including cases with acute exacerbation of chronic disease. In diabetic cats, median urea concentration was 12 mmol/l (range, 4–63) versus 11 mmol/l in controls (range, 3–80) (P = .96). Fifteen of 30 (50.0%) diabetic cats and 8 of 19 (42.0%) controls had urea above the reference range (7–13 mmol/l). The frequency of cats with increased creatinine or urea above reference did not differ between groups (creatinine, P = .53; urea, P = .77).
Because no differences were observed between diabetic and control cats for serum markers of renal function and because of the low frequency of most histologic parameters, associations between serum creatinine or urea and glomerular or tubulointerstitial lesions were studied considering all cats grouped together. An association was observed between increased creatinine concentration and the presence of renal interstitial fibrosis (P = .01); 10 of 13 (76.9%) cats with increased creatinine had interstitial fibrosis and 3 of 27 (11.1%) cats without interstitial fibrosis had increased creatinine. No association was identified between creatinine and the other histologic lesions of the tubulointerstitial or glomerular compartment. Associations were not documented between increased serum urea concentration and histopathology.
Survival of Diabetic Cats, Glycemic Control, and Association With Histopathology
Median survival of the 32 diabetic cats, calculated from diagnosis, was 199 days (range, 1–1470), with 8 (25.0%) of them living longer than 365 days. The median age of the subgroup of 8 diabetic cats with longer survival was 12 years (range, 10–18) and that of the remaining cats was 11.5 years (range, 2–17); age did not differ between subgroups. In the subgroup of diabetic cats with longer survival, 7 had glomerular lesions, 7 had tubulointerstitial lesions, and 3 had vascular lesions. Glomerular lesions were more frequent in the subgroup of diabetic cats that survived longer (P = .04), whereas tubulointerstitial lesions were similarly represented. Vascular lesions were only documented in this subgroup. Median age of the subgroup of diabetic cats that lived longer did not differ from that of control cats.
Data on glycemic control were retrieved from the clinical records of 22 diabetic cats. Four (18.2%) cats had good glycemic control, as defined by fructosamine concentrations <500 µmol/l (reference range, 200–340) throughout treatment, and the remaining 18 (81.8%) cats had poor glycemic control. Of the 4 cats with good glycemic control, 2 had glomerular lesions, 3 had tubulointerstitial lesions, and none had vascular lesions. Of the 18 cats with poor glycemic control, 8 had glomerular lesions, 14 had tubulointerstitial lesions, and 2 had vascular lesions.
Discussion
Renal lesions are understudied in diabetic cats, and no data are available to assess whether specific histologic changes suggestive of diabetic nephropathy exist. Results of the present investigation indicate that DM in cats does not lead to more microscopically detectable renal lesions in the glomeruli, tubulointerstitium, and vessels than in a well-matched control group. In addition, clinically relevant renal dysfunction is not more frequent in diabetic cats than in matched controls.
With regard to glomerular findings, the most frequent lesion was increased mesangial matrix, identified in 34.4% of diabetic and in 40.0% of control cats. The frequency and degree of severity did not differ significantly between the 2 groups. Expansion of the mesangial matrix is a hallmark of humans with either type 1 or 2 DM and diabetic nephropathy. 1,10 Hyperglycemia directly increases mRNA expression and synthesis of fibronectin and collagen by mesangial cells; progressive increase of the extracellular matrix occludes glomerular capillaries, contributing to the development of chronic renal failure in up to 30% of diabetic humans. 1,9,18 In some affected humans, light microscopic changes of glomeruli include nodular lesions consisting of areas of marked expansion of the mesangium forming large round fibrillar zones lined by palisading of mesangial nuclei (Kimmelstiel-Wilson nodules). 10 None of the diabetic cats in our study with an increase in the mesangial matrix presented these characteristic nodules.
In the cats of the present study all other glomerular lesions were scant, with only individual cases documented, and were not represented more often in diabetics than controls. Apart from the increased mesangial matrix, thickening of the glomerular basement membrane is most frequent in humans with diabetic nephropathy. 1,10 This lesion was reported in only 1 diabetic cat and in 2 controls. Thus, differently from humans, DM in cats does not seem to cause marked glomerular lesions. A possible explanation of the difference between human diabetes and diabetic cats might be the shorter life span of cats, as compared to humans. Indeed, glomerular lesions may occur approximately 15 years after diagnosis in diabetic humans, whereas median survival of the present diabetic cats was only of approximately 6 months. In addition, glomerular and vascular lesions were documented more often in diabetic cats that lived longer than 1 year. Therefore, these findings suggest that in most cats the timeframe may not be long enough to cause nephropathy.
Of note, the analysis of the glomerular compartment revealed that the number of obsolescent glomeruli tended to be lower in diabetic cats (P = .06). The reason for this finding is unclear and deserves further investigation. Even though all other glomerular lesions were not more frequent, DM is unlikely to exert protective effects on cat glomeruli. Indeed, in diabetic humans the number of obsolescent glomeruli increases, in particular with longer disease duration.
Overall, tubulointerstitial lesions were much more common than those affecting the glomeruli in cats (42 vs 29), and interstitial inflammation or fibrosis and tubular necrosis were most frequently represented. Interestingly, however, and similar to the glomeruli, the frequency and degrees of severity were comparable between diabetic and control cats. Only the prevalence of tubular necrosis tended to be higher in diabetic cats, with 50.0% showing the lesion in contrast to 25.0% of control cats (P = .07). In addition, 4 diabetic cats with necrosis had the maximum degree of severity (score 3) as opposed to none in the controls. Humans with diabetic nephropathy may have lesions in the tubulointerstitial compartment, but they are less frequent and with lesser degree of severity as compared to glomeruli, unless end-stage kidney disease is observed. 11 Among changes observed in humans with diabetic nephropathy, interstitial fibrosis and tubular atrophy are more common, and they are mainly secondary to glomerular damage. 10,25 Thus, because diabetic cats do not show glomerular changes, absence of tubulointerstitial lesions was expected.
Glycosuria may also contribute in the pathogenesis of tubulointerstitial damage. Human tubular cells are sensitive to glucotoxicity, and cell death may occur after exposure to elevated glucose concentrations, such as during poorly controlled hyperglycemia and severe glycosuria. 24 Whether necrosis of tubular cells might have been related to poorly controlled glycemia in the cats of our study is unclear. Data on glycemic control were retrieved from the clinical records of 3 of the 4 diabetic cats with tubular necrosis given a score 3 (data not shown); all 3 cats had poor glycemic control throughout treatment. Information on glycemic control were also collected from 7 of the remaining 12 diabetic cats with tubular necrosis and scores 1 or 2; 5 cats had poor and 2 had good glycemic control throughout treatment. These results do not clearly indicate that tubular necrosis is associated with poor glycemic control in diabetic cats. Overall, data on glycemic control were retrieved from 22 diabetic cats. Renal lesions were documented in cats with and without good glycemic control. Additional studies are necessary to verify a potential causal relationship between uncontrolled diabetes and kidney damage.
Lesions of the vascular compartment were infrequent in the present cats, and as observed for the glomeruli and tubulointerstitium, they were similarly represented in diabetic and control cats. Of note, however, in diabetic cats vascular lesions were only documented in cats with longer duration of diabetes, possibly suggesting that vessels may be a target organ for diabetic complications in the long term. In humans with diabetic nephropathy, hypertrophy of small and large arteries is common and is thought to be caused by hypertension and concurrent endothelial dysfunction. 7,9 The reason for the low prevalence of vascular changes in the kidneys of diabetic cats may arise from the fact that survival is not long enough for developing renal lesions and, possibly, that hypertension is unusual during DM in this species. Indeed, concerning the latter, a study performed in 14 diabetic cats found no evidence of hypertension based on systolic blood pressure measurement and ophthalmic evaluation in any of them. 22 In another study including 66 diabetic cats, mean systolic blood pressure was higher in cats with DM than in controls, but the prevalence of hypertension (>160 mm Hg) was not different between groups (diabetic cats, 15%; controls, 9%). 2 Unfortunately, data regarding blood pressure measurement were not available from clinical records of the present diabetic cats.
Serum concentrations and percentage increase of creatinine and urea were similar in diabetic and control cats. Although these markers may not be sensitive enough to early detect differences in renal function, in particular if the glomerular filtration rate is not decreased by more than 70% to 75%, 8 comparable values between groups were expected because histologic lesions of all examined compartments did not differ.
In addition to the comparison of kidney morphology and function of diabetic and control cats, results of the present study allowed the investigation of associations among renal lesions and between damage and parameters of function, in general. Strong positive associations were observed among tubulointerstitial inflammation, tubulointerstitial fibrosis, and tubular atrophy; this may suggest that the 3 lesions represent different stages or parts of a common pathophysiological event in cats, as described in humans. 13 In addition, a positive association was also found between tubular necrosis and tubular protein casts, probably due to the fact that necrotic cells reach the tubular lumen after detachment from the basement membrane. To the authors’ knowledge, a single study with 80 cats, including CKD and non–renal diseases, investigated the relationships between structural lesions of the kidneys. 6 Similar to our findings, tubulointerstitial inflammation and fibrosis were positively associated; tubular atrophy and protein casts were not evaluated. From our study, an association was found between tubulointerstitial fibrosis and increased serum creatinine. Similar structural-functional findings have been reported in cats. 6 Thus, our study confirms that tubulointerstitial fibrosis is a strong predictor of renal function in cats, as has been described in humans with a variety of nephropathies. 21
Some limitations of the study need to be mentioned. The evaluation of renal lesions was based on light microscopy and it cannot be excluded that ultrastructural changes would have been identified more often in diabetic cats with the use of transmission electron microscopy. The number of cats included might not have been enough to identify group differences, in particular considering the low prevalence of glomerular and vascular lesions. In addition, the control group included cats collected from the same faculty, and the particular scientific interests of the institution may affect the types of diseases the control cats may have suffered from, possibly introducing a bias in the pathologies observed in the kidneys of these cats. Moreover, we had to rely on serum creatinine and urea concentrations that were collected during the month prior to death. It is therefore possible that some values would have differed if obtained few days before death, perhaps modifying the results of the analysis. Furthermore, creatinine and urea do not represent sensitive markers to characterize glomerular filtration rate; hence, iohexol or exogenous creatinine clearance, although not routinely used in clinical practice, would have provided more precise information about renal function in cats. 23 Finally, although the current literature suggests that hypertension does not occur in diabetic cats and the presence of proteinuria is doubted, 2,16,22 the lack of blood pressure measurement and the lack of urine protein loss quantification represent important limitations; the retrospective nature of the study did not allow us to thoroughly investigate the effect of diabetes on blood pressure and proteinuria.
In summary, DM in cats does not cause microscopic lesions suggestive of kidney damage in the glomerular, tubulointerstitial, and vascular compartments or clinical evidence of renal dysfunction that go beyond those observed in a matched control population. The shorter life expectancy of diabetic cats may be responsible for the difference to human diabetics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was partially supported by a grant from the Policlinico di Monza, Italy. The Policlinico di Monza, Italy, for the work represented.