
Abstract
Verrucous hemangiomas are a rare specific variant of equine skin tumors not well described in the literature. An 8-year-old gelding presented a unilateral lesion on the pastern. Macroscopically, the mass showed a warty and verrucous surface with focal ulcerations. The histology showed a dermal proliferation of endothelial-layered capillaries and venules separated by a delicate stroma of scant fibroblasts and collagen deposition, with pseudoepitheliomatous hyperplasia (exuberant reactive irregular epithelial hyperplasia with tongue-like projections extending into the dermis, mimicking downgrowth of squamous cell carcinoma) and orthokeratotic hyperkeratosis of the overlying epidermis. The immunohistochemical study confirmed the endothelial origin of the tumor, and a final diagnosis of verrucous hemangioma with pseudoepitheliomatous hyperplasia was confirmed. To the knowledge of the authors, this is the first detailed description of this entity in adult horses. Moreover, the clinical progression and epidermal changes have not been previously reported, emphasizing the importance of a pathological study of any epithelial preneoplastic lesion to rule out an underlying dermal neoplasia.
The current classification of tumors and malformations of vascular tissues in horses is difficult due to the frequent overlap of terms. Benign neoplasia of blood vessel endothelium or hemangioma is an uncommon equine skin neoplasia, characterized by a solitary, well-circumscribed, reddish gray to pink, soft pedunculated nodular mass mainly located in the distal limbs. 6 This lesion may acquire a plaque-like, dark, warty appearance, known as verrucous hemangioma. 11 This neoplasm has no breed or sex predisposition but is particularly frequent in horses younger than 1 year, which suggests a congenital origin. 10 Surgical removal may be successful, but recurrence is not rare. Verrucous hemangioma is an uncommon capillary or cavernous hemangioma with reactive epidermal changes of hyperkeratosis, acanthosis, and papillomatosis. 11 Preneoplastic and neoplastic lesions may present marked epithelial changes that may lead to a misdiagnosis if the sample is not thoroughly inspected. 6,8 We describe here a verrucous hemangioma with pseudoepitheliomatous epidermal hyperplasia in an adult horse and discuss the differential diagnoses to be considered.
An 8-year-old Andalusian gelding was presented to the Veterinary Hospital of the University of Cordoba with a unilateral insidious lesion on the plantar aspect of the right hindlimb pastern. The horse did not present pain, and the lesion was nonpruritic. The growth presented an evolution of 2 years, being characterized by a slow growth and persistent episodes of progression and involution without a seasonal pattern. Macroscopically, the mass was 10 × 3 cm in size and showed a warty and verrucous surface with a brown color associated with hyperpigmentation and focal ulcerations (Fig. 1). A loosely demarcated firm nodular mass beneath the epidermal thickening expanding to deeper skin planes was noted on palpation. No other finding was evident. A punch biopsy was obtained and submitted to the Veterinary Pathology Service.
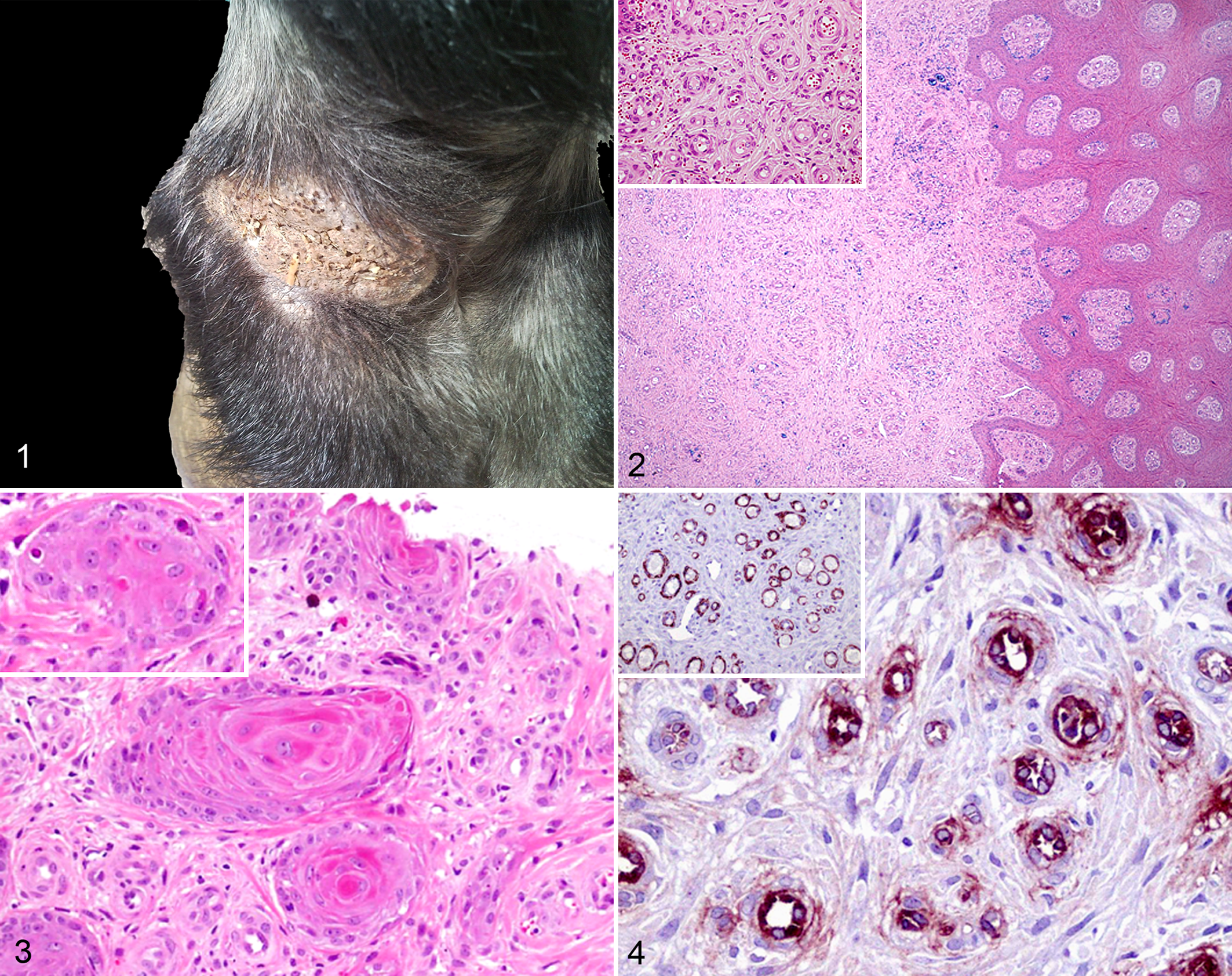
Microscopically, a nonencapsulated nodular mass expanding from the dermis-epidermis interface to the deep dermis and superficial subcutaneous tissue was observed. The mass corresponded to a proliferation of thin endothelial-layered capillaries and venules, some of them filled with blood, separated by scant stroma with a low number of fibroblasts and some areas of collagen deposition (Fig. 2). Inflammatory infiltrate was inconspicuous and consisted mostly of small lymphocytes and scattered plasma cells. No blood-filled cavernous dilations or abnormal ecstatic thin vessels were observed in the tissue. The vascular spaces were lined by typical endothelial cells with plump oval nucleus and scant cytoplasm, without cellular atypia, mitosis, or signs of malignancy (Fig. 2, inset). In the periphery of some vascular spaces, 1 to 3 concentric layers of elongated to spindle cells with a faint eosinophilic cytoplasm and larger euchromatic nuclei were evident, but no smooth muscle layer was observed surrounding the endothelium (Fig. 2, inset).
The overlying epidermis showed small foci of ulceration and an orthokeratotic hyperkeratosis, acanthosis, and rete ridges formation along with areas of pseudoepitheliomatous epidermal hyperplasia (Fig. 2). Most of the proliferative cells corresponded with stratum spinosum and showed a wide eosinophilic cytoplasm with central nuclei and prominent single nucleoli. Scattered keratinocytes appeared vacuolated, but neither koilocytes nor inclusion bodies were seen. In several foci, keratinocyte nests were interspersed between the endothelial proliferation in the transition between the dermis and epidermis. Occasionally, a clear squamous differentiation was observed with the eventual formation of keratin pearl–like eosinophilic centers but without cellular atypia, conforming typical squamous eddies (Fig. 3). In other foci, images of dyskeratosis were evident along with keratinocyte apoptosis (Fig. 3, inset).
No evidence of bacterial, fungal, or parasitic structures was identified with Gram, Giemsa, Gomori methenamine silver, and Warthin-Starry staining. Orcein staining did not show any change compatible with solar elastosis.
The immunohistochemical study revealed positive staining of every cell forming vascular channel walls against von Willebrand’s factor (Fig. 4) as well as spindle cells against α–smooth muscular actin (Fig. 4, inset). No desmin neither vimentin positive cell was detected but scattered vimentin-positive fibroblasts. Moreover, the overlying proliferating epidermis showed marked pan-cytokeratin staining.
Gross, microscopic, and immunohistochemical findings led to the final diagnosis of a verrucous hemangioma with prominent pseudoepitheliomatous epidermal hyperplasia and acanthosis. According to the final diagnosis, surgical removal was proposed, but the owner preferred not to treat the animal due to economic reasons. At a 1-year follow-up, with treatment involving only daily antiseptic washes and without any specific topical or systemic therapy, the mass had diminished significantly, being detected only in a 0.5 × 0.5–cm skin lesion without identifying any mass on palpation.
Reported hemangiomas in yearlings appear to have a congenital origin, raising the question of whether the lesions are true neoplasms or vascular malformations. 7 Hemangiomas have also been rarely reported in the dermis and subcutis of several locations in adult horses. 6 In our case, the gross presentation of the tumor resembled that previously reported for verrucous hemangiomas. 11 The location and appearance of the lesion led to several differential diagnoses. Histologically, there were no signs of vasculitis or parasite invasion. Most of the vascular spaces were recognized as capillaries without a clear surrounding muscular layer and were arranged in line with the superficial epidermis. Granulation tissue commonly presents a perpendicular arrangement of the neoformed vessels in relation to the epidermis. 1 Nonetheless, in our case, there was no such arrangement, and the proportional paucity of collagen and fibroblasts together with the lack of a previous injury in the area discards the diagnosis of a granulation tissue.
Verrucous sarcoids resemble the gross findings of this case. Although polymerase chain reaction could not be performed in our case to rule out the presence of bovine papillomavirus 1 or 2, verrucous sarcoids consistently show a proliferation of dermal fibroblasts with a picket fence distribution in the dermal-epidermal junction, 9 findings not seen in our case, which makes this diagnosis improbable. The lack of any agent in the epidermis and dermis and the absence of inclusion bodies also discarded any infectious agent.
The striking hyperkeratotic epidermis observed in our case allowed the final diagnosis of verrucous hemangioma. Typically, the epidermal hyperplasia associated with this tumor has been defined as irregular to papillated without the atypical squamous growth seen here. 11 Pseudoepitheliomatous epidermal hyperplasia is a subtype of pseudocarcinomatous hyperplasia arising from the epithelial component without involvement of adnexal structures. 8 It usually represents an exuberant reactive epithelial proliferation characterized by prominent irregular epithelial hyperplasia, acanthosis, stratum basale activation, and disorganized tongue-like projections that extend into the dermis resembling the downward invasion of squamous cell carcinomas (SCCs). 5 Both the presence of squamous eddies and the pseudoepitheliomatous hyperplasia have been related to concurrent dermal neoplasia. 6,8 The keratinocyte nests and squamous eddies found in the present case could be related to a trimming artifact or to the proliferation of the epidermis associated with the dermal neoplasia. The former was ruled out by reorientation and reinclusion of the sample. The latter is supported by the report of concomitant hemangiomas and overlying SCCs in the same biopsy. 2
Angiokeratoma is a rare neoplasia in veterinary medicine characterized by a proliferation of vascular spaces and irregular hyperplasia of the epidermis. Typical veterinary angiokeratomas show dilated vascular spaces filled with blood in the superficial dermis, 3 contrary to our case. Moreover, in human angiokeratomas, the lesion is limited to the superficial dermis. 4 SCC was discarded due to the lack of atypical mitotic figures and atypical nuclei, rare dyskeratosis, and the absence of a basement membrane or adjacent tissue invasion. The clinical outcome also supports the exclusion of SCC as a possible cause. 11
The dermal mass of this case presented the common features of capillary hemangiomas. The lack of blood-filled vascular spaces discarded the cavernous variant of hemangioma. The presence of erythrocytes inside the vascular spaces and the normal morphology of the endothelium ruled out an epithelioid variant. 12 In addition, the mass was not circumscribed, which mimics the previous descriptions of dermal hemangiomas, in contrast to the well-delineated subcutaneous variants. 6
In summary, here we describe a clinical case of verrucous hemangioma in an adult gelding with striking epidermal changes and a partial regression without treatment. The concomitant dermal neoplasia and epidermal pseudoepitheliomatous hyperplasia with squamous eddies can lead to a mistaken diagnosis, making it necessary to carefully evaluate the mass to recognize the primary process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported here was supported with funding from Plan Andaluz de Investigacion (CTS-661 group) from Consejeria de Salud de la Junta de Andalucia.