
Abstract
A 9-year-old Thoroughbred gelding presented with a 97-day history of poor performance and intermittent fever. Clinicopathologic changes included increased serum activity of γ-glutamyltransferase and alkaline phosphatase, mild hyperbilirubinemia, and leukocytosis with neutrophilia and lymphopenia. Abdominal ultrasound revealed hepatomegaly with hyperechoic hepatic parenchyma and biliary distention. Pathologic findings included marked hepatomegaly (liver 3.6% of body weight), firm hepatic consistency with a diffuse enhanced reticular pattern, severe portal bridging and sinusoidal fibrosis, oval cell/bile duct hyperplasia, and bile stasis. The differential diagnoses and diagnostic workup to achieve the diagnosis are briefly discussed.
History and Laboratory Tests Results
A 9-year-old 505-kg Thoroughbred gelding racehorse presented with a 97-day history of poor performance since early December 2010. In late December, it developed intermittent fever variably between 39.4°C and 41.1°C. Biochemical analyses of serum and complete and differential blood cell counts performed in early and late January revealed marked increased serum activity of γ-glutamyltransferase (GGT), slight increased activity of alkaline phosphatase (ALP), mild hyperbilirubinemia, and leukocytosis with neutrophilia and lymphopenia (Table 1). An abdominal ultrasound performed in late January revealed hepatomegaly with increased echogenicity of the hepatic parenchyma and biliary duct distention. In late February 2011, the clinical course progressed to head pressing, jaundice, anorexia, and weight loss. The horse was euthanized due to poor prognosis on March 11, 2011, and submitted to the California Animal Health and Food Safety Laboratory, Davis for postmortem examination.
Relevant Results of the Serum Biochemistry and Blood Cell Counts.
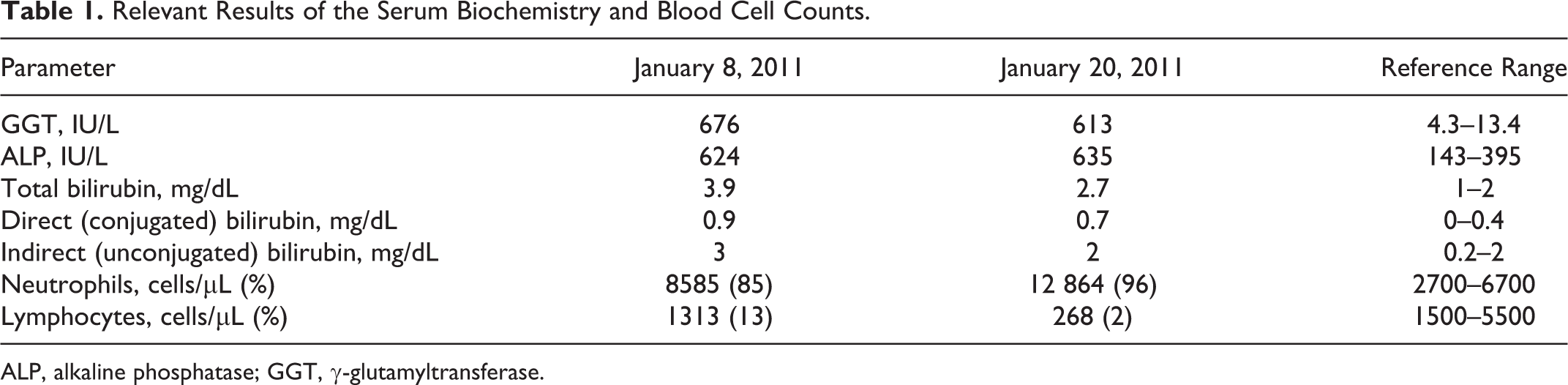
ALP, alkaline phosphatase; GGT, γ-glutamyltransferase.
Differential Diagnoses
The history, clinical signs, clinicopathologic, and ultrasonographic changes were suggestive of chronic liver disease. 1,5,7 The differential diagnoses included toxic (pyrrolizidine alkaloids [Senecio spp., Crotalaria spp., Echium spp., Heliotropium spp., Amsinckia spp., etc], aflatoxins, Panicum spp., iron toxicity, and other toxicants), 3,7,10 parasitic (Fasciola hepatica), metabolic (hepatic lipidosis), 7 infectious (liver abscesses or ascending cholangiohepatitis—Streptococcus equi, Corynebacterium pseudotuberculosis, Escherichia coli, Fusobacterium necrophorum, Mycobacterium spp., and bacterial or fungal pyo/granulomas), 7 neoplastic, 10 and idiopathic conditions such as chronic active hepatitis, 7 rare atypical chronic presentation of equine serum hepatitis, or hepatic amyloidosis. Hepatic or extrahepatic space-occupying lesions involving or compressing the choledochus can eventually result in obstructive hepatopathy; these potentially include inflammatory conditions (abscesses, granulomas), neoplasias, cysts (ie, hydatid cysts), hematomas, and scars. 7,10 Hepatolithiasis, cholelithiasis, and/or choledocholithiasis (calculi in the intrahepatic biliary tree, extrahepatic biliary ducts, or common hepatic bile duct, respectively) should also be considered. 2,8,9 Other intraluminal foreign bodies such as parasites (Anoplocephala magna, Parascaris equorum) and vegetal fragments can be responsible for mechanical obstruction of the choledochus. 4,10
Pathologic Findings and Diagnosis
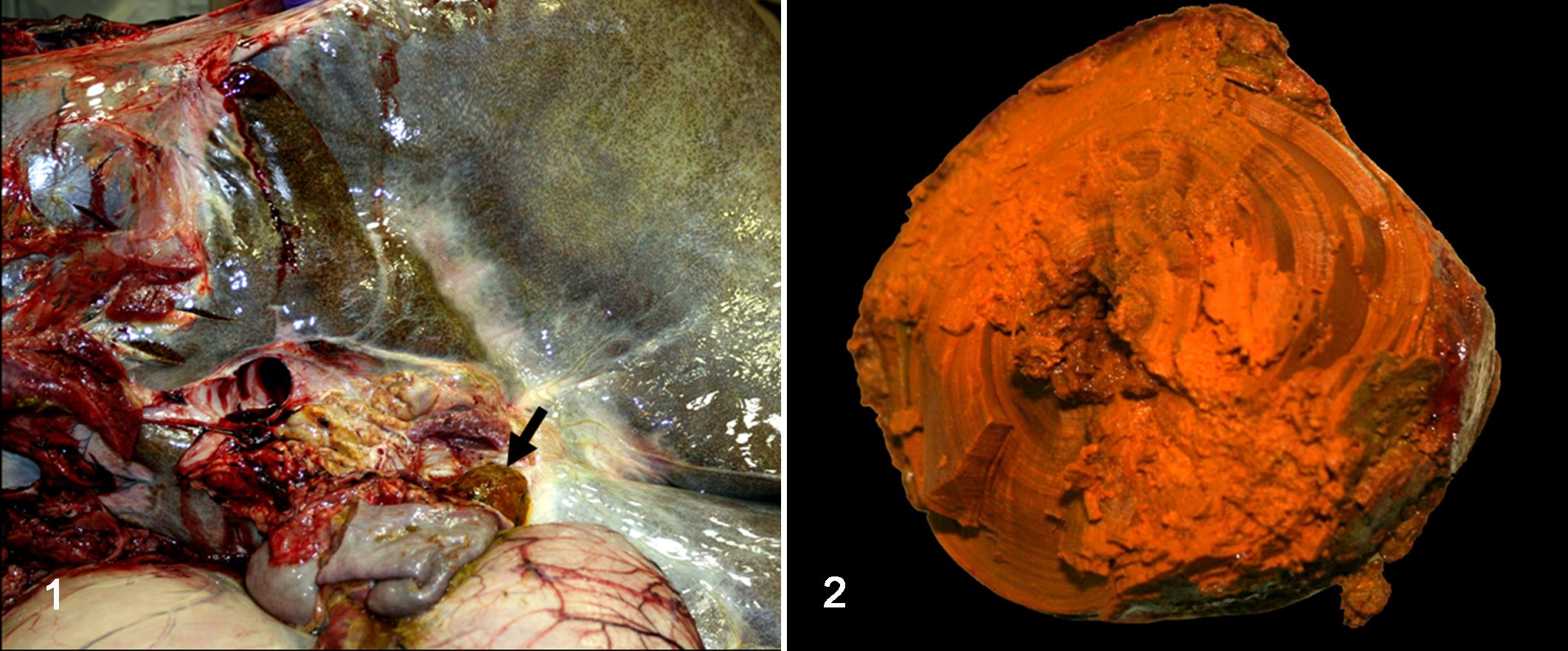
Grossly, the liver was globally and markedly enlarged (hepatomegaly), had thick margins and rounded edges, weighed 18.2 kg (3.6% of body weight; reference: 1.5%), and had a firm consistency. A diffuse enhanced reticular pattern characterized by a delicate reticular gray meshwork encircling a green-tinted hepatic parenchyma was evident on external examination of the capsular surface and on cut sections. There was a 6.5 × 4–cm ellipsoid, orange-brown to tan calculus lodged in and obstructing the lumen of the most distal aspect of the common bile duct just proximal to the choledochoduodenal junction (major duodenal papilla) (Fig. 1). The choledocholith was firm but could be cut with a knife and had a laminar appearance (Fig. 2) with a central core within which there were two 8- to 10-mm-long by 2- to 3-mm-wide lanceolate grass seeds having 2 bent 20-mm long dark-brown bristle-like appendages (awns). A gross diagnosis of obstructive hepatopathy secondary to choledocholithiasis induced by a vegetal foreign body (choledochophytolithiasis) was achieved.
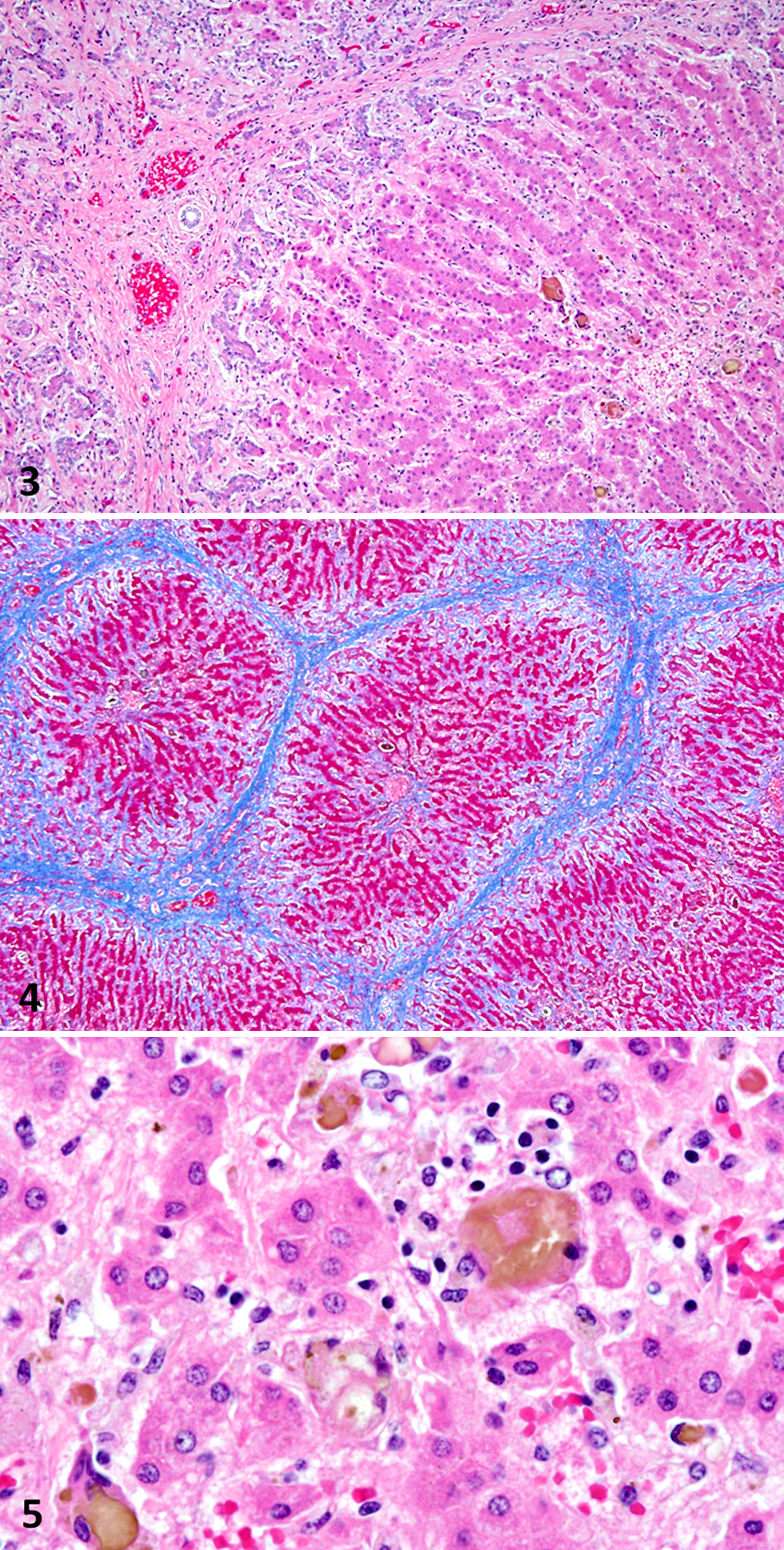
Microscopically in sections of liver, there was diffuse severe portal fibrosis with thick bands of well-organized mature fibrous collagenous connective tissue bridging between adjacent portal tracts, delineating and enhancing the limits of hepatic lobules. The fibrosis extended to the sinusoids, often disrupting the hepatic cord histoarchitecture, as well as separating and surrounding small nests of atrophic hepatocytes and the periphery of the centrilobular veins. Diffusely along the portal and bridging fibrous tracts, there was a band of proliferating oval cells occasionally forming poorly defined bile ducts (oval cell/bile duct hyperplasia) (Figs. 3 and 4). There was abundant bile pigment within the cytoplasm of Kupffer cells that were markedly distended and were often bi/multinucleated, forming scattered microgranulomas engulfing bile pigment throughout the sinusoids (Figs. 5) that stained dark green with Hall’s bile stain, indicative of cholestasis. There was also multifocal mild to moderate lymphohistiocytic portal hepatitis with fewer neutrophils and plasma cells, as well as mild sinusoidal microhemorrhage.
Ancillary Test Results
The seeds (calculus nidus) were submitted for botanic identification and were identified as florets of Avena fatua (wild oat, family Poaceae). Chemical analysis of the choledocholith (infrared spectroscopy) revealed it was composed 100% of bilirubin.
Discussion
The premortem diagnosis of liver disease in horses is sometimes difficult because the clinical signs are highly variable and usually nonspecific, and there may be liver disease without liver failure, since most of the liver functions are not lost until there is extensive loss of liver parenchyma. In the horse in this study, the elevated serum activity of GGT and ALP and the mild hyperbilirubinemia were suggestive of obstructive biliary disease, 1 and a diagnosis of severe obstructive hepatopathy due to choledocholithiasis was made at necropsy. Biliary tract disease in large animal medicine is rare. 7,10 The occurrence of biliary calculi in horses has an estimated prevalence of 0.08%, 9 but choledocholithiasis is the most common cause of biliary obstruction in this species. 4,7 The risk for biliary calculi increases with age, and generally most affected horses are older than 9 years. 5,8 Hepatolithiasis/cholelithiasis is usually asymptomatic. 10 Several calculi are generally observed, 5 but a single stone may be present. 4,7 Occasionally, the stones lodge in and obstruct the choledochus, 10 resulting in clinical disease. Cholelithiasis should be suspected in horses with anorexia, recurrent abdominal pain, icterus, and intermittent fever. 5,7 Hyperammonemic hepatic encephalopathy, photosensitization, and weight loss are other, less common features. 7 Typical laboratory findings indicative of obstructive hepatic disease in horses are increased serum activities of GGT and ALP (as in our case) and increased serum concentration of bilirubin and bile acids, 1 although these values may be normal until advanced stages of the disease. The elevation in total bilirubin during cholestasis is result of elevations in both conjugated (direct) and unconjugated (indirect) bilirubin. 7 Hyperbilirubinemia should be interpreted cautiously in horses since anorexia or fasting may decrease bilirubin uptake by hepatocytes, and the total serum bilirubin concentration may reach 10 mg/dL in otherwise healthy horses. 1 Posthepatic biliary obstruction is expected to increase conjugated bilirubin concentration, but hepatic injury secondary to cholestasis also may result in increased concentration of unconjugated bilirubin. In the horse, cholestasis should be suspected if more than 25% to 30% of the total bilirubin is of the conjugated type. 7 Evaluation of other laboratory parameters is necessary to provide more information about the cause of the hyperbilirubinemia; increased GGT and/or ALP activity suggests cholestasis. 1 In the serum biochemistry analysis performed in late January in this horse, conjugated bilirubin represented 26% of total bilirubin, which along with the elevation in the serum activity of GGT and ALP led to the presumptive clinical diagnosis of cholestasis.
Ultrasonography is a reliable noninvasive aid in the premortem diagnosis of chronic liver disease and cholelithiasis as it allows the investigation of the liver size, echogenicity of the hepatic parenchyma, and the presence of liver masses, dilated bile ducts, and stones. 8 Ultrasonographic identification of hepatic calculi is possible in 44% to 75% of cases, 5,8 but their identification in the common bile duct is more difficult than in intrahepatic or peripheral bile ducts due to its anatomic location. 4 The ultrasonographic findings in our horse were suggestive of obstructive hepatopathy, but the choledocholith could not be found in a detailed examination. Endoscopy or surgical exploration may be necessary for a definitive premortem diagnosis of choledocholithiasis in horses. 2
In this case, a diagnosis of choledocholithiasis was confirmed postmortem, and both gross and microscopic lesions described here were consistent with those described elsewhere in the literature. 7,8,10 Interestingly, a vegetal foreign body identified as florets of wild oats was found in the center of the calculus. Most likely, the wild oat florets reached the common bile duct through the major duodenal papilla during normal intestinal peristalsis, serving as a nidus for bilirubin deposition and consequent choledocholith formation and leading to clinical obstructive hepatopathy. A case of choledocholithiasis in which a vegetal foreign body (wooden stick) served as a nidus for stone formation has been reported in a horse previously, 4 but the vegetal species was not identified. In people, choledocholithiasis associated with fish bone nidus for stone formation has been reported. 6
This report illustrates an unusual presentation of choledocholithiasis caused by an intraluminal vegetal foreign body in a horse and represents a very rare example of this condition in which the foreign body could be identified as florets of wild oat, a species that is widely distributed throughout the United States (http://plants.usda.gov/java/profile?symbol=AVFA) and the world.
Footnotes
Acknowledgements
We thank Terry Wildman and Karen Sverlow for their technical assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.