
Abstract
Objectives:
Post-obstructive pulmonary edema is thought to occur from hemodynamic changes secondary to forced inspiration against the closed airway due to acute or chronic airway obstruction. We report a case of a 13 month-old boy who developed pulmonary edema from aspirated foreign body, nuts.
Methods:
He underwent emergency bronchoscopy to confirm the clinical diagnosis of aspirated nuts in the trachea and nuts were removed endoscopically. His trachea was then intubated and he was mechanically ventilated with oxygen.
Results:
He developed florid pulmonary edema early in the course with tracheal obstruction and during endoscopic removal of nuts. After removal of obstruction he was ventilated mechanically and pulmonary edema cleared rapidly.
Conclusions:
Aspirated nuts obstructing trachea can induce obstructive pulmonary edema. Early recognition of foreign body obstruction based on clinical history and its removal resolved pulmonary edema.
Introduction
Post-obstructive pulmonary edema (POPE) has most frequently been described after an upper airway obstruction.1–3 We report the case of a 13-month-old boy who developed POPE following acute respiratory distress from an obstruction of the distal trachea following aspiration of a foreign body (FB). This case illustrates the importance of considering FB aspiration as a cause of POPE.
Case report
A 13-month-old boy with a history of a small ventricular septal defect was brought to the emergency department (ED) for an acute onset of respiratory distress after FB aspiration. The child grabbed a granola bar with nuts from his mother and ate it while walking and laughing. Suddenly, he started choking and developed breathing difficulty. His father and a neighbor administered back blows, but he did not cough up any nuts. His father immediately called 911. When the emergency medical service (EMS) arrived within a few minutes, the child was still responsive and breathing on his own, but developed worsening respiratory distress. EMS found him cyanotic, but did not see any visible FB in the oral airway or oropharynx. EMS initiated bag mask ventilation with 100% oxygen and brought him to the ED. In the ED, he was noted to be in moderate respiratory distress with respiratory rate of 52/min, heart rate of 171/min and oxygen saturation of 90% on non-rebreather mask with 100% oxygen. He had noisy breathing, but was able to phonate intermittently and made a weak cry. He was pale and had mottled skin with cold extremities. Chest auscultation revealed decreased air entry in both lung fields without wheezing or crackles.
The ED attending physician performed direct laryngoscopy, but did not find any FB. The anesthesiologist intubated the child with a 4.0 uncuffed endotracheal tube for the progressively worsening respiratory distress with oxygen desaturation. A peripheral intravenous line and an intraosseous line were placed and normal saline bolus was started. Initial chest X-ray (CXR) showed patchy opacity in the right middle lobe (Figure 1). A repeat CXR to confirm the position of endotracheal tube showed interval development of bilateral, diffuse, hazy ground glass opacities suggestive of pulmonary edema (Figure 2). The patient received dexamethasone, nebulized racemic epinephrine and Unasyn. Venous blood gas showed pH of 7.20, PvCO2 of 50 mmHg, PvO2 of 28.6 mmHg, HCO3 of 10.9 mmol/L, base deficit of 15.8, oxygen saturation of 63.8% on mechanical ventilation with inspired oxygen of 100%, respiratory rate of 25/min and pressure support (PS) of 18 cm H2O with positive end-expiratory pressure (PEEP) of 10 cm H2O. The basic metabolic panel revealed Na 134 mmol/L, K 4 mmol/L, Cl 110 mmol/L, CO2 of 14 mmol/L, glucose 418 mg/dL, blood urea nitrogen (BUN) 17 mg/dL and creatinine 0.4 mg/dL. CO2 of 14 mmol/L suggested metabolic acidosis, most likely a lactic acidosis either from hypoxemia or systemic circulatory impairment from hemodynamic changes of Muller’s maneuver in response to FB obstruction of trachea.

Hazy opacity projecting over the right heart border on presentation to ED.
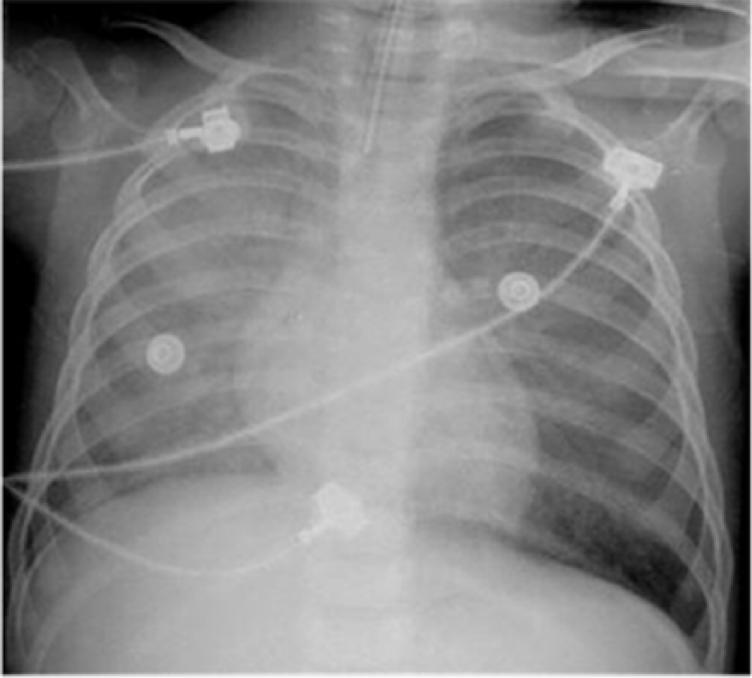
Interval development of bilateral diffuse hazy opacities suggestive of pulmonary edema (45 min after Figure 1).
The otolaryngologist performed bedside flexible laryngoscopy, which also did not show a FB in the larynx or hypopharynx. The child was taken emergently to the operating room (OR) for direct laryngoscopy and rigid bronchoscopy. Multiple pieces of nuts were found in the distal trachea at the level of carina (Figure 3), occluding the airway completely. All the pieces of nuts were removed. During the procedure, a significant amount of pink, frothy fluid suggestive of pulmonary edema fluid was suctioned from the airway. Tracheal aspirate and blood culture for bacteria were taken and he was started on intravenous Unasyn. He received another dose of dexamethasone, two doses of furosemide 20 mg each and nebulized albuterol. After complete removal of the FB from the airway, he was re-intubated with a 4.0-mm endotracheal tube and was placed on mechanical ventilation with inspired oxygen of 100%. His respiratory status continued to worsen. A repeat CXR (Figure 4) 2½ h after initial CXR showed worsening pulmonary edema. The ventilator settings were readjusted to PS of 24 cm H2O and PEEP of 10 cm H2O to achieve oxygen saturation greater than 94%. He was transferred to the pediatric intensive care unit for further management of pulmonary edema and close monitoring of respiratory status. Pediatric pulmonary was notified late and was not involved in the bronchoscopy for FB removal.

On bronchoscopy, multiple pieces of nuts found in the distal trachea at the level of carina were removed entirely.

Further worsening of pulmonary edema after removal of foreign body (2½ h after Figure 2).
He was extubated 15 h later when his oxygen saturation improved and was placed on bilevel positive airway pressure (BiPAP) mask. Arterial blood gas showed pH of 7.37, PaCO2 of 40 mmHg, PaO2 of 65 mmHg, HCO3 of 23 mmol/L, base deficit of −2 and oxygen saturation of 92% on BiPAP of 10/5 cm H2O with inspired oxygen of 35%. By this time, HCO3 had increased to 23 mmol/L reflecting reversal of metabolic acidosis when oxygenation improved and systemic circulation was normalized. A CXR taken 36 h after initiation of mechanical ventilation showed a marked resolution of the bilateral pulmonary edema. Unasyn was discontinued 3 days later when cultures from the tracheal aspirate and blood were negative. He was weaned to room air on hospital day 3 and discharged to home on hospital day 4. On multiple follow-up visits to clinic, the child was doing well with no long-term respiratory complications.
Discussion
When a young child presents to the ED with sudden onset of respiratory distress, there are wide differential diagnoses to consider including croup, epiglottitis, bronchiolitis, asthma, aspiration pneumonia and FB aspiration. In the context of a child who presents with a history of eating a candy bar containing nuts, while walking and laughing and then developing a choking spell followed by respiratory distress, FB aspiration is suspected as the most likely cause.
FB aspiration can be a medical emergency as in our case and requires immediate intervention to remove the obstructing FB. For our patient, the pediatric otolaryngologist performed bronchoscopy emergently to remove the FB obstructing the trachea. Pediatric pulmonary should ideally join the otolaryngologist in performing flexible bronchoscopy to evaluate the airway for residual pieces, but the pediatric pulmonologist usually does not remove foreign bodies.
POPE, also referred to as negative pressure pulmonary edema (NPPE), is a life-threatening condition, in which immediate, acute pulmonary edema develops after an upper airway obstruction. Two distinct subclasses of POPE have been described in the literature: type I is associated with forceful inspiratory effort in the context of an acute airway obstruction and type II occurs after relief of a chronic partial airway obstruction.4,5
The first description of POPE was on an animal model in 1927. 6 Oswalt et al. 7 first reported pulmonary edema in adults as a complication of upper airway obstruction in 1977. Luke et al. 8 suspected pulmonary edema in pediatric patients as a complication of adenotonsillar hypertrophy in 1966. The first pediatric case of POPE was reported in association with acute upper airway obstruction in the 1970s. They described development of pulmonary edema following FB aspiration and after the relief of airway obstruction from croup and epiglottitis.9–11 Ringold et al. 12 reported two patients with POPE following FB aspiration in the upper airway and reviewed the literature on pediatric case series in 2004. Subsequent reports indicate that postoperative laryngospasm after anesthesia as the most common cause of adult POPE. 13 However, the true incidence of pulmonary edema associated with airway obstruction from FB aspiration is not known. Among the pediatric patients who develop type 1 POPE associated with an upper airway obstruction secondary to croup and epiglottitis, it is estimated that 12%–28% may require active airway intervention such as intubation or tracheostomy.11,14,15 Subsequent reports indicated that postoperative laryngospasm after anesthesia as the most common cause of POPE in adults. 15 In a case series describing type 1 POPE, the time to onset of edema ranged from 5 to 240 min following an acute airway obstruction, with a mean of 33 min. The time to resolution of symptoms ranged from 2 to 96 h with a mean of 42 h. 15 Various physiologic mechanisms for development of POPE have been proposed, but the precise pathophysiology remains uncertain.
One plausible theory states that POPE may be caused by significant fluid shifts due to changes in intrathoracic pressure. In an acute upper airway obstruction, a patient takes forceful inspiration against the obstruction, known as Muller’s maneuver. Excessive negative intrathoracic and pleural pressure generated by forceful inspiration against the obstruction leads to increased venous return to the right heart, which in turn causes increased right ventricular (RV) output and increased pulmonary artery pressure. The left ventricular (LV) function is impaired due to the markedly decreased pleural pressure surrounding LV, increasing LV transmural pressure and afterload. 16 LV function is further impaired from the rising RV pressure pressing on the interventricular septum affecting the LV contraction. The impaired LV function leads to increased pulmonary venous pressure and increased pulmonary capillary back pressure. When the pulmonary transcapillary pressure exceeds 20 cm H2O, fluid leaks from the capillary bed to the surrounding low pressure pulmonary interstitium. When the capillary transudation into the interstitium reaches a critical point, the interstitial fluid floods the regional alveoli causing pulmonary edema. 17 A similar mechanism operates in pulmonary edema formation in patients with congestive heart failure or volume overload states. 18
Another factor implicated in the pathophysiology of POPE is the effects of hypoxemia and subsequent hyper-adrenergic state on cardiac function and capillary permeability. Hypoxemia and consequent acidosis are believed to cause a massive sympathetic discharge resulting in systemic vasoconstriction and shift of the blood from the systemic circulation to the low pressure pulmonary circulation. 19
Prompt diagnosis and management of POPE allows for its resolution within 24 h. 20 Standard treatment includes positive pressure ventilation and diuretics. Whether the addition of diuretics plays a role in the resolution of POPE is not clear.2,3 Mild pulmonary edema can be treated with supplemental oxygen alone. More severe pulmonary edema may require intubation and positive pressure ventilation. Overall, patients have a good prognosis if they are promptly diagnosed and appropriate treatment is instituted.
Conclusion
The development of POPE has been associated with upper airway obstruction, but our case demonstrated that POPE can occur with obstruction of the distal trachea, which is considered lower airway. Obstruction of the lower end of trachea nevertheless causes physiological disturbance similar to that of the upper airway. This case illustrates the importance of considering FB aspiration as an uncommon cause of POPE. 21 Prompt diagnosis will lead to appropriate treatment of POPE leading to its rapid resolution.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.