
Abstract
Intestinal volvulus was recognized as the cause of death in 18 cetaceans, including 8 species of toothed whales (suborder Odontoceti). Cases originated from 11 institutions from around the world and included both captive (n = 9) and free-ranging (n = 9) animals. When the clinical history was available (n = 9), animals consistently demonstrated acute dullness 1 to 5 days prior to death. In 3 of these animals (33%), there was a history of chronic gastrointestinal illness. The pathological findings were similar to those described in other animal species and humans, and consisted of intestinal volvulus and a well-demarcated segment of distended, congested, and edematous intestine with gas and bloody fluid contents. Associated lesions included congested and edematous mesentery and mesenteric lymph nodes, and often serofibrinous or hemorrhagic abdominal effusion. The volvulus involved the cranial part of the intestines in 85% (11 of 13). Potential predisposing causes were recognized in most cases (13 of 18, 72%) but were variable. Further studies investigating predisposing factors are necessary to help prevent occurrence and enhance early clinical diagnosis and management of the condition.
The order Cetacea includes approximately 85 species of whales, dolphins, and porpoises with 2 suborders: Odontoceti, compromising the toothed whales, and Mysticeti, the baleen whales. Increasing our knowledge about causes of death in marine mammals is important to help conservation efforts and improve clinical management of captive animals.
Volvulus is a rotation of the intestine on its mesenteric axis. 6 Compression of thin-walled veins in the mesentery tends to occur before the influx of arterial blood is obstructed. The tissues normally drained by the obstructed veins, such as the intestine, mesenteric lymph nodes, and mesentery, become congested and edematous, and large amounts of fluid can be trapped, causing hemodynamic stress. In addition, the lumen of the involved intestinal segment is obstructed and, over time, can become severely distended with bloody fluid and gas. There is often loss of integrity of the intestinal wall and subsequent septic peritonitis. 1 Without intervening surgery, the death of the animal usually follows quickly. 1,14,18
If the intestinal volvulus is present at time of necropsy and the lesions are not obscured by postmortem changes, the diagnosis is usually readily made via gross examination. 1 The intestinal twist may reduce before the necropsy is performed, typically during transport and handling of the body. 10 A probable diagnosis can be made by finding a sharply demarcated area of congested and edematous bowel and mesentery with distention of the intestinal lumen by blood and gas, potentially accompanied by ascites or peritonitis. In cases with loss of the twist, differentiation from peracute Clostridium perfringens–type B enteritis 3 and from intestinal incarceration is needed.
Intestinal volvulus has been well documented in humans, and there appear to be variations in incidence and predisposing causes dependent upon geographical location, sex, and age class. 11,12
Intestinal volvulus is likely to occur in all animals. 4,14,18,30 It has been documented most commonly in horses, swine, and suckling ruminants, with different predisposing factors reported. 1 However, in marine mammals there are only isolated case reports or incidents mentioned in larger studies. Intestinal volvulus has been reported as the cause of death in 14% of 355 and 1% of 232 free-ranging harbor seals (Phoca vitulina) in comprehensive studies of pathological findings in this species. 22,25 It is mentioned as the cause of death in 1 free-ranging sea otter (Enhydra lutris), 26 and there are case reports of an adult male captive stellar sea lion (Eumetopias jubatus) 19 and a free-ranging adult female dugong (Dugong dugon). 7 Within several large case series of cetaceans, intestinal volvulus was listed as the cause of death for 2 bottlenose dolphins (Tursiops truncatus), 27 a harbor porpoise (Phocoena phocoena 13 ; case No. 1, Table 1), and a beluga whale (Delphinapterus leucas). 16 In addition, there is 1 published description of a suspected intestinal volvulus in an adult female bowhead whale (Balaena mysticetus) involving 7 m of the midjejunum. The volvulus was suspected to have been reduced by postmortem handling of the carcass. 10
Signalement, Gross and Histologic findings related to intestinal volvulus in 18 cetaceans
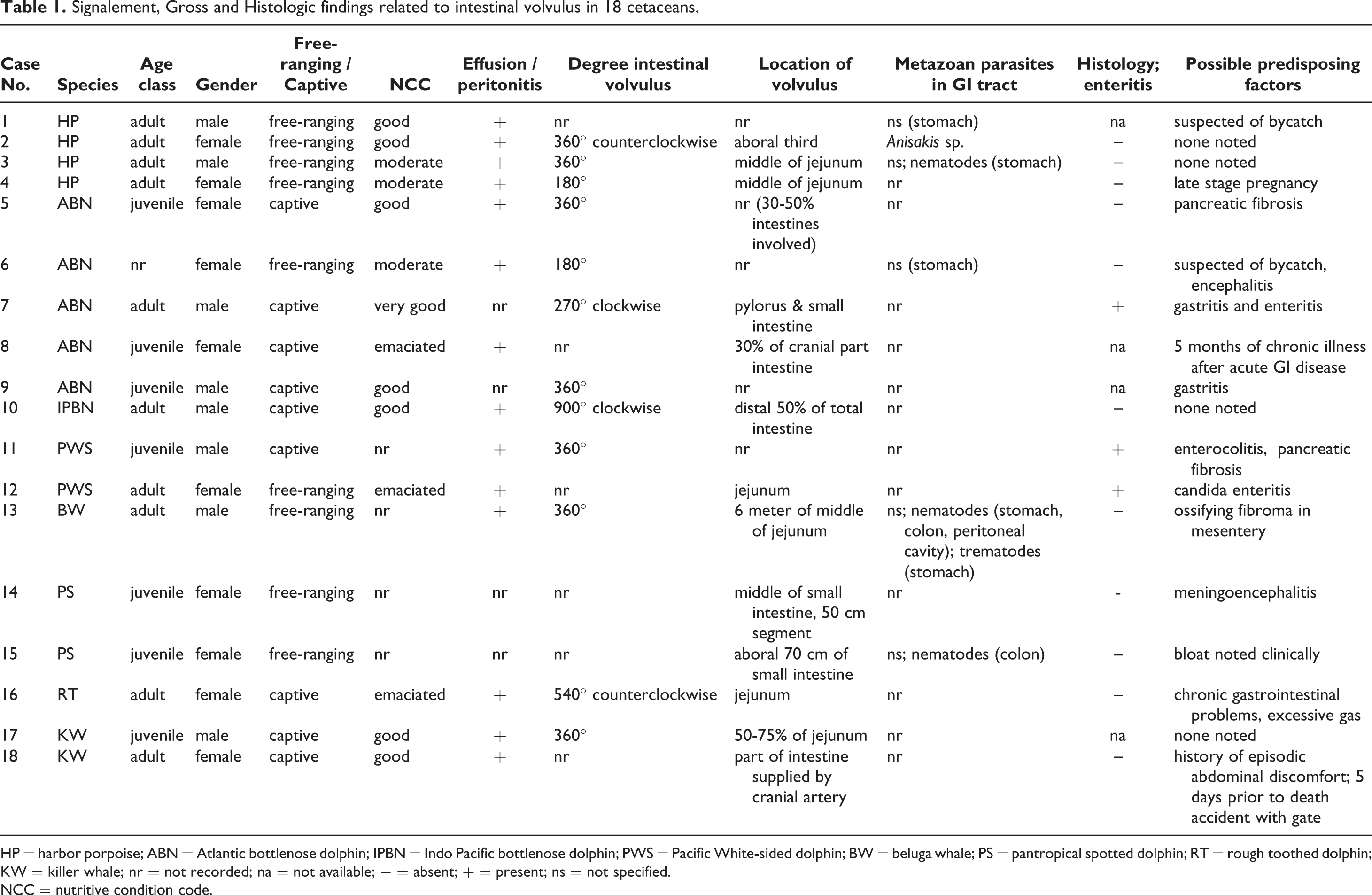
HP = harbor porpoise; ABN = Atlantic bottlenose dolphin; IPBN = Indo Pacific bottlenose dolphin; PWS = Pacific White-sided dolphin; BW = beluga whale; PS = pantropical spotted dolphin; RT = rough toothed dolphin; KW = killer whale; nr = not recorded; na = not available; − = absent; + = present; ns = not specified
NCC = nutritive condition code
Here we report the postmortem results of 18 animals constituting 8 odontocete species with naturally occurring intestinal volvulus. The cases originate from 11 institutes within Europe, North America, Asia, and Australia. We present and compare the gross and histologic lesions, compare species incidence, and discuss possible predisposing factors of intestinal volvulus.
Materials and Methods
A variety of marine mammal clinicians and pathologists were queried about cases of intestinal volvulus within their records. Submitting facilities included zoos and display facilities that respond to stranded free-ranging cetaceans and diagnostic services that receive samples from these facilities. Selection criteria included availability of a complete gross necropsy report describing intestinal volvulus present at time of necropsy and changes consistent with antemortem presence of the volvulus, such as congestion and edema of the intestine or ascites. For each animal, the following information was obtained when possible: species, sex, age, medical history, nutritional status, gross necropsy findings, histologic findings, and results of ancillary testing. The age class (neonate, juvenile, or adult) of the free-ranging animals was estimated on the basis of standard body-length measurements and evidence of maturity of the gonads. 5,20 Half of the selected cases were stranded animals from free-ranging populations, and the decomposition condition code of those animals was categorized in a standardized method prior to necropsy, with code 1 being alive and code 5 being severely decomposed. 23 Eighteen odontocete cetaceans (case Nos. 1–18), examined between 1991 and 2011, associated with 11 institutions, met the criteria for inclusion. There were no cases reported in the suborder Mysticeti. Information about species, age class, sex, autolytic state of the animal at time of necropsy, and country of origin can be found in Table 1.
Histopathology
Tissues available for histologic review varied by case and included brain, skin, skeletal muscle, heart, lung, trachea, liver, kidney, spleen, lymph nodes, thyroid gland, thymus, adrenal gland, pancreas, gonads, esophagus, stomach, intestine, and mesentery. Tissues were routinely fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned at 4 to 7 μm, stained with hematoxylin and eosin, and examined microscopically.
Ancillary Tests
In case Nos. 2, 5, 12, 14, and 16, diagnostic aerobic and anaerobic cultures were performed on various sections of the gastrointestinal tract. Material was collected at necropsy, inoculated, and incubated at 37°C for periods ranging from 2 to 10 days. In case No. 12, additional fungal media was employed. In case No. 2, multiplex polymerase chain reaction was performed for toxin typing of C. perfringens. 29
Results
Animals
Eighteen odontocetes of 8 species met the study inclusion criteria (Table 1) with variation in the extent of histopathology and ancillary tests performed per case. The species represented included harbor porpoise (Phocoena phocoena; n = 4), Atlantic bottlenose dolphin (Tursiops truncatus; n = 4), Indo Pacific bottlenose dolphin (Tursiops aduncus; n = 2), Pacific White-sided dolphin (Lagenorhynchus obliquidens; n = 2), beluga whale (Delphinapterus leucas; n = 1), pantropical spotted dolphin (Stenella attenuata; n = 2), rough-toothed dolphin (Steno bredanensis; n = 1), and killer whale (Orcinus orca; n = 2). In all cases, the cause of death was attributed to the volvulus and associated conditions.
Nine cases were animals held in captivity, and 9 were stranded animals. Clinical signs in the captive animals were noted between 1 and 5 days prior to death. Animals showed dullness, and in case Nos. 9–11, 13, 17, and 18 anorexia was noted (6 of 9, 67%). Case No. 7 had colic and asymmetric distention of the abdomen. Case Nos. 13, 15, and 16 had bloat with gas in the stomach and rectum. In case Nos. 8, 13, and 18, the clinical history mentioned chronic or recurrent gastrointestinal problems over a variable period. In case No. 13, this included anorexia, vomiting, and unspecified parasites detected by fecal flotation a month before death. Case No. 18 showed intermittent abdominal discomfort and diarrhea for approximately 6 years prior to death.
Among the free-ranging animals, 8 were found dead, and 1 harbor porpoise (case No. 2) was stranded alive but died shortly after it was found with no clinical signs noted. Where recorded, all captive animals died spontaneously.
Pathologic Findings
The gross findings associated with the intestinal volvulus are summarized in Table 1. In 78% (14 of 18) of the cases, moderate to severe, acute, diffuse peritoneal effusion or peritonitis was recorded. The appearance of the peritoneal fluid varied from serofibrinous to hemorrhagic. The degree of intestinal volvulus was recorded in 10 of 18 animals and ranged from 180° to 900° but was most often 360° (6 of 10). In case Nos. 8 and 10, the volvulus was clockwise, and in case No. 2 it was counterclockwise as seen from the caudal aspect. The estimated extent of the portion of intestine involved ranged from 50 cm (case No. 14) to 30% to 50% of the entire intestinal tract (case Nos. 2, 5, 8, 10). The location of the volvulus was recorded in 13 cases, involving the proximal half of the intestines in 85% (11 of 13).
In 83% (15 of 18) of the cases, the involved intestinal segment was reported to be focally extensively dark red to purple to black with an obvious demarcation from the adjacent nonaffected intestines (Fig. 1). The intestinal wall was either thickened and firm with congestion and edema or had focal or multifocal areas of decreased thickness to 1 mm with 1- to 2-mm ulcerations of the mucosa. Perforation was noted in case No. 4, although due to the decomposition of this case, postmortem artifact could not be excluded. The involved segments were often (7 of 18, 38%) distended with gas and had dark red to dark brown liquid contents. In the mesentery distal to the twist, multifocal hemorrhages and infarctions, as well as multifocal or diffuse edema and congestion of both blood and lymphatic vessels, were noted in 73% (13 of 18) of the cases. In some cases (case Nos. 2, 12, 16, 18), mesenteric lymph nodes were involved in the mesenteric twist and were enlarged up to threefold the normal size due to congestion and edema. In the beluga whale (case No. 13), the twist wrapped around a 26 × 21 × 18 cm, 6.5-kg ossifying fibroma in the mesentery of the proximal jejunum. In case No. 18, there was an intestinal volvulus without congestion and edema of the affected intestine although the associated lymph nodes and mesentery were enlarged and hemorrhagic.
Unspecified metazoan parasites of the gastrointestinal tract were seen macroscopically in 33% (6 of 18) of the cases. No tests were performed to determine the presence of parasites, and speciation was not performed. In 6 of the free-ranging animals, the stomach contents were recorded. In these cases, the stomachs were empty or contained scant contents.
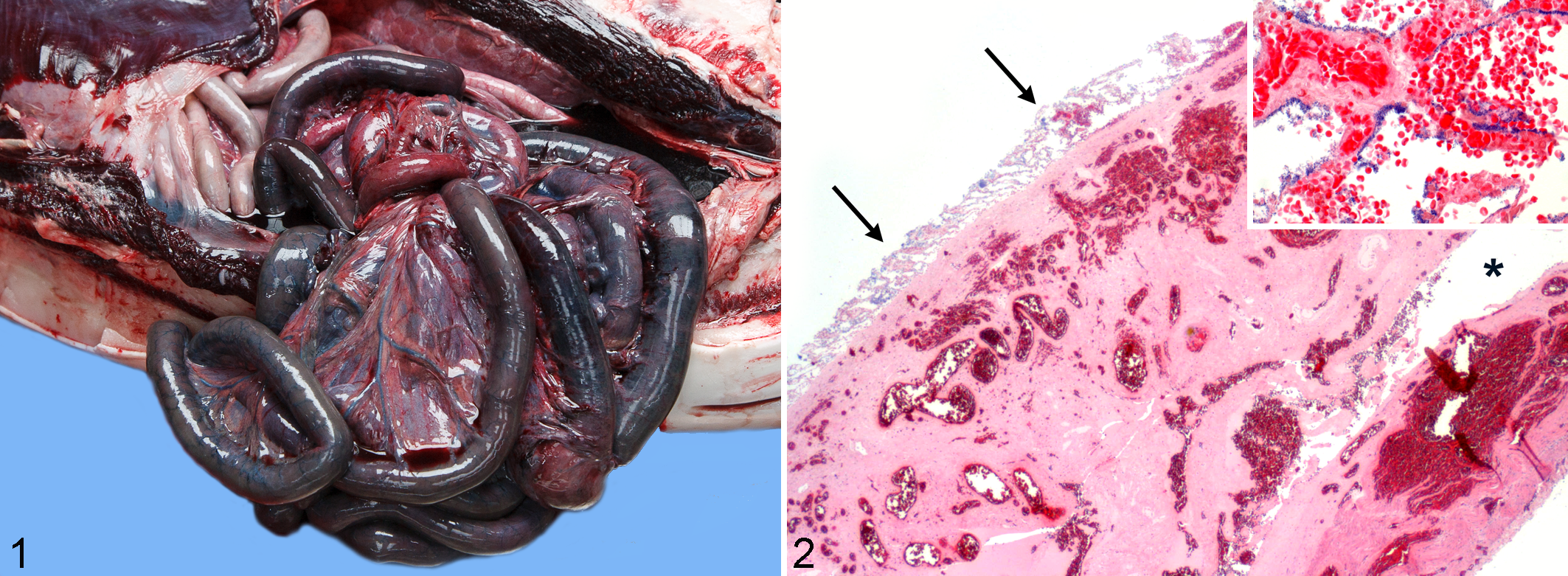
Histologic findings related to the twist were recorded in 11 of 18 cases. The intestines involved in the volvulus showed severe congestion and edema, sometimes with multifocal to coalescing hemorrhages. There was variable necrosis ranging from only the superficial mucosa to transmural involvement with mild to severe perivascular to interstitial neutrophilic infiltration. In case No. 2, a layer of bacteria, predominantly large bacilli, covered the mucosa, and there was expansion of the tunica muscularis by variably sized clear spaces (emphysema) lined by rod-shaped bacteria (gas gangrene; Fig. 2). In case No. 18, the mesentery showed severe congestion and hemorrhage, and a large mesenteric artery and vein contained a partially occlusive thrombus.
Concurrent significant macroscopic and microscopic findings in the gastrointestinal tract were found in 9 of 18 (50%) of cases. In several cases, mild to moderate gastritis or moderate to extensive gastric erosion and ulceration were noted and were occasionally associated with metazoan parasites (Table 1). Lymphoplasmacytic enteritis and enterocolitis were described in 2 cases (case Nos. 7 and 11). Case No. 12 had a systemic Candida spp infection with involvement of the intestine causing a multifocal lymphohistiocytic and suppurative enteritis with florid intrahistiocytic yeasts. Remaining findings in the colon included multifocal ulcerations in case No. 6, focal suppurative inflammation with intralesional nematodes in case No. 13, and a solitary parasitic cyst in case No. 15.
A few other animals had notable lesions beyond the gastrointestinal tract. Case No. 9 showed small multifocal areas of acute hepatocellular necrosis. In case No. 6 marked pancreatic atrophy was noted. There was mild, multifocal, chronic interstitial pancreatic fibrosis in case No. 5 and mild multifocal chronic pancreatitis with ductular hyperplasia and rare intralesional trematode ova in case No. 12. Other potentially important findings were a late-stage pregnancy in a harbor porpoise (case No. 4) and meningoencephalitis in case Nos. 6 and 14.
Ancillary Tests
Bacterial and yeast cultures of intestinal contents were performed in 8 cases (Table 1). Cultures of several organs from case No. 13 (kidney, synovia, lung, mammary gland, and spleen) and case No. 9 (stomach contents, kidney, liver, heart, spleen) yielded no growth. Cultures of lungs, liver, and kidneys from case No. 16 grew Escherichia coli, which was also cultured from the intestine in this case. Culture of the intestinal contents from case No. 9 yielded a mixed growth of normal fecal flora, a heavy growth of Shewenella putrefaciens, and very light growth of Candida glabrata. From the pancreas of the same case, E. coli and mixed Clostridium spp were cultured. In case No. 10, C. perfringens was grown in pure culture from the blood and cultured within a mixed population of bacteria from the intestine proximal to and within the volvulus. The cultured tissues from this animal were negative for Vibrio spp, Salmonella spp, and yeasts. Culture of the intestinal contents from case No. 2 yielded a pure growth of C. perfringens which polymerase chain reaction confirmed as type A, non–β toxin producing. In case No. 14 Vibrio damsela was grown from the anus and blowhole.
Discussion
Intestinal volvulus can be the cause of death in a variety of cetaceans, captive and free-ranging, male and female, and juveniles and adults (Table 1). The absence of baleen whales in this study is likely due to the rarity of animals for necropsy examinations. The contributing authors have a range of 0.3% to 1% Mysticeti cases within their total cetacean submissions. Typical lesions found at necropsy in this case series are analogous to those seen in other mammals. 1,4,7,14,18,28,30
The absence of severe congestion and edema of the wall of the twisted intestine in case No. 18 is intriguing. It is possible that arterial obstruction occurred early, then congestion and edema of the intestinal wall would not be expected, although loss of blood from the ischemic mucosa into the lumen would still be present. 19 This theory is supported by the histologic findings of both venous and arterial thrombi in the mesenteric vessels, demonstrating that there was at least partial obstruction of the arterial flow.
Clinical signs were nonspecific and typically acute 1,14 and as expected for intestinal obstruction with severe hemodynamic consequences. Most consistently, animals presented with acute dullness and anorexia and less commonly with regurgitation, vomiting, bloat, and excessive gas production.
Evidence of more chronic gastrointestinal disease prior to the intestinal volvulus was apparent in several animals both clinically and histologically. Three of the 9 animals with a clinical history had chronic gastrointestinal problems. In addition, of the 11 cases in which histology was performed, 4 had gastritis, enteritis, or marked pancreatic atrophy (Table 1). Therefore, gastrointestinal disease could be a risk factor in these species. There are variable reports in other animal species that relate intestinal volvulus to prior gastrointestinal disease, such as dogs with exocrine pancreas insufficiency, 8,30 gastric dilation volvulus, enteritis, 9,15,21 ileocolic carcinoma, parvoviral infection, and gastrointestinal foreign bodies, 9,17 as well as a report of a sea otter (Enhydra lutris) with fecal impaction. 26
Additionally, 6 cases had gastrointestinal parasites (Table 1). Parasitism is a common finding in free-ranging cetaceans; therefore, a correlation is difficult to make. In future evaluations, specific information relative to parasite load, parasite species, and location of those organisms may help to better define any association with enteric volvulus. In young horses, an association with Parascaris equorum infestation has been suggested. 4 In humans, a proposed etiological factor for small intestinal volvulus also includes ascariasis. 12 In none of our cases was a severe intestinal parasitic load specifically identified.
Furthermore in humans, the suggested generalized mechanism for small bowel volvulus is first an obstruction at 2 fixed points by a predisposing condition. Then, as the loop fills with liquid, peristalsis causes it to twist around its mesentery. More common causes include anatomical abnormalities, including malrotation in children, adhesions, Meckel diverticulum, leiomyomas of the mesentery, and internal hernia. 11,12,31 In the beluga whale (case No. 13), there was an ossifying fibroma in the mesentery. Mesentery and intestines wrapped around this mass in a fashion similar to that described with the mesenteric leiomyomas. One case of acute death in a captive juvenile killer whale (Orcinus orca) not included in our study had an intestinal volvulus associated with a remnant fetal ligament that was attached to the mesentery and abdominal wall (personal communication, Lanny Cornell). The intestine seemed to be coursing through the opening and around the ligament, similar to volvulus in humans due to adhesions or Meckel diverticula.
Another predisposing factor for intestinal volvulus is consumption of large quantities of food after fasting, seen in suckling calves and lambs as a relatively common entity. Additionally, swine fed a highly fermentable substrate have an increased risk to develop torsion of different abdominal organs, including intestine. 2,12,18 In the cetacean cases under the care of humans, no such feeding schedule would be typical. Likewise, in the free-ranging animals, neither the gastric or intestinal contents were excessive when noted.
One harbor porpoise had a late-stage pregnancy at the time of death. In humans, pregnancy is proposed as an etiologic factor for intestinal volvulus at the stages of rapid fetal growth. A sudden increase in the amount of space the uterus occupies in the abdomen is thought to be the inciting cause. 12,31 In a large study of 355 free-ranging harbor seals, 2 of 14 (14%) seals that had a volvulus were pregnant. 25 A similar pathogenic mechanism might underlie the intestinal volvulus cases in these seals; however, they also had uterine torsions. 25 Although a reason for this combination was not speculated on in this article, it is possible that the rolling movement of the body, rather than space occupation, caused the multiple torsions in these animals.
The intestinal volvulus in case No. 18 might suggest a similar etiology of a sudden change in abdominal organ arrangement. Five days prior to death, the animal was found leaning over a gate. Interestingly, a similar accident was described in a female captive Atlantic bottlenose dolphin (Tursiops truncatus) not included in this study (personal communication, Joseph Geraci) that died due to intestinal volvulus after being on top of a gate.
Remaining possible risk factors specific for marine mammals may relate to their normal 3-dimensional movements within the water. These risk factors include the meningoencephalitis in case No. 14 and signs of bycatch in 2 cases (case Nos. 1 and 6), which could have induced changes in behavior and abnormal movements of the animals, increasing the chance of intestinal volvulus.
All animals included in this study died spontaneously, most likely due to hemodynamic consequences or septic shock from the intestinal volvulus. In 2 animals, sepsis was diagnosed based on a pure culture of enteric bacteria from multiple organs.
Of the cases that were cultured, a variety of bacteria were found. Although C. perfringens was cultured in 2 cases, both had no signs of gastrointestinal problems prior to the intestinal volvulus. A pathogenic role of this organism, which is known to produce toxins that might alter motility, could not be excluded. 2,24 However, it is most likely that this organism proliferated secondarily in the favorable anaerobic conditions caused by the volvulus.
In addition to the presented cases, 3 cases were submitted that did not meet the inclusion criteria: a live stranded female sperm whale (Physeter macrocephalus; personal communication, Gretchen Lovewell) and 2 cases of a captive false killer whale (Pseudorca crassidens) and an adult beluga whale (personal communication, Lanny Cornell). Including these communications, a total of 23 cases were reported from approximately 30 facilities involved in postmortem diagnostic investigations in cetaceans around the world. Annual cetacean case rates per facility ranged from dozens to almost 300 animals, and databases regularly extended to 5 years. Taking into account that intestinal volvulus is a fairly recognizable gross diagnosis even in autolytic animals, although exact numbers are not available to give the precise prevalence, this condition seems to be rare in cetaceans. It is possible that anatomic differences, such as the firm, relatively large, mesenteric lymph nodes at the root of the mesentery causing rigidity and lack of a cecum in some species of cetaceans, prevent more frequent volvulus of the intestine.
Facilities holding cetaceans in captivity should be aware of this condition when animals show sudden signs of dullness and anorexia, especially when animals have chronic gastrointestinal problems. Although in many (14 of 18) of our cases, possible predisposing conditions could be recognized, these were variable. Further investigations are necessary to determine potential predisposing conditions for intestinal volvulus in these species.
Footnotes
Acknowledgements
We would like to thank the clinicians, veterinary pathologists, and technicians that contributed to this multi-institutional and international study. Special thanks to Andrew Brownlow for his advice and inspiration, Pieter Cruq for photographic assistance, Fonds van Asten for typing of the clostridial toxin, and Sjoukje Hiemstra for technical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.