
Abstract
Canine visceral leishmaniasis frequently causes renal damage that leads to chronic kidney disease. Fifteen dogs seropositive for Leishmania were selected and biopsied before (T0) and 60 days later after (T1) treatment with a specific anti-Leishmania pharmacological agent. Various parameters were selected for evaluating the glomerular and tubulointerstitial damage. At T0, mesangioproliferative and membranoproliferative glomerulonephritis were observed in 6 dogs, chronic glomerulosclerosis in 5, and end-stage kidney in 3; renal tissue from 1 dog was within normal histologic limits. The most frequently observed ultrastructural changes were foot-process effacement, thickening of the basement membranes, and immune deposits. One dog had mesangial immune deposits at T1 that had not been present at T0, so the diagnosis was changed to mesangioproliferative glomerulonephritis. In dogs with end-stage kidney, the number of obsolescent glomeruli and cystic atrophied glomeruli was increased at T1. However, progression of the glomerular lesions was minimal in most dogs. Worsening of tubulointerstitial scores was evident in the dogs with the most severe lesions at the first biopsy. Progression of the tubulointerstitial damage was minimal in the mildly affected dogs, and the interstitial inflammation was abated. In conclusion, renal lesions can progress over a 60-day period in canine leishmaniasis. A longer period between the renal biopsies would be necessary to demonstrate more severe changes. In addition a specific anti-Leishmania treatment could have a significant effect in the early stages of the disease.
Canine leishmaniasis due to Leishmania infantum is a major cause of renal disease in Italy. 20 The renal damage in canine visceral leishmaniasis is thought to be a multifactorial process that is caused by immune complex deposition; however, a recent study has also highlighted the role of T lymphocytes and adhesion molecules. 8 Immune complex deposition can be the consequence of persistent antigenemia and circulating immune complexes; the process typically triggers the activation of the complement system and causes acute injury to the glomerular capillaries and mesangium. The severity of the tubulointerstitial damage is probably linked to the progression of the disease. 17,19 In dogs with nephropathy from naturally acquired visceral leishmaniasis, diffuse membranoproliferative and mesangioproliferative glomerulonephritis appear to be the most common histologic patterns. 3,4,6,10,15,20 No data on follow-up biopsies at the conclusion of treatment in Leishmania-infected dogs have been published. The objective of this study was to analyze the morphologic and ultrastructural changes in 15 symptomatic dogs that were serologically positive for Leishmania spp.; these dogs were biopsied at diagnosis and again at the end of treatment with a specific anti-Leishmania pharmacological agent. Immunohistochemistry was also performed to characterize the interstitial inflammatory infiltrate.
Materials and Methods
Case Selection
Fifteen dogs, seropositive for Leishmania spp., were selected from a shelter. The selected dogs had a serum titer > 1:160 by indirect fluorescent antibody test and had Leishmania amastigotes in fine-needle aspirate samples of sternebral bone marrow. 12 The dogs were treated with a leishmanicidal pharmacologic compound without supportive therapy for chronic renal failure. The study was performed in accordance with an approved Institutional Animal Care and Use Committee protocol.
Sample Collection
A percutaneous ultrasound-guided biopsy specimen was collected from the caudal pole of the left kidney at diagnosis (T0) using a True-cut disposable biopsy needle. A second biopsy was performed on the caudal pole of the right kidney 60 days later (T1). All biopsy specimens were divided for light and electron microscopy. Blood and urine samples were also obtained at T0 and T1.
Light Microscopy
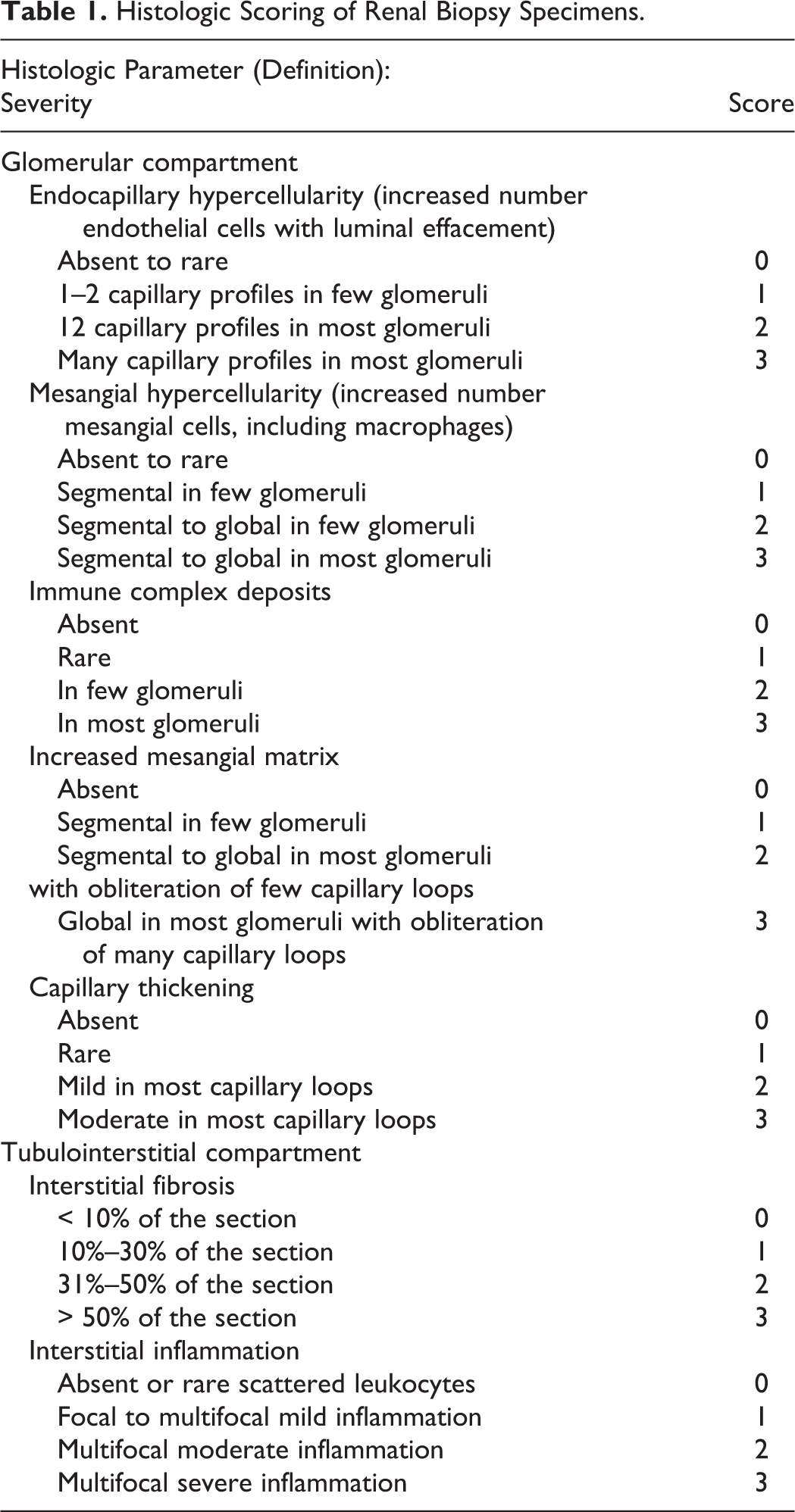
For histopathology, renal tissue was fixed in 10% neutral buffered formalin, processed routinely, and embedded in paraffin. Serial 3-µm sections were stained with hematoxylin and eosin (HE), Masson’s trichrome, periodic acid–Schiff, acid fuchsine orange G (AFOG) and Jones’ methenamine silver. Histologic sections were evaluated and scored (Table 1) independently by 2 authors without knowledge of the clinical data; any interobserver discrepancy in grading was resolved by arbitration. The histologic diagnoses were categorized according to the World Health Organization classification of human glomerular diseases. 5,9 A diagnosis of glomerulonephritis was corroborated by the finding of characteristic electron-dense deposits ultrastructurally. Renal lesions classified as mesangioproliferative glomerulonephritis had increased mesangial cells and matrix with no involvement of the capillary lumen, and immune deposits were found in the mesangium at electron microscopy. Chronic glomerulosclerosis was characterized by increased mesangial matrix with or without hypercellularity and absence of immune deposits. End-stage kidney was characterized by severe glomerular damage with obsolescence of > 40% of the glomeruli, severe tubular atrophy and fibrosis, and few electron-dense deposits in the basement membrane and in the mesangium. In membranoproliferative glomerulonephritis, glomeruli had increased mesangial matrix and cellularity and thickened glomerular capillary walls with immune complexes in the basement membrane and mesangium, cellular interposition, and new basement membrane formation.
Histologic Scoring of Renal Biopsy Specimens
Electron Microscopy
For transmission electron microscopy (TEM), the tissue was postfixed in osmium (2% in distilled water) for 1.5 hours, dehydrated in graded acetone, and embedded in Epon. Semithin sections were stained with azure-methylene-blue. Ultrathin sections were contrasted with uranyl acetate and lead citrate and examined with a Philips EM 420 transmission electron microscope.
Immunohistochemistry
For immunohistochemistry, serial paraffin sections were cut at 4-μm thickness on surface-coated slides (Superfrost®Plus). Slides were incubated at 37°C for 30 minutes before immunohistochemistry, which was performed with an automatic immunostainer (Ventana Benchmark XT, Roche-Diagnostics, Monza, Italy). The immunostainer uses a kit with a secondary antibody with a horse radish peroxidase–conjugated polymer to enhance the signal (ultraViews Universal DAB, Ventana Medical System Inc.). All reagents are dispensed automatically except for the primary antibody, dispensed by hand. Antibodies against CD3 (clone F7.2.38, Dako Italia Milano-Italy) and CD79acy (clone HM57, Dako Italia Milano-Italy) were used to detect T lymphocytes and B lymphocytes, respectively; incubation time was 20 minutes at 37°C. For negative controls, the primary antibody was replaced by antibody diluent; sections of hyperplastic lymph node were used as positive controls.
Clinical Chemistry
Total urinary protein and urinary creatinine were quantified by Pyrogallol red direct colorimetric method (Sentinel Diagnostics, CH) and Jaffé enzymatic colorimetric method (Sentinel Diagnostics–CH, Hitachi 911, Roche), respectively. Samples with very high urinary protein were diluted with sterile saline (1:3 or 1:10). For measurement of urinary creatinine, all samples were diluted 1:10, as recommended by the manufacturer.
Results
The median age at T0 was 4.5 years (range, 2.6–7.7 years). Renal biopsy specimens varied from 10 to 17 mm long × 2 mm thick; each histologic section contained an average of 19 glomeruli (range, 15–37).
At T0 biopsy, a wide spectrum of glomerular lesions was evident. Membranoproliferative and mesangioproliferative glomerulonephritis were observed in 6 dogs, chronic glomerulosclerosis in 5, end-stage kidney in 3, and no lesions in 1 case. Biopsy specimens were evaluated by electron microscopy in all dogs; the most striking glomerular lesion in 9 dogs was the presence of electron-dense deposits in various sites. Seven dogs had a multifocal and moderate distribution of lymphocytes and plasma cells in the renal interstitium. The mean inflammation score for all dogs was 1.9 (range, 0–3). At T1, progression of the glomerular lesions was minimal in most dogs. Interstitial fibrosis was stable or increased; the mean interstitial inflammation score (1.8; range, 0–3) was not significantly different. Histological evaluation and scoring at T0 and T1 are summarized in Table 2.
Light Microscopic Evaluation of Sequential Renal Biopsy Specimens in 15 Leishmania-Seropositive Dogs
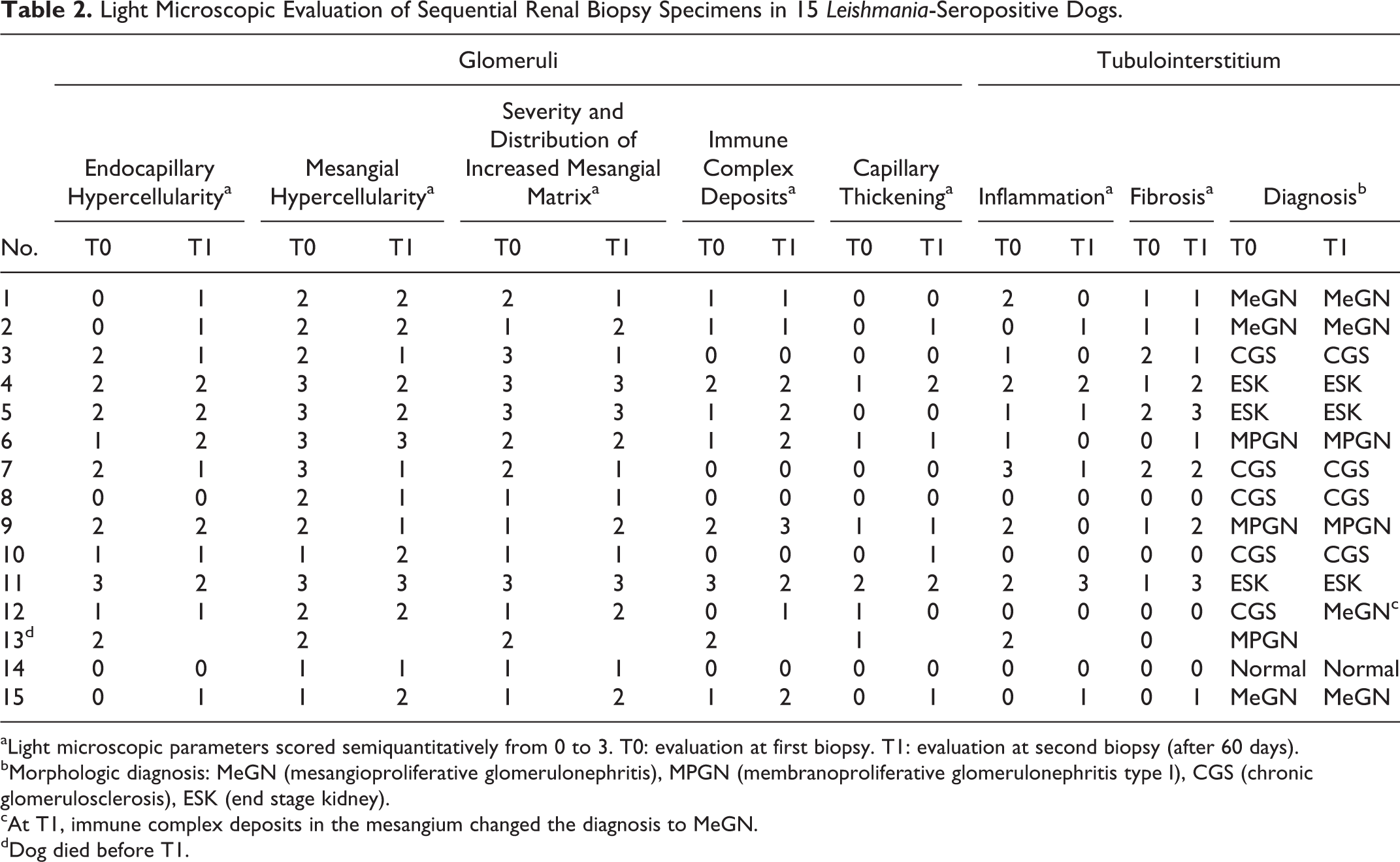
aLight microscopic parameters scored semiquantitatively from 0 to 3. T0: evaluation at first biopsy. T1: evaluation at second biopsy (after 60 days).
bMorphologic diagnosis: MeGN (mesangioproliferative glomerulonephritis), MPGN (membranoproliferative glomerulonephritis type I), CGS (chronic glomerulosclerosis), ESK (end stage kidney).
cAt T1, immune complex deposits in the mesangium changed the diagnosis to MeGN.
dDog died before T1.
Normal Dog
At T0, dog No. 14 was considered within normal limits, with only a few glomeruli having minimal and segmental increase in mesangial cellularity and matrix. At electron microscopy, mild and multifocal foot-process effacement was presented. Neither interstitial fibrosis nor inflammation (except for rare CD3+ lymphocytes) was evident. At T1, glomerular and tubulointerstitial scores were similar to those for the T0 biopsy specimen, as were the electron microscopic results.
Mesangioproliferative Glomerulonephritis
The diagnosis for dog Nos. 1, 2, and 15 was mesangioproliferative glomerulonephritis. The glomeruli had a moderate increase in mesangial matrix and mesangial hypercellularity (Fig. 1). Most podocytes were hypertrophied with karyomegaly and 1 or more large cytoplasmic vesicles. With Jones’ methenamine silver stain, multiple mesangial holes (2 µm in diameter) were observed. Overall, the glomerular basement membrane (GBM) had normal thickness. Two dogs (Nos. 2 and 15) lacked tubulointerstitial inflammation; 1 dog (No. 1) had multifocal moderate lymphoplasmacytic infiltrate. Fibrosis was absent in dog 15 and scored as 1 in dog Nos. 1 and 2. Ultrastructural electron-dense deposits were in the mesangium and in the subepithelial surface of the GBM overlying the mesangium (paramesangium). At T1, segmental endocapillary hypercellularity (absent at T0) was observed in a few glomeruli. Ultrastructurally, the GMB was segmentally thickened due to mesangial cell interposition, and mesangial immune complex deposits had a similar distribution to that at T0. Tubulointerstitial changes were mild, and in dog No. 1, no leukocytes were detected. At T1, mesangial and paramesangial deposits were still present.
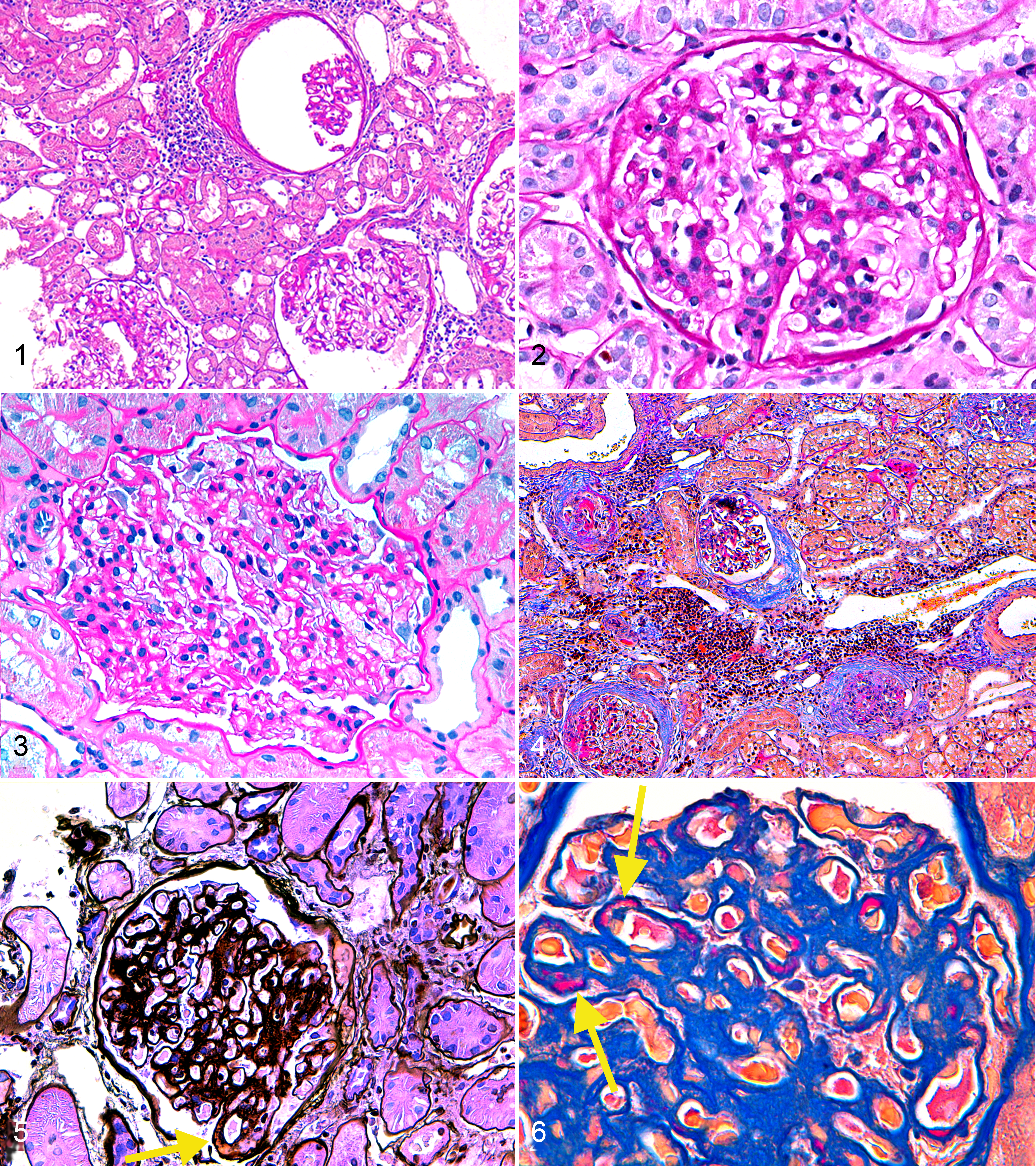
Kidney; dog No. 15. Glomeruli with dilated urinary space, with thickening and splitting of the capsule in a mesangioproliferative glomerulonephritis. HE.
Chronic Glomerulosclerosis
At T0, 5 dogs (Nos. 3, 7, 8, 10, and 12) were diagnosed with chronic glomerulosclerosis and lacked immune complex deposits. Three dogs (Nos. 8, 10, 12) had mild glomerular lesions with diffuse, mild to moderate expansion of the mesangium and minimal segmental mesangial hypercellularity (6 mesangial cell nuclei per mesangial area; Figs. 2, 3) and rare obsolescent glomeruli. Electron microscopy confirmed the histologic lesions, and no electron-dense deposits were detected at T0. Multifocal foot-process effacement was also observed. No tubulointerstitial inflammation was evident except for rare CD3+ lymphocytes, which were not associated with tubular damage. At T1, glomerular and tubulointerstitial scores were similar to those at T0. Electron-dense deposits were detected in only 1 dog, in the mesangium, so the diagnosis for dog No. 12 was changed to mesangioproliferative glomerulonephritis.
Dog Nos. 3 and 7 had more severe glomerular lesions. Global and diffuse glomerular lesions, with increased mesangial matrix and endocapillary and mesangial hypercellularity, were scored as 2 or 3 in the absence of GBM thickening or immune complex deposits. Many cystic atrophic or obsolescent glomeruli were observed. Electron microscopy confirmed the histologic lesions with multifocal expansion of mesangium and mesangial hypercellularity. Electron-dense deposits were not detected. Multifocal foot-process effacement was observed. These results were similar at T1. Interstitial damage included moderate multifocal fibrosis and variable degree of inflammation. At T1, glomerular lesions were moderate; the tubulointerstitium had reduced inflammation, but the fibrosis score remained mild to moderate.
End-Stage Kidney
Three dogs (Nos. 4, 5, and 11) had the most severe and chronic lesions, in both the glomerular and tubulointerstitial compartments. The glomerular tufts were irregular in shape, and the Bowman's capsules were markedly thickened. More than 40% of the glomeruli were obsolescent (Fig. 4); many were cystic and atrophic. Synechiae and GBM hyalinosis were segmentally present. The GBMs, where identifiable, were minimally to mildly thickened. Podocytes were diffusely hypertrophic; some contained protein resorption droplets and large cytoplasmic vacuoles. Ultrastructural lesions at T0 and T1 included multifocally increased mesangial matrix and cellularity (possibly including macrophages) with electron-dense deposits. The deposits were predominantly in the paramesangial regions. In addition, multifocal mesangial cell interpositioning was observed in the GBM. Interstitial damage was characterized by severe, multifocal fibrosis. However, the inflammation score for these dogs was low (mean score, 1.3), whereas the mean score for fibrosis was 2.6. At T1, the severity of fibrosis had increased.
Membranoproliferative Glomerulonephritis
In dog Nos. 6, 9, and 13, the diagnosis was membranoproliferative glomerulonephritis, with severe and global hypercellularity, and a lobulated appearance of the glomerular tufts. The hypercellularity was mainly mesangial, with lesser contributions from hypertrophic podocytes and an increased number of endothelial cells. The GBMs were moderately and globally thickened with multifocal membrane duplication, which indicated mesangial cell interpositioning (Fig. 5). The immune complex deposits in the capillary wall were accentuated with AFOG stain (Fig. 6). Electron-dense deposits were common in the mesangium and in the GBM at T0 and T1 (Figs. 7, 8), specifically, in the subepithelial, subendothelial, and intramembranous regions, often in association with interpositioned mesangial cells. All dogs had severe multifocal to confluent visceral epithelial cell foot-process fusion (Fig. 9). Tubulointerstitial lesions were mild and mainly inflammatory, with lymphoplasmacytic infiltration in all cases. Only dog No. 9 had interstitial fibrosis, scored as 1. Dog No. 13 died during the study period, so a T1 biopsy specimen could not be obtained. Other dogs at T1 had an increased number of immune complex deposits by light microscopy. Three parameters, increased mesangial matrix and mesangial and endocapillary hypercellularity, were scored 2 or 3 for global and diffuse glomerular involvement. The T1 tubulointerstitial inflammation score was reduced, but fibrosis score was increased in comparison to that at T0.
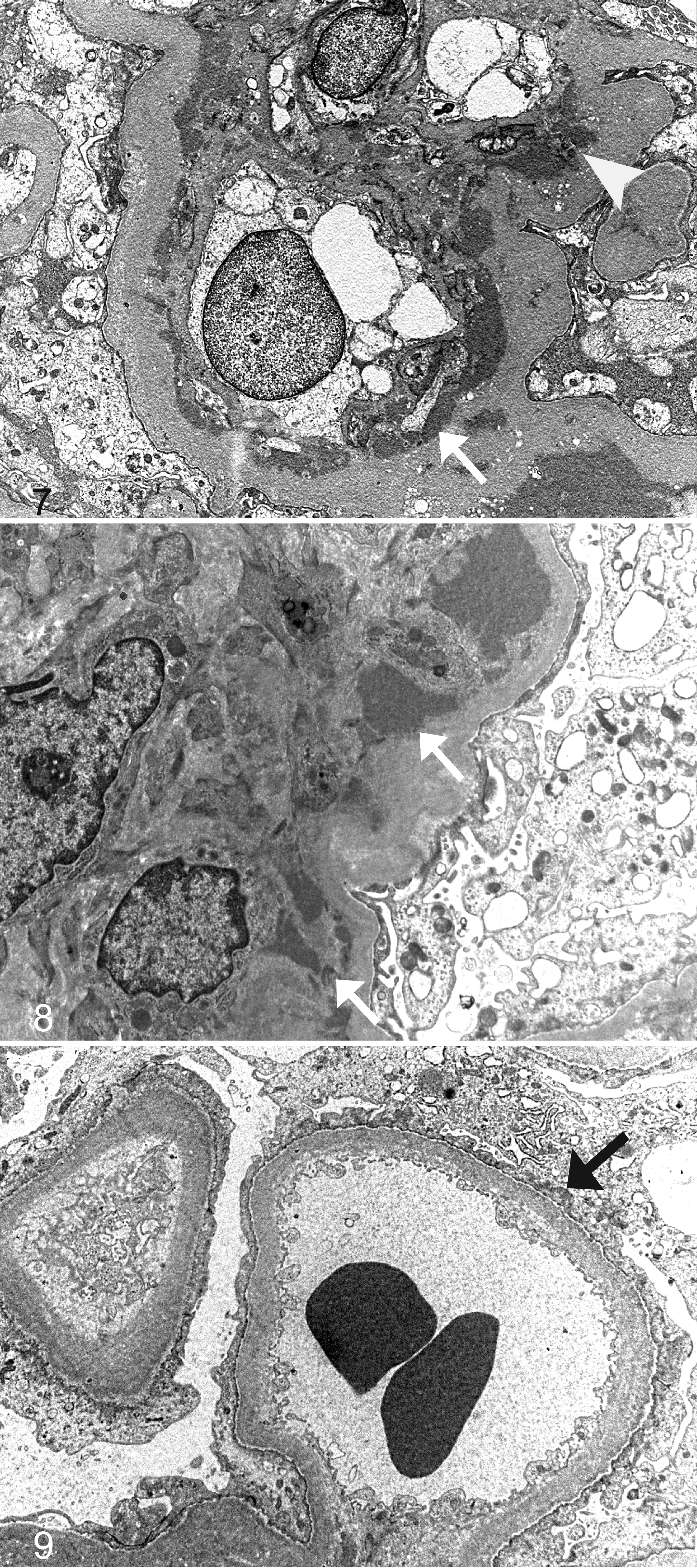
Renal glomerulus; dog No. 13. Segment of a capillary wall with large, discrete subendothelial (arrow), intramembranous, and mesangial electron-dense deposits. Transmission electron microscopy (TEM).
Immunohistochemistry
At both T0 and T1, the immunohistochemical analyses demonstrated that CD79a+ and CD3+ cells were equally distributed in the dogs. The majority of the CD79a+cells were plasma cells. The CD3+ lymphocytes were the most numerous lymphoid cell adjacent to tubules that were atrophied or contained luminal protein. The predominant leukocyte in areas of interstitial fibrosis was also the CD3+ lymphocyte.
Clinical Chemistry
At T0, 13 dogs (Nos. 1–7, 9–13, and 15) were proteinuric (urine protein: creatinine ratio > 0.3). The diagnosis for these dogs was membranoproliferative glomerulonephritis (n = 3), mesangioproliferative glomerulonephritis (n = 3), chronic glomerulosclerosis (n = 4), and end-stage kidney disease (n = 3). All the dogs, except dogs Nos. 10, 12, and 14, had increased serum creatinine (> 88.4 µmol/L). Clinical chemistry data are summarized in Table 3.
Urine Protein-Creatinine Ratio and Serum Creatinine in 15 Leishmania-Seropositive Dogs at First Renal Biopsy
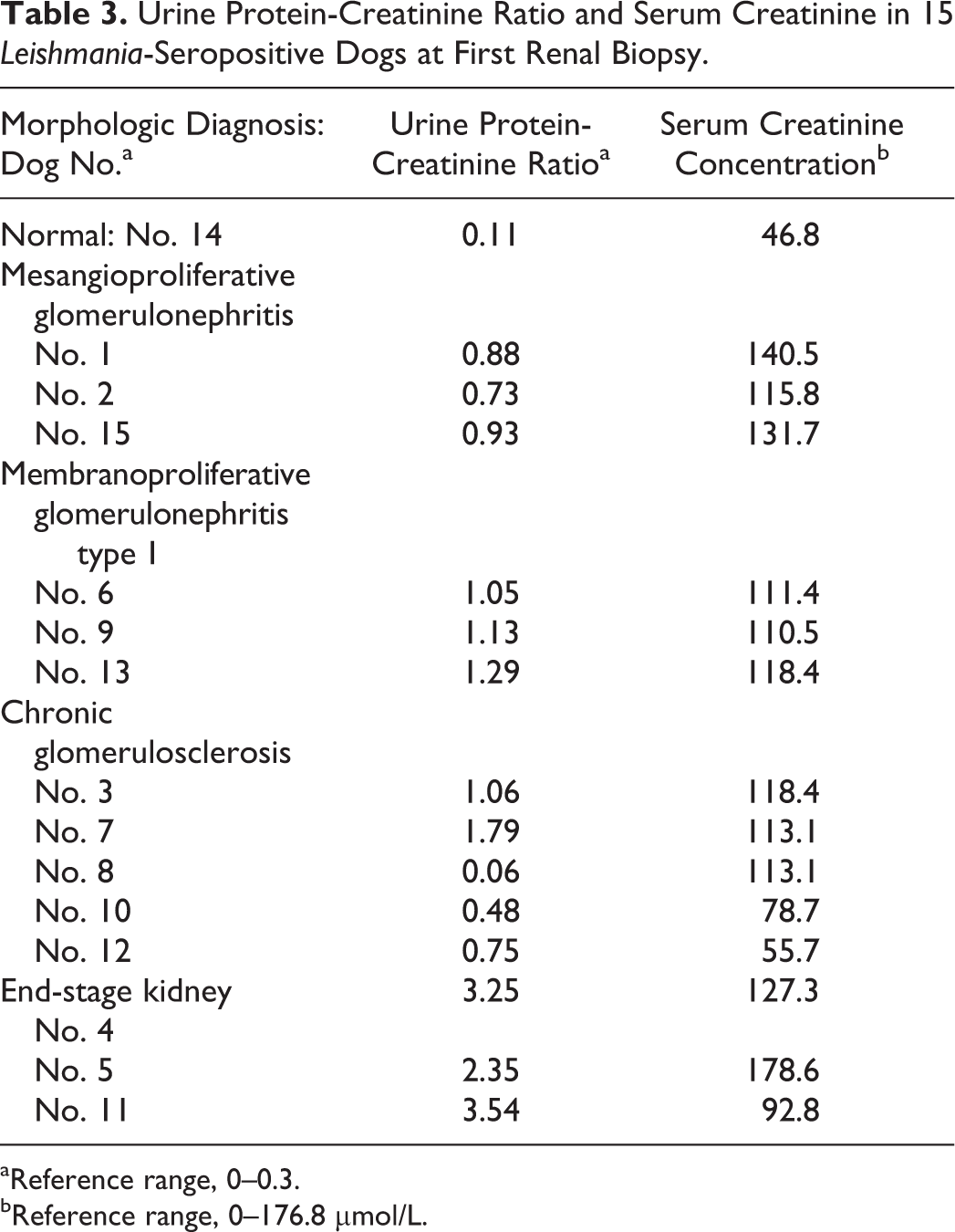
aReference range, 0–0.3.
bReference range, 0–176.8 μmol/L.
Discussion
Visceral leishmaniasis is a frequent cause of renal damage that evolves into progressive chronic kidney disease in dogs. 20 Membranoproliferative and mesangioproliferative glomerulonephritis are the most frequently reported lesions in affected dogs; 6,10 this trend is substantiated in the present study. The pathogenesis of the renal damage in Leishmania infection is not well defined; both a type III hypersensitivity mechanism and the involvement of CD4+ T cells have been proposed. 6 The glomerular proliferation pattern has also been attributed to an inhibition of mesangial cells apoptosis and the migration of inflammatory cells into the glomerular tuft. 8 In the current study, immune complex deposits were detected within the GBM and in the mesangium by electron microscopy, supporting a role of type III hypersensitivity in the renal damage during Leishmania infection. To our knowledge, sequential biopsy has not been used to evaluate histologic and ultrastructural progression of renal lesions in Leishmania-infected dogs.
The 15 dogs had various types of renal damage at T0, with a minimal progression of the glomerular lesions between the 2 sampling times in most dogs. However, in 1 dog, the finding of mesangial immune complex deposits at T1 prompted a change in diagnosis from chronic glomerulosclerosis to mesangioproliferative glomerulonephritis. This change could have been the result of progression of an early lesion with rare and small deposits that were not detected at the first biopsy. In contrast, greater change was detected in the tubulointerstitial compartment between the 2 samplings, with a reduction of the inflammation score in most dogs at T1. This could have been the result of the leishmanicidal treatment, which could have eliminated most parasites, thereby reducing the circulating antigens and, consequently, the immune-mediated glomerular damage. 13 Inflammation is part of an active process that might be reversible with the correct therapy. 1 Inflammatory cells are also known to contributed to fibrosis through the secretion of various cytokines. Both CD4+ and CD8+ T cells are the most important inducers of tubulointerstitial fibrosis; these cells promote the proliferation of fibroblasts and the production of the extracellular matrix mainly by stimulating the production of TGF-β, IL-4, TNF-α, and other fibroblast-stimulating factors. 19 Although T lymphocytes were not detected in glomeruli in the current study, Costa et al demonstrated the correlation of CD4+ T cells with the presence of Leishmania antigens in the pathogenesis of canine glomerulonephritis. 7,8 CD4+T cells may stimulate B cells to produce antibodies against circulating antigens, leading to the formation of large immune complexes that precipitate in the mesangium and GBM, and trigger the complement cascade. 11
In contrast to inflammation, fibrosis is considered an irreversible replacement of destroyed parenchyma by connective tissue 18 and is the most common pathogenic mechanism in the chronic failure of parenchymal organs, such as liver, kidney, and lungs. 2 In chronic glomerulosclerosis with mild glomerular lesions, fibrosis was absent at T0 and T1. The absence of detectable glomerular immune complex deposits and the minimal interstitial fibrosis could be key factors in the slow progression of the tubulointerstitial damage. Immune complex deposits in the glomerular capillary wall and in the mesangium promote inflammation, first in the glomeruli, then extending into the interstitium. The presence of the deposits alters the slit diaphragm with the consequent leakage of proteins into the urinary space. The resultant hemodynamic changes contribute to the reduction in glomerular filtration rate and expansion of mesangial matrix. 14 A progression of the fibrosis was observed in dogs with moderate to severe glomerular damage and in which the tubulointerstitial involvement was already evident at T0. Previous studies have also shown that, regardless of the glomerular lesions, most renal diseases that progress to chronic renal failure involve the interstitium and the tubules. 2,16,17,19 The mild progression of the tubulointerstitial damage in this study may reflect the short (a 60-day) interval between T0 and T1; a longer interval between biopsy samplings might uncover more significant changes. Dog Nos. 4, 5, and 11 had the most severe lesions. The main finding in these dogs was ischemic glomerular obsolescence (probably secondary to hypertension). In these 3 dogs, the T0 diagnosis was end-stage kidney disease; a more specific diagnosis could not be made due to the severity of the lesions. At the second biopsy, the severity of the fibrosis, and the number of obsolescent glomeruli and cystic atrophied glomeruli, had increased. The prognosis in such dogs is usually poor due to the severity and presumed irreversibility of the renal lesions.
In conclusion, the progression of renal lesions is described in dogs naturally infected by Leishmania. Despite the primary location of the lesions in the glomeruli, by the time damage is moderate, tubulointerstitial involvement is also evident. The lesions did progress between the first and second biopsies; however, a longer period between biopsies might allow detection of more severe changes. A specific anti-Leishmania treatment could reduce the tubulointerstitial inflammatory response, especially in the absence of glomerular immune complex deposits. In contrast, anti-Leishmania treatment may be less effective for glomerulonephritis and renal interstitial fibrosis. Thus, supportive treatment for chronic renal failure is recommended for the dogs with visceral leishmaniasis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.