
Abstract
The goal of this study was to determine if cartilage lesions of the humeral head in adult dogs are the consequence of osteochondrosis dissecans or degenerative joint disease. A gross and histologic survey was performed of humeral head cartilage lesions of 155 dogs ranging in age from 1 week to 19 years. The humeral head and cartilage lesion size were measured for each dog. Cartilage lesions were classified as fibrillation, fissures, erosion, and/or eburnation. The area of each lesion was multiplied by a severity score (fibrillation and fissures 1, erosion 2, and eburnation 3) to create a combined score for each humeral head. Correlations between this combined lesion score and age, humeral head size, body weight, and body condition score were assessed using a Bonferroni-corrected alpha of .01. Twenty-six humeral heads were also evaluated histologically. Of the 155 dogs, 80 (52%) had gross lesions of the articular cartilage. The presence and severity of the articular cartilage lesions were positively correlated with age, humeral head size, body weight, and body condition score. The average age of dogs with cartilage lesions was 8.8 years, and 77/105 (74%) of adult dogs had cartilage lesions. Fifty dogs were 3 years of age or younger; 3 of those had cartilage lesions, 1 of which was osteochondrosis. These data indicate that cartilage erosion of the caudal humeral head in dogs is a common degenerative lesion acquired in adult large breed dogs; osteochondrosis dissecans does not precede the lesion in the vast majority of cases.
Degenerative joint disease (DJD, also known as osteoarthritis) is common in adult large breed dogs. 19 Cartilage lesions such as fissures, fibrillation, erosion, and eburnation are often found in the hip, shoulder, and stifle joints of dogs at necropsy, even without a clinical history of lameness.15,19 Cartilage lesions of the hip and stifle joints are typically attributed to joint instability and subsequent DJD, but similar lesions on the caudal humeral head are often attributed to osteochondrosis dissecans (OCD) rather than DJD, even in adult dogs. The purpose of this study was to determine whether cartilage lesions of the caudal humeral head develop in adult dogs (as expected with DJD) or appear during the growth period and persist throughout life (as expected with OCD).
Materials and Methods
Every dog submitted to the University of Tennessee College of Veterinary Medicine for complete necropsy during a 12-month period (2010) was evaluated for humeral head lesions. The length and width of the humeral heads and the length and width of grossly visible cartilage lesions were measured. The character of the lesions (fissures, fibrillation, erosion, or eburnation) was evaluated grossly. The breed, sex, weight, and body condition score were also recorded at the time of necropsy. The age of the dog was taken from the necropsy submission form. Selected humeral heads (26 dogs, selected to represent the range of gross lesions) were decalcified in 15% formic acid and processed routinely for histologic evaluation.
The gross size of each cartilage lesion was multiplied by a severity score (1 for fissures or fibrillation, 2 for erosion, and 3 for eburnation) to calculate a combined lesion score for each humeral head. A nonparametric paired samples test (Wilcoxon signed ranks test) was used to compare right to left humeral head size and lesion score, before taking the average of the 2 side measures. The nonparametric Spearman’s rank correlation was used to assess the association between the averaged lesion score and other continuous variables (such as age, weight, and body condition score). The effect of sex on lesion severity was tested using the nonparametric Mann–Whitney test. Because of the increasing chance of committing a Type I error with multiple testing, a Bonferroni alpha correction was used for each set of statistical tests. A Pearson chi-square test was used to determine if breed size was independent of age.
Results
A total of 309 humeral heads from 155 dogs were examined (one dog was an amputee). Of the dogs, 80 (52%) had gross lesions; 77 (96%) of the affected dogs were over 3 years of age. There was no significant difference between the severity of lesions of the right and left humeral heads and lesion severity did not differ significantly by sex. The presence and severity of articular cartilage lesions were positively correlated with age (Fig. 1), body weight (Fig. 2), humeral head size (Fig. 3), and body condition score of 5/5 (Fig. 4) (Bonferroni-corrected alpha = .01). There were too few dogs of each breed to test breed correlations.
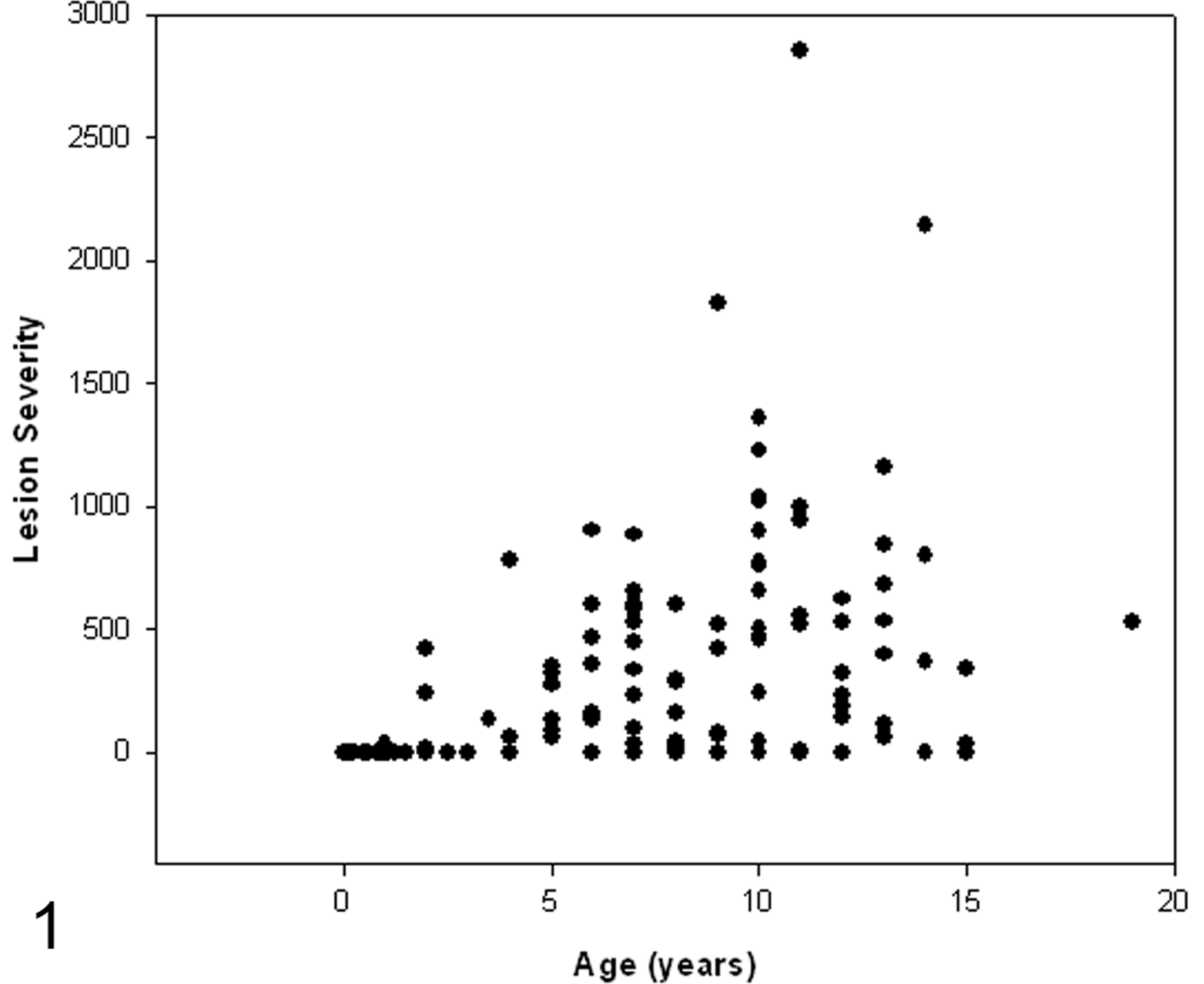
Combined lesion severity score plotted against age in years for 155 dogs. The lesion severity score was calculated by multiplying the size (in millimeters) of the cartilage lesion, by a factor according to the depth of the lesion, and combining the scores for each humeral head. Lesions were more common and more severe in middle-aged and older dogs.
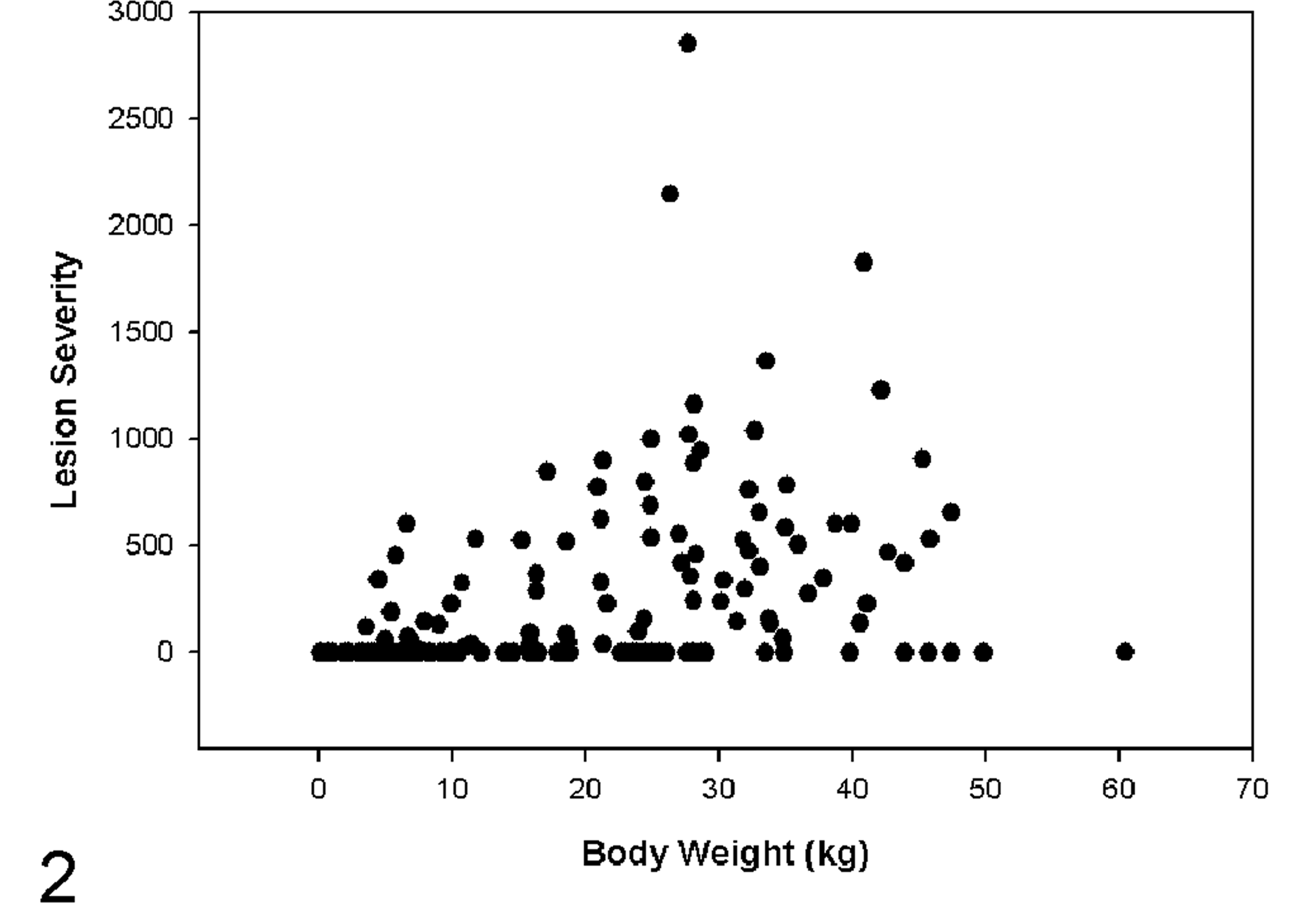
Combined lesion severity score plotted against body weight in kg for 155 dogs. The lesion severity score was calculated as in Fig. 1. Lesions were more common and more severe in larger dogs.
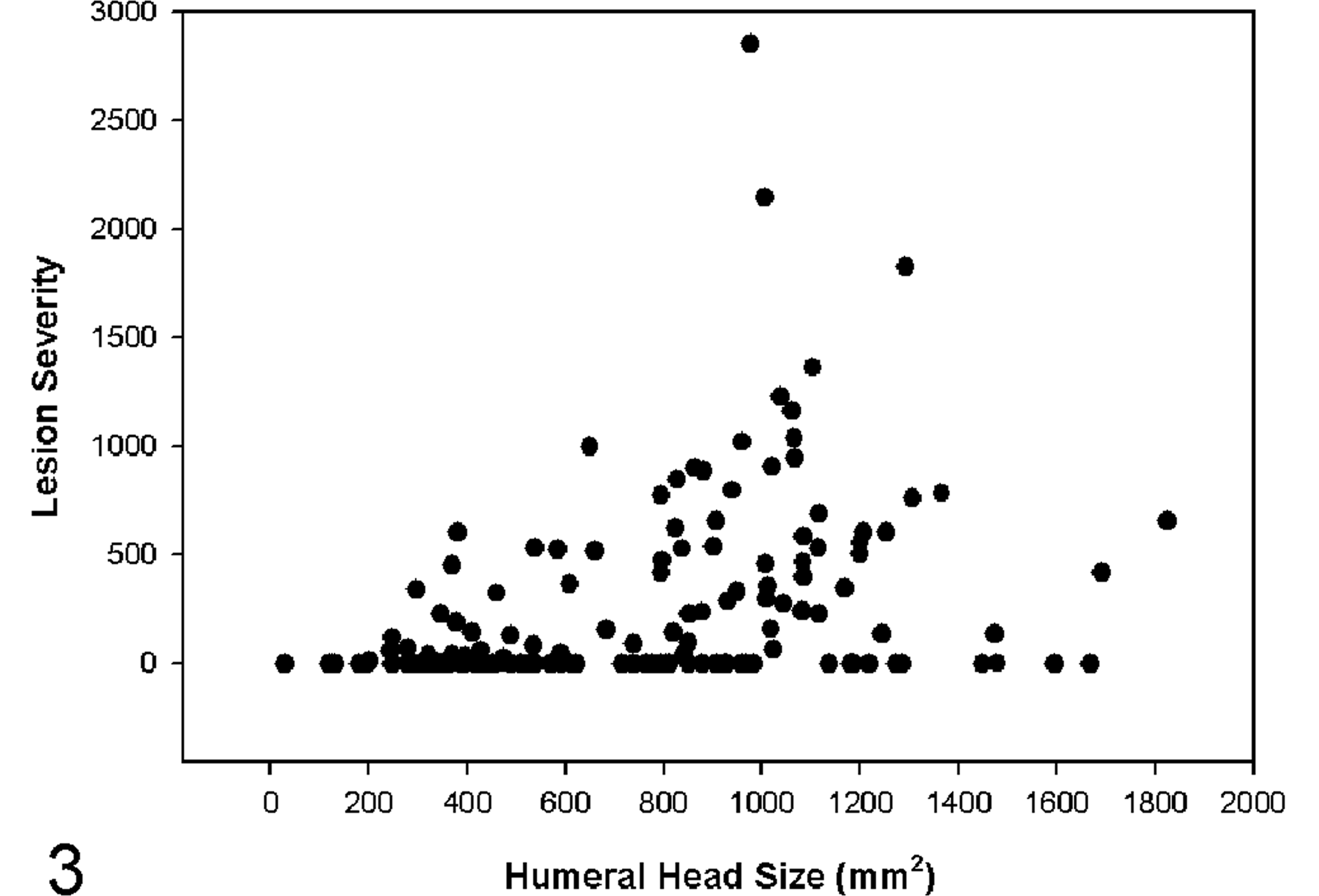
Combined lesion severity score plotted against humeral head size in millimeters (width times length) for 155 dogs. The lesion severity score was calculated as in Fig. 1. Lesions were more common and more severe in dogs with larger humeral heads.
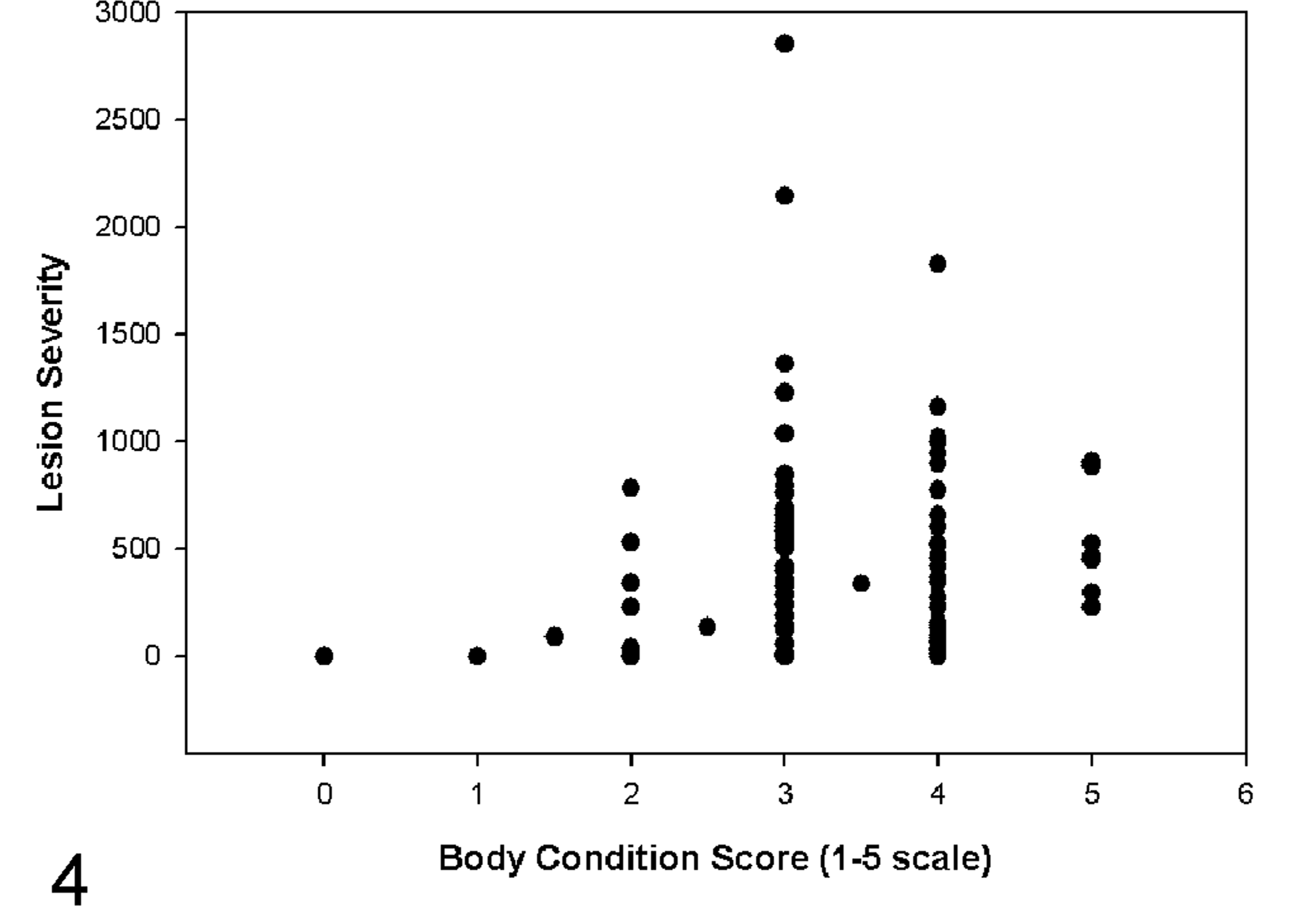
Combined lesion severity score plotted against body condition score for 155 dogs. The lesion severity score was calculated as in Fig. 1. Lesions were more common and more severe in dogs with a higher body condition score.
The average age of dogs with cartilage lesions was 8.8 years. None of the gross lesions in adult dogs resembled OCD, and of the 13 adult humeral heads examined histologically, none had histologic lesions of OCD (ie, the cartilage lesion only involved the superficial cartilage without any deep cartilage necrosis). The cartilage lesions were typically on the caudal humeral head (Fig. 5). Deeper lesions, such as deep erosions and eburnation were often surrounded by more superficial erosions or fibrillation. Histologically, the lesions were characterized by fissures, fibrillation, and/or erosion with loss and clustering of superficial chondrocytes and decreased cartilage matrix staining (Fig. 6). None of the lesions in adult dogs had deep areas of cartilage necrosis or fibrocartilage proliferation characteristic of OCD. One dog (a 10-year-old Golden Retriever) had histiocytic sarcoma causing bone necrosis and collapse of the overlying cartilage.
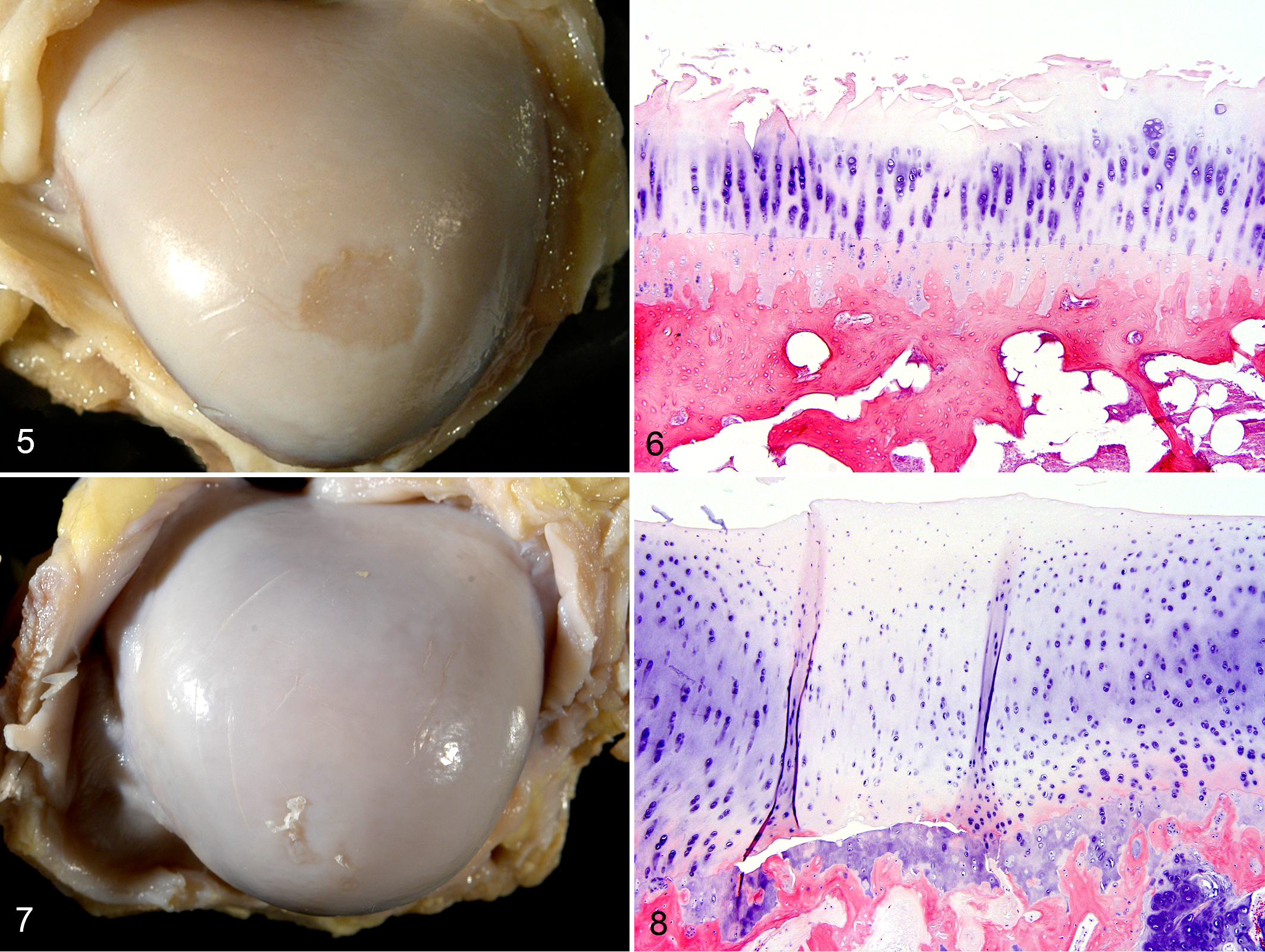
Humeral head, 9-year-old Chow mix dog, case no. 102. There is a discrete area of cartilage erosion on the caudal humeral head (degenerative joint disease). The articular cartilage is diffusely yellow-brown.
There were 50 dogs 3 years of age or younger; 3 (6%) of those had cartilage lesions. Of these, 2 were consistent with early DJD (fissures and fibrillation), and 1 (from an 18-month-old Newfoundland) was consistent with mild (1 mm diameter) OCD (Figs. 7 and 8).
To ensure that the low number of OCD lesions in the 50 younger dogs was not due to breed differences, all dogs were categorized as small, medium, or large breed, based on breed or adult weight. Using these categories, the 50 dogs 3 years of age or younger were 36% (18/50) small breed, 10% (5/50) medium breed, and 54% (27/50) large breed. The 105 dogs over 3 years of age were 30% (31/105) small breed, 10% (11/105) medium breed, and 60% (63/105) large breed. The difference in the percentages of small breed dogs between the 2 groups was not statistically significant (P = .716).
In both younger and older groups of dogs, the average age and weight of affected dogs was slightly higher than unaffected dogs. In dogs 3 years of age or younger, the average age of affected dogs was 1.6 years versus 1.2 years for unaffected dogs; the average weight of affected dogs was 31.7 kg versus 12.9 kg for unaffected dogs. In dogs over 3 years of age, the average age of affected dogs was 9.3 years versus 8.3 years for unaffected dogs; the average weight of affected dogs was 24.2 kg versus 18.1 kg for unaffected dogs.
Eight of the 77 affected adult dogs had eburnation, which could have masked preexisting OCD. Three of the 8 dogs with eburnation were examined histologically; none had retained cartilage in the epiphysis, as was seen in the OCD-affected 18-month-old Newfoundland.
Discussion
The correlation of cartilage lesions with increasing age indicates that they are age-acquired DJD lesions, rather than OCD. If the lesions had begun as OCD, then they would be present at all ages, rather than appearing in middle-aged and older dogs. In addition, they would be characterized by deep cartilage necrosis, rather than superficial fibrillation and erosions. Studies that have followed the development of humeral head cartilage lesions in research beagles 12 and food-restricted Labrador Retrievers 17 have reported a similar association of cartilage erosion with age. Nevertheless, there is a common perception that most cartilage defects in the caudal humeral head of dogs are the result of OCD, regardless of the age of the dog.
The pathogenesis of the age-associated DJD of the canine shoulder is likely similar to that in other joints, with increasing joint laxity contributing to cartilage wear. 1 Instability is increasingly recognized as the most common cause of shoulder lameness in adult dogs.2–4,16 The gross and histologic lesions of fissures, fibrillation, erosion, and eburnation seen in this study are similar to those previously reported in DJD of the canine shoulder, 10 hip, 13 and stifle. 5 One contributing factor to shoulder instability may be the depth of concavity of the glenoid, 9 similar to the shallow acetabulum contributing to hip dysplasia. No attempt was made in this study to measure joint laxity or glenoid concavity. Interestingly, dogs with hip dysplasia have been found to have changes in their humeral head articular cartilage that indicate a predisposition to DJD of the shoulder. 6 Cartilage lesions of DJD are often present in both the hip and shoulder joints at necropsy, even in dogs without a clinical history of lameness.15,19 The dogs in this study were submitted for necropsy following death or euthanasia for a variety of causes; the history rarely included concurrent conditions, such as chronic lameness.
High body condition score (5/5) was correlated with severity of humeral head cartilage lesions in this study. This supports the link between obesity and DJD in dogs. 11 Studies have shown that lifetime food restriction in Labrador Retrievers decreases the development of DJD of the canine shoulder;8,17 as it does in other joints. 18
OCD is the most common lesion found in young, large breed dogs undergoing shoulder arthroscopy. 14 Osteochondrosis is a disorder of growing cartilage which may manifest as deep necrosis of the articular cartilage (osteochondrosis latens), radiographically and/or grossly visible failure of endochondral ossification (osteochondrosis manifesta), or a dissecting band of necrosis forming a flap of articular cartilage (OCD). 20 The term osteochondrosis dissecans is preferred to osteochondritis dissecans, since the lesion is not inflammatory. 20 Young dogs with OCD may be treated with surgical removal of the cartilage flap and debridement of the underlying bone; this defect is then replaced with fibrocartilage. 7 None of the dogs in this study had fibrocartilage on the articular surface. One dog (an 18-month-old Newfoundland) had a 1 mm diameter OCD lesion, which was unlikely to have caused clinical lameness; the eventual outcome of such small lesions is unknown. The rarity of significant OCD lesions in this study is likely a reflection of the small percentage of dogs affected compared to the overall canine population. While OCD may be common in young, large breed, dogs with shoulder lameness, these compose a very small proportion of the entire canine population. Conversely, DJD of the shoulder is very common in dogs, especially middle-aged and older large breed dogs. In this study 77/105 (74%) of adult dogs had cartilage lesions consistent with DJD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.