
Abstract
Cryptococcus neoformans var. grubii was identified at necropsy in a case of bilateral otitis interna in a 7-year-old, female, domestic shorthair cat with a 9-day history of acute onset of vestibular disease. Gross examination, including that of the middle and inner ears, was unremarkable. Histologically, the auricular vestibuli, cochleae, and semicircular canals were bilaterally affected by granulomatous inflammation with extracellular and intrahistiocytic yeasts. The yeasts and associated inflammation obstructed and disrupted perilymphatic and endolymphatic spaces of the inner ears. Disruption of the saccular and utricular maculae, cristae ampularis, and organ of Corti, as well as changes in the endolymphatic and perilymphatic fluids, probably impaired the vestibular and auditory functions of this cat. The route of infection was most likely hematogenous.
In domestic animals, otitis interna usually results from an extension of middle ear bacterial infection, and otitis media likewise commonly extends from infections of the external ear canal or from the upper respiratory tract via the auditory tube. In domestic cats, otitis media and interna also can be associated with inflammatory polyps or be a complication of aural neoplasms. Otitis interna may lead to signs of peripheral vestibular disease.
Case Presentation
A 7-year-old, 3.9-kg, female domestic shorthair cat in good nutritional condition was presented with an acute onset of disequilibrium (falling to both sides) and a skewed head posture but normal mentation and appetite. After a 9-day hospitalization without clinical improvement, the cat was euthanized.
Necropsy and Laboratory Findings
At necropsy, no gross lesions were present. Aerobic bacterial cultures of brain, lung, and liver and direct fluorescent antibody test for rabies yielded negative results. Cryptococcus neoformans var. grubii was identified and confirmed by polymerase chain reaction (PCR) test 6 by the British Columbia Centre for Disease Control Public Health Microbiology and Reference Laboratory in formalin-fixed, paraffin-embedded samples of brain, liver, lung, intestine, and inner ear and in frozen brain (frontal lobe).
Tissue samples were fixed in 10% neutral buffered formalin; osseous tissues were decalcified with Formical4. Sections of major organs were trimmed, including 24 transverse sections of brain, and sections of nasal cavity and cribriform plate. The petrous portion of the temporal bone, tympanic bulla, and external ear canal were trimmed transversely, and both halves were processed for histopathology (Fig. 1). Tissue samples were embedded in paraffin according to standard histologic technique. For histologic evaluation of the inner and middle ears, 50 serial sections were produced representing the posterior, middle, and anterior aspects of each inner ear. The sections were stained with hematoxylin and eosin (HE), Grocott’s methenamine silver (GMS), periodic acid-Schiff (PAS), and Alcian blue (pH 2.5). An age-matched cat without clinical disease or histologic lesions was used as control for the histology of the inner ear.
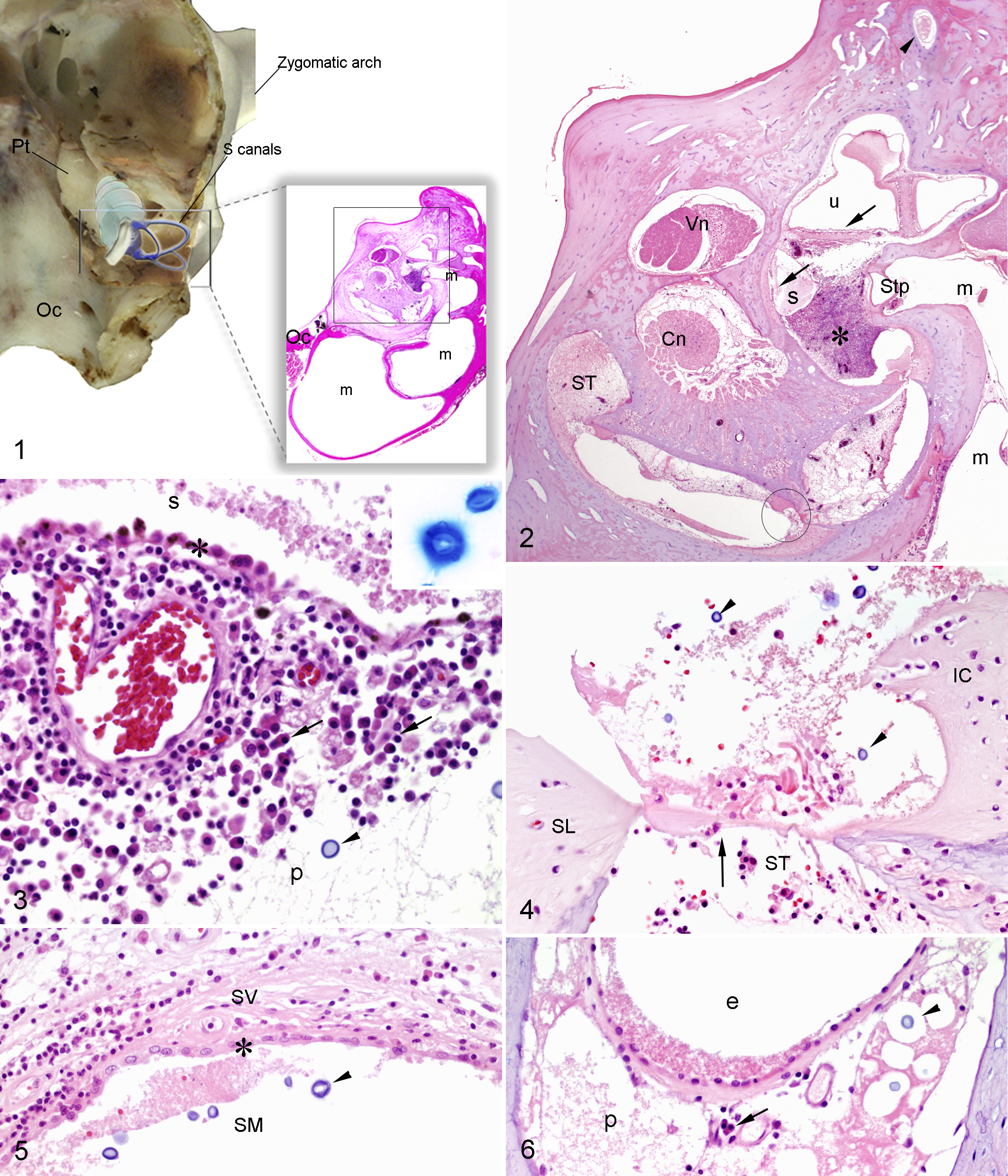
Right base of the skull; cat. Illustration of the transverse plane of section for histology of the temporal bone. Inset: subgross view of the tympanic bulla and inner ear (area within square is shown in Fig. 2). Middle ear (m), basilar occipital bone (Oc), petrous portion of the temporal bone (Pt), and semicircular canals (S canals). The middle ear is free of exudate. Hematoxylin and eosin (HE).
Histologic Examination
The salient histopathologic findings were detected bilaterally in the inner ears and affected the vestibules, cochleae, semicircular canals and ducts, sacculi, and utriculi (Fig. 2). A granulomatous inflammation consisting of lymphocytes, plasma cells, and macrophages affected the endolymphatic and perilymphatic spaces of the vestibular and auditory systems. The inflammation partially obliterated the perilymphatic space near the vestibular window. The saccular membrane was lined by hypertrophied epithelial cells (Fig. 3) and was segmentally fragmented. Throughout the inner ear and in association with the inflammation, numerous extracellular and intrahistiocytic yeasts, morphologically consistent with Cryptococcus sp., were found. The yeasts measured 10 to 15 μm in diameter. The yeast wall was 1 μm thick and PAS and GMS positive, and the capsule was 5 to 8 μm thick and Alcian blue positive (Fig. 3, inset).
A variable amount of cellular debris, fibrin, and proteinaceous material was in the vestibular and cochlear perilymphatic and endolymphatic spaces. Cochlear inflammation and granulation tissue extended from base to apex. The boundaries between the scalae tympani, vestibuli, and media were disrupted or indistinct. Portions of the scala tympani and scala vestibuli perilymphatic space were obliterated by granulation tissue. The scala media had total loss of the organ of Corti (Fig. 4). Reissner’s membrane was lined by hypertrophied epithelium and disrupted by the fibroplasia and inflammation of the scala vestibuli (Fig. 5). Semicircular canals (Fig. 6) had subtle leukocytic infiltration, proteinaceous fluid, and yeasts in the perilymphatic space. Occasionally, the epithelial cells lining semicircular ducts appeared mildly reactive.
The middle ear and external ear canal were not affected. Occasional mild lymphoplasmacytic and histiocytic infiltrates were in the cerebral leptomeninges. A single, 1 mm in diameter, focus of inflammation with 3 yeasts was detected in the thalamus. No fungi or inflammation was detected in other tissues, including the cerebellum, brainstem, spinal cord, nasal cavity, lungs, and other major organs.
Discussion
This cat had chronic bilateral otitis interna, with cochleitis, sacculitis, and utriculitis, accompanied by degeneration and loss of sensory receptors. The damage to sensory structures of the vestibular and auditory systems affected the cat’s balance and hearing, respectively. The composition of the inner ear fluids is tightly regulated and essential for normal function of otolith organs and cochlea.7,9 Inflammation, even in the middle ear, can alter the inner ear’s fluid composition. 5 Due to the limited regenerative capacity of vestibular and cochlear sensory cells in adult mammals, 3 severe injury, as seen in this cat, can lead to permanent impairment of balance and auditory function.
Clinical signs of bilateral peripheral vestibular disease include wide head excursions and loss of balance to either side in the absence of postural asymmetry or nystagmus. In contrast, unilateral peripheral vestibular disease typically causes postural asymmetry, circling, and nystagmus. 1 In this case, the cat had loss of balance to both sides and skewed head posture. Although its auditory functional status was not reported, it was probably affected as well based on the degree of cochlear lesions.
C. neoformans var. grubii is the most commonly isolated Cryptococcus species in domestic animals and people worldwide. 8 This pathogen is also a common cause of feline systemic mycosis and can manifest as focal or multifocal cutaneous nodules, upper respiratory infections, meningitis, or otitis media/interna. 4 Cryptococcal infection typically occurs through inhalation followed by adhesion and invasion of respiratory epithelial cells. Thereafter, C. neoformans can infect other organs hematogenously or via leukocyte trafficking or direct extension.
The route of inner ear infection in this case was probably hematogenous. No histologic evidence of infection was detected in the external ear canals, middle ears, auditory tubes, or vestibulocochlear nerve roots. The perilymphatic duct that provides communication between the inner ear and meninges could not be visualized, but its location, the posterior cranial fossa, was also free of inflammation or yeasts. Thus, infection via this structure appears unlikely. The detection of yeast by PCR in multiple organs also indicates that yeasts may have undergone hematogenous spread at some point during the infection.
Detailed histologic examination of the inner ear is rarely reported in the veterinary literature, even in animals with gait and vestibular abnormalities due to cryptococcosis. 10 The auditory apparatus is morphologically complex,2,7 so examination of the inner ear is time-consuming and requires meticulous trimming for histologic processing and examination of serial sections. Nevertheless, detailed histologic examination of the vestibule and cochlea is diagnostically important in cases with known inner ear disease or suspected neurologic disease.
Footnotes
Acknowledgements
The authors thank Dr James Collins and the Minnesota Veterinary Diagnostic Laboratory staff, Ms Rhonda Aho and Mr Edgar d’Almeida for technical support, and Mr Min-Kuang Lee, BC Centre for Disease Control Public Health Microbiology and Reference Laboratory, for molecular diagnostic work.
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.