
Abstract
Lymphoma is the most common malignant neoplasm in the horse. Single case reports and small retrospective studies of equine lymphomas are reported infrequently in the literature. A wide range of clinical presentations, tumor subtypes, and outcomes have been described, and the diversity of the results demonstrates the need to better define lymphomas in horses. As part of an initiative of the Veterinary Cooperative Oncology Group, 203 cases of equine lymphoma have been gathered from 8 institutions. Hematoxylin and eosin slides from each case were reviewed and 187 cases were immunophenotyped and categorized according to the World Health Organization classification system. Data regarding signalment, clinical presentation, and tumor topography were also examined. Ages ranged from 2 months to 31 years (mean, 10.7 years). Twenty-four breeds were represented; Quarterhorses were the most common breed (n = 55), followed by Thoroughbreds (n = 33) and Standardbreds (n = 30). Lymphomas were categorized into 13 anatomic sites. Multicentric lymphomas were common (n = 83), as were skin (n = 38) and gastrointestinal tract (n = 24). A total of 14 lymphoma subtypes were identified. T-cell–rich large B-cell lymphomas were the most common subtype, diagnosed in 87 horses. Peripheral T-cell lymphomas (n = 45) and diffuse large B-cell lymphomas (n = 26) were also frequently diagnosed.
Lymphoma is common in the horse and may have a highly variable clinical presentation and course. Although large-scale retrospective classification studies have been performed in other domestic species,49,50,53 no large-scale reports of equine lymphoma have been previously published to the best of our knowledge. Several individual equine case reports and small classification studies have been performed since the 1980s,1, 2, 4–11, 13–28, 30–45, 52 with a maximum sample population of 79 horses limited to ocular and periocular neoplasia. 37 Three studies have used immunophenotyping15,17,25 with differing results as to the most common immunophenotype of lymphoma.
Historically, as lymphoid neoplasms were described, multiple guidelines were attempted to categorize the disease.12,29 Most recently, the Revised European American Lymphoma (REAL)–World Health Organization (WHO) classification system, published in 2001 and updated in 2008, integrates knowledge of topography, cell morphology, immunophenotype, genetic features, and clinical presentation and course. This system has been validated with a greater than 85% agreement rate among pathologists and has achieved true international consensus. 12 A veterinary reference of the WHO classification system was published in 2002. 46 A project modeled after the study, which validated the WHO system in human lymphomas, was conducted for canine lymphomas in 2011 with nearly identical results: the overall accuracy of the 17 pathologists on the 300 cases of canine lymphoma was 83%. 50
The purpose of the current study is to review previously diagnosed cases of equine lymphoma, classify these cases via morphology and immunophenotyping according to the veterinary adaptation of the WHO guidelines, and describe the signalment, topographic or tissue distribution, and tumor category. To the authors’ knowledge, this is the first attempt at a large-scale retrospective equine lymphoma classification study. This study began as an initiative of the Veterinary Cooperative Oncology Group of the Veterinary Cancer Society.
Methods
Case Material
Cases included in this study consisted of a total of 204 horses with excisional or incisional biopsies (n = 63), necropsies (n = 113), both biopsy and necropsy (n = 14), or unknown samples (n = 14). Cases with a previous diagnosis of lymphoma were submitted from 8 different universities in the United States and Canada from 1975 to 2008 as a study begun by the Veterinary Cooperative Oncology Group of the Veterinary Cancer Society. The supporting institutions include Ontario Veterinary College (University of Guelph), Colorado State University, University of Wisconsin at Madison, Purdue University, University of Florida, University of Illinois, Ohio State University, and University of Pennsylvania.
Tissue specimens had been fixed in 10% neutral buffered formalin, routinely processed, and sectioned at 3 or 5 microns and stained with hematoxylin and eosin (HE). The medical records and pathology submission forms were reviewed retrospectively for patient data. For each case, signalment and tumor topography were recorded if available; presenting clinical data were also obtained for 109 cases. Topography was categorized into 13 anatomical sites: mediastinal, multicentric (involving at least 2 organs, excluding the regional lymph node), bone marrow, gastrointestinal, nodal, splenic, hepatic, heart, skin, ocular/orbital, central nervous system, oral cavity, and nasal. Each case was reviewed by 2 pathologists (VEV, ACD). The HE slides were first evaluated and an initial tentative diagnosis was given. The immunohistochemical stains (CD3 and CD20) were then reviewed and a final diagnosis was recorded. The mean mitoses were calculated by averaging the mitotic figures counted in three 40× high-power fields (field diameter of 0.09 cm) in regions deemed to have the best fixation and least amount of artifact. Mitoses per high-power field were assessed to relate to the grade of lymphoma (indolent grade = 0–1 mitoses, low grade = 2–5 mitoses, mid grade = 6–10 mitoses, and high grade = >10 mitoses).
Immunophenotyping
In total, 187 cases were labeled immunohistochemically for B- and T-cell antigens following a routine protocol. Briefly, for those cases immunostained at the University of Illinois, antigen retrieval was achieved by heating the mounted tissues to 125°C for 30 seconds followed by 90°C for 10 seconds in citrate buffer at pH 6.0 in a commercial pressure cooker, Decloaker (Biocare Medical, Walnut Creek, California). Endogenous peroxidase was blocked for 15 minutes with 3% hydrogen peroxide. Nonspecific immunoglobulin binding was blocked by incubation of slides for 10 minutes with a protein blocking agent (DAKO, Carpinteria, California) prior to application of the primary antibodies. The latter were allowed to react for 30 minutes at room temperature. Sections were stained in a Biogenex autostainer (BioGenex Laboratories, San Ramon, California). For those cases immunostained at the University of Pennsylvania, antigen retrieval was achieved by immersion in a citrate buffer, pH ~9.0, for 15 minutes in a 200-W microwave oven. Hydrogen peroxide was applied to tissue sections for 10 minutes to inactivate endogenous peroxidases. The immunostainer used was a DAKO automatic universal staining system. At both institutions, the slides were incubated with a rabbit monoclonal anti-CD20 antibody (RB=9013-P; Thermo Scientific, Rockford, Illinois) for B cells at a dilution of 1:100 and a rabbit polyclonal anti-CD3 antibody for T cells at a dilution of 1:100 (DAKO). CD20 antibody was selected over CD79a because superior staining quality of equine B cells was observed. At the University of Illinois, a supersensitive multilink kit was used for detection (BioGenex Laboratories), and a DAKO ENVISION+ kit (CD3) and DAKO LSAB2 kit (CD20) were used at the University of Pennsylvania. The immunoreactions were visualized with 3,39-diaminobenzidine substrate, and sections were counterstained with Mayer’s hematoxylin. Positive immunohistochemical controls included a normal equine lymph node to which the appropriate antisera were added. For negative controls, the primary antibodies were replaced with homologous nonimmune sera. In older cases in which the paraffin-embedded tissue blocks were unavailable, the cover slips were removed, heat-activated antigen retrieval was carried out, and the above staining protocol for the University of Illinois was performed.
Results
Signalment
The age of diagnosis was available for 183 horses. The mean age was 10.7 years (median, 10 years), with a range of 2 months to 31 years. There were 88 females and 97 males, 67 of which were geldings; the sex was unknown for 18 cases. Twenty-four breeds were represented. The most common breed was the Quarterhorse (n = 55; 27%), followed by Thoroughbreds (n = 33; 16%), Standardbreds (n = 30; 15%), and Arabs (n = 15; 7%). Other breeds included Morgan (n = 7; 3.5%); Appaloosa, Percheron, and Paint (n = 5 for each; 2.5%); Pony (n = 4; 2%); Warmblood, Welsh, and Trakehner (n = 3 for each; 1.5%); Palomino and mixed breed (n = 2 for each; 1%); and one each of Andalusian, Belgian, California Sport, Hanovarian, Mule, Mustang, and Shire. The breed was unknown for 24 horses.
Tumor Topography and Subtype
Thirteen anatomic locations were identified. The majority of the cases were multicentric (n = 83; 41%), followed by skin (n = 38; 19%) and gastrointestinal tract (n = 24; 11%). Other locations included mediastinal (n = 9; 4.5%), nodal (n = 9; 4.5%), ocular/orbital (n = 8; 4%), splenic (n = 5; 2.5%), nasal (n = 4; 2%), central nervous system (n = 4; 2%), oral cavity (n = 3; 1.5%), hepatic (n = 2; 1%), bone marrow (n = 1; 0.5%), and heart (n = 1; 0.5%). Tumor location was unknown in 12 cases. Sixty-two of the lymphoma cases were submitted as biopsy samples. Fifty percent of those cases (n = 31) were skin biopsies, and only 6 of the cases submitted 2 or more tissues and were categorized as multicentric. Using the WHO classification criteria, 14 subtypes of lymphoma were diagnosed (Table 1); a single case of atypical follicular hyperplasia originally diagnosed as lymphoma was also evaluated for comparison but not included in the overall evaluation of lymphomas. As such, 203 cases of lymphoma were included in the study and subtyped. The most common subtype was T-cell–rich large B-cell lymphoma (TCRLBCL) with 87 cases (43%) (Fig. 1a–c). Peripheral T-cell lymphoma (PTCL) was the second most common (n = 45; 22%) (Fig. 2a–c), followed by diffuse large B-cell lymphoma (DLBCL) (n = 26; 12.5%) (Fig. 3a–c). An additional 12 cases (6%) were diagnosed as diffuse large cell lymphomas (DCL); 4 of these were double negative for CD20 or CD3, and the remainder were not immunophenotyped and thus would likely have fallen into the PTCL or DLBCL categories. Eight cases (4%) were diagnosed with enteric-associated T-cell lymphoma (EATCL) (Fig. 4a–c).
Lymphoma Subtype and Mean Mitoses of Each Diagnosis (n = 203).
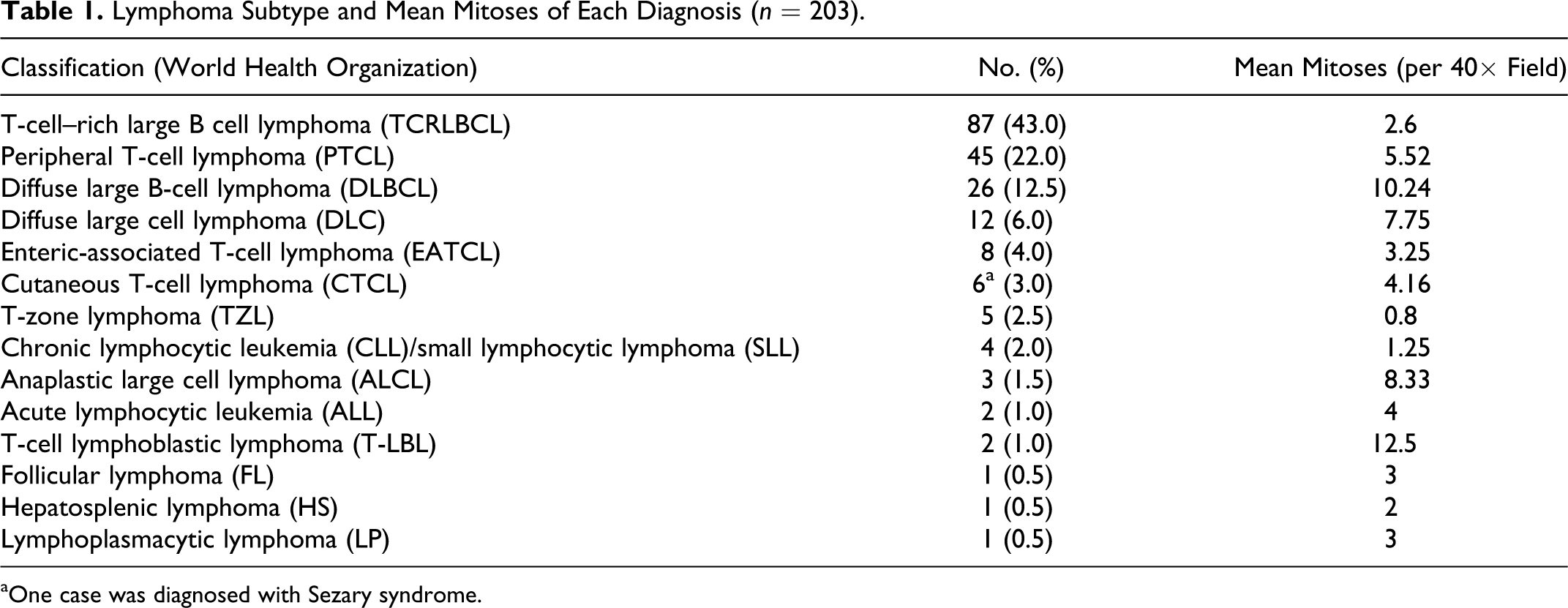
aOne case was diagnosed with Sezary syndrome.
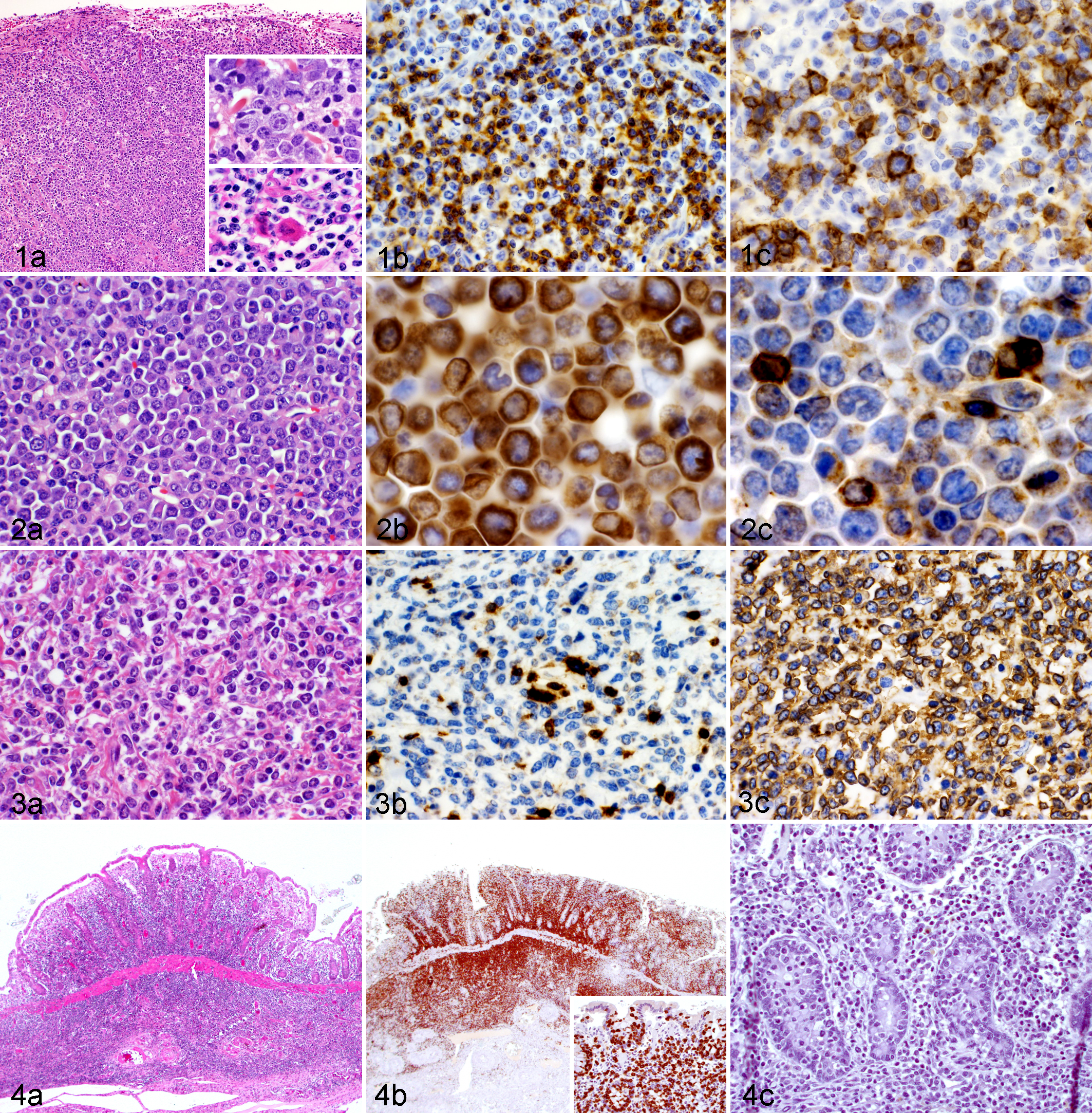
The diagnostic features of TCRLBCL include a majority of small, mature lymphocytes with nuclei approximately the size of a red blood cell. Among the small lymphocytes is a population of large cells with nuclei 2 to 3 times the diameter of a red blood cell; these cells are often binucleated and have prominent eosinophilic nucleoli. The large cells may be observed in mitosis or as single-cell necrosis with retracted cytoplasm and pyknotic nuclei. An additional characteristic feature of TCRLBCL is the presence of a dense fibrovascular network that keeps the tissue from fragmenting when sectioned, as opposed to the high-grade lymphomas such as PTCL and DLBCL, which are friable and tend to fissure when sectioned.46,47
The lymphoma subtypes were evaluated within the most common anatomic locations (Fig. 5a–c). The most common subtypes in the multicentric lymphomas followed the overall trend with TCRLBCL (n = 28; 34%), PTCL (n = 26; 31%), and DLBCL (n = 11; 13%) as the most common, respectively. Of the cutaneous lymphomas, the majority were TCRLBCL (n = 27; 71%) followed by cutaneous T-cell lymphoma (CTCL) (n = 6; 16%). Of note, 1 case of cutaneous T-cell lymphoma was diagnosed with Sezary syndrome based on the mucosal involvement and characteristic cells in the blood smear. TCRLBCL (n = 7; 30%), PTCL (n = 5; 21%), and EATCL (n = 6; 25%) (Figs. 2 to 4a–c) were the most common within the gastrointestinal tract.
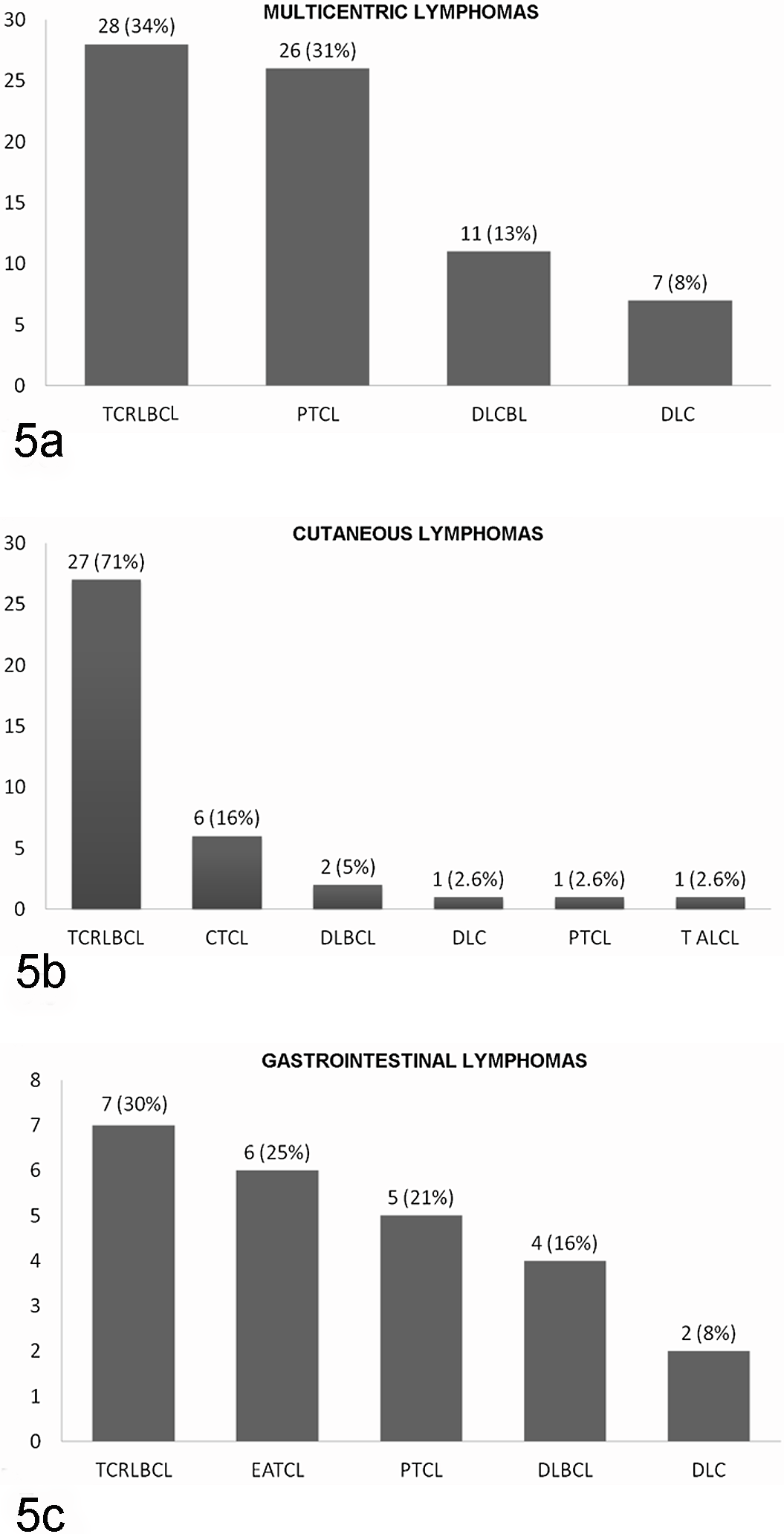
(a–c) Lymphoma subtypes based on the 3 most common anatomic locations: multicentric (a), cutaneous (b), and gastrointestinal (c). CTCL, cutaneous T-cell lymphoma; DLBCL, diffuse large B-cell lymphoma; DLC, diffuse large cell lymphoma; EATCL, enteric-associated T-cell lymphoma; PTCL, peripheral T-cell lymphoma; TALCL, T-Cell Anaplastic Large Cell Lymphoma; TCRLBCL, T-cell–rich large B cell lymphoma.
The subtypes and tumor topography were evaluated for each of the 3 most common breeds. Compatible with the overall trend, Quarterhorses had more multicentric lymphomas (n = 20; 24% of total), followed by cutaneous lymphomas (n = 13; 34% of total) and gastrointestinal lymphomas (n = 4; 16%). In contrast, Standardbreds had more gastrointestinal lymphomas (n = 8; 33% of total) than any other breed and only 1 case of cutaneous lymphoma. There were 18 cases (22% of total) of multicentric lymphoma in Standardbreds. Thoroughbreds had only 1 case of gastrointestinal lymphoma, 8 cases of cutaneous lymphoma, and all 3 cases of lymphoma in the oral cavity. There were 17 cases (21% of total) of multicentric lymphoma in Thoroughbreds. Both Quarterhorses and Thoroughbreds followed the overall trend of lymphoma subtypes, whereas Standardbreds had more cases of EATCL than DLBCL, with only 1 case of the latter.
Mitoses
The average mitoses per single high-power field are listed on Table 1. Of the most common lymphoma subtypes, TCRLBCL had the lowest mitoses (2.6). Lymphoblastic lymphoma had the highest number (12.5), followed by DLBCL (10.24). The single case of atypical follicular hyperplasia had 15 mitoses.
Clinical Data
Limited clinical data consisting mainly of information derived from the pathology request form were available for 109 cases. Weight loss, anorexia, and depression were described in 32 cases (30%); ventral edema, with or without reported hypoproteinemia, in 20 cases (18%); pyrexia and anemia in 19 cases each (17%); diarrhea in 8 cases (7%); and colic in 7 cases (6%). The reports of diarrhea and colic were not restricted to the cases of gastrointestinal lymphoma.
Discussion
Our study found that TCRLBCL is the most common lymphoma subtype in the horse. This subtype was first reported in the horse by Kelley and Mahaffey in 1998, 17 who describe 11 of their 31 cases as TCRLBCL. One of the most common clinical presentations of this neoplasm is multiple subcutaneous nodules; some have described a waxing and waning nature of these tumors, and one proposed cause is fluctuations in serum hormone concentration, particularly progesterone, associated with the estrous cycle.14,15
In humans, TCRLBCL is not defined as a separate entity in the REAL-WHO classification but rather as one of the variants of large B-cell lymphoma and is referred to as T-cell/histiocytic-rich large B-cell lymphoma (T/HRLBL). It is thought that the T-cell infiltrate may be related to interleukin-4 production by the lymphoma cells and histiocytes. 3 It is also one of the so-called “gray zone lymphomas” because of its overlapping features with nodular lymphocyte predominant Hodgkin lymphoma (NLPHL). 55 Hodgkin lymphoma (HL) has been divided in the WHO classification into 2 major groups based on molecular pathology: classic HL and NLPHL. Classic HL has 4 subtypes but is characterized by Reed-Sternberg cells that are CD15 and CD30 positive and CD20 negative. NLPHL has the opposite pattern of expression and invariably expresses the B-cell marker CD20.
The morphology of the neoplastic cells seen in classic HL includes mononuclear Hodgkin cells and the aforementioned Reed-Sternberg cells (RS cells), which are binucleated or bilobed and have large prominent nucleoli. Some cells are known as “mummified cells” and have condensed cytoplasm and pyknotic nuclei. In one of the subtypes of classic HL (nodular sclerosis HL), there are RS variant “lacunar cells” that have a cytoplasm that retracts from the membrane, so the cells appear to sit in lacunae in formalin-fixed tissue. In NLPHL, the RS cells show a different morphology and have folded or multilobated nuclei and scant cytoplasm and thus are called popcorn or lymphocytic and/or histiocytic (L&H) cells.
It is currently believed that progressively transformed germinal centers (PTGC), NLPHL, and T/HRLBL are related and represent different stages of a progressive disease. PTGC is a benign reactive disease process characterized by local, usually asymptomatic, lymphadenopathy. Histologically, there is follicular hyperplasia with large germinal centers that are poorly demarcated from the surrounding expanded mantle zone. In contrast, NLPHL is a mature B-cell lymphoma with an indolent clinical course, and T/HRLBL has an aggressive clinical course and is treated as DLBCL. Because of the different biological behavior and treatment protocols, distinguishing NLPHL from T/HRLBL is critical.
In humans, several arbitrary clinical and histologic features have been proposed to differentiate the 2 entities: NLPHL is limited to lymph nodes, whereas T/HRLBL often involves the extranodal sites; NLPHL tends to be nodular and T/HRLBL diffuse; the neoplastic cells in NLPHL are “popcorn” L&H cells, whereas T/HRLBL has centroblastic, immunoblastic, or RS-like cells; and the background population of small lymphocytes are a mixture of B and T cells in NLPHL, but small reactive B cells are rare in T/HRLBL. In veterinary species, TCRLBCL is seen in many domestic animals but is most commonly reported in the horse and cat47,54 and rarely in dogs. 48 Biologically, it appears that this entity has a slow clinical course in cats and dogs, but further study is necessary to determine if TCRLBCL is an indolent lymphoma in horses.
Several indolent lymphomas have been fairly well characterized in dogs and are thought to arise from chronically hyperplastic nodes. The indolent lymphomas are in part defined as having 0 to 1 mitoses per high-power field. The most common indolent lymphomas in dogs include the B-cell neoplasms follicular lymphoma (FL), mantle cell lymphoma (MCL), and marginal zone lymphoma (MZL); the T-cell type is T-zone lymphoma (TZL). These subtypes tend to maintain a nodular pattern within the node or spleen and have few mitoses (0–1 per high-power field) and a slow clinical progression. 51 We did not recognize MCL or MZL in our study population. We did have 5 cases of TZL, and the mean mitoses was very low (0.8), suggesting an indolent neoplasm. To our knowledge, this is the first description of TZL in horses. In dogs, TZL comprises about 10% to 12% of lymphomas 50 and is clinically associated with long survival times with minimal to no treatment. In humans, TZL does not exist as a distinct entity and is instead described as the T-zone variant of peripheral T-cell lymphoma, unspecified.
In contrast, FL in humans is a well-described entity, comprising 22% of the non-Hodgkin lymphomas worldwide. It is considered one of the most common low-grade lymphomas; patients are usually asymptomatic except for lymph node enlargement. FL is currently subdivided into 3 grades based on the number of centroblasts per high-power field, with more numerous centroblasts associated with a higher grade. Although a common subtype in human lymphoma, FL is a rare diagnosis in domestic animals but appears to follow an indolent course as seen in people and is often found incidentally in otherwise healthy animals.47,49 We report 1 case of FL in the liver, which is the first known report of this disease in horses. Unfortunately, we had no clinical data on this patient, but histologically it was noted as FL grade 2 and had an average of 3 mitoses, compatible with a low-grade lymphoma.
One obvious limitation of this study is its retrospective and descriptive nature and lack of clinical data and follow-up. In addition, most biopsy samples consisted of only the one tissue of interest, potentially falsely decreasing the total number of multicentric lymphomas. Our goal of this project was to provide information about the most commonly seen lymphoma subtypes in horses as categorized by the WHO classification system, identify the range of anatomic distributions, and report trends of signalment data. From the human and canine studies, it is apparent that lymphoma is a diverse disease, and patients need to be treated according to their individual disease subtype and clinical presentation. Future studies focusing on specific subtypes or locations, as well as their clinical outcome, are necessary to help identify prognostic features and appropriate therapies in horses.
Footnotes
Acknowledgements
We are grateful to all of the universities that submitted case material for this study and are especially thankful for the many cases shared by Dr. Weisbrode from the Ohio State University. We thank Jackie Ferracone at the University of Pennsylvania and Jane Chladny at the University of Illinois for their excellent work with the immunohistochemical preparations. We also thank Fiona Scott for her input and organization of our data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.