
Abstract
This multi-institutional report describes 8 cases of rhabdomyosarcoma in horses. Four neoplasms were in the tongue and other areas of the mouth or head, 2 were in the abdominal wall, and 1 each was in right shoulder muscles and heart. Four rhabdomyosarcomas that were less than 10 cm in diameter were treated by surgical excision or radiation with no recurrence. Two neoplasms greater than 10 cm in diameter in the abdominal wall and the right shoulder were considered inoperable and led to decisions to euthanize the horses. Two neoplasms were incidental findings at necropsy. All the neoplasms were classified as embryonal except for 1 pleomorphic rhabdomyosarcoma. These 8 cases were evaluated with 9 published case reports of equine rhabdomyosarcoma. For all cases, the most common sites were limb muscles (5/17) and tongue (4/17). Metastasis was reported in 4 of the previously published cases; none was found in this study.
Rhabdomyosarcoma is rare in horses.4,14 Standard veterinary references define it as a malignant neoplasm that differentiates to form striated muscle. More broadly, it is a neoplasm derived from primitive mesenchyme with characteristics of myogenesis (ie, rhabdopoietic sarcoma). 9 In veterinary pathology, rhabdomyosarcoma is classified as embryonal (including botryoid), alveolar, or pleomorphic.4,14 This classification system is based on histomorphology and derived from systems developed in human pathology from which more elaborate schema have evolved.9,10,12 There is well-defined correlation of the pathologic classification of human rhabdomyosarcomas with prognosis and molecular markers including genetic markers associated with translocation.9,10,12 For equine rhabdomyosarcoma, data on age, breed, site, presenting signs, frequency of metastasis, and treatment outcome are limited to information from individual case reports.1–3,5–8,11,13 Criteria for grading equine rhabdomyosarcomas have not been developed, 4 so prognostication is difficult beyond general comments that they are invasive with metastatic potential.4,14 We describe clinical and pathologic features of 8 rhabdomyosarcomas in horses submitted to 5 university diagnostic centers and contrast our findings with those of 9 previously published cases of equine rhabdomyosarcoma.1–3,5–8,11,13
Methods
After accession of an equine rhabdomyosarcoma (Case 1) in 2009, a search of the database for surgical pathology at the University of Florida from 1992 through 2009 (8,929 equine accessions) and necropsy pathology from 1995 through 2009 (4,368 equine accessions) identified 2 additional cases of equine rhabdomyosarcoma from Florida veterinary practices. An additional 5 cases were identified through database searches and case review by pathologists at the University of Kentucky Livestock Disease Diagnostic Laboratory, University of Pennsylvania School of Veterinary Medicine, University of California School of Veterinary Medicine, and Texas A&M University College of Veterinary Medicine. Findings were summarized and compared with those from previously published cases.1–3,5–8,11,13
The diagnosis of embryonal rhabdomyosarcoma was based on the presence of round and spindle cells resembling myoblasts and primitive myotubes. Cells had strap cell or racquet cell appearance; some had cytoplasmic striations visible in hematoxylin and eosin (HE) and/or phosphotungstic acid hematoxylin (PTAH)-stained sections, or sarcomeric ultrastructural features, including Z-bands and/or thick and thin (actin and myosin) filaments.4,14 Immunohistochemical features of striated muscle differentiation included expression of muscle-associated proteins such as desmin, myosin, and/or sarcomeric actin. 4 Criteria of alveolar rhabdomyosarcoma were round cells in an alveolar pattern with alveolar spaces defined externally by fibrous bands and internally by a row of neoplastic cells attached to the fibrous septa.4,12 Pleomorphic rhabdomyosarcoma was composed of highly pleomorphic cells with prominent nucleoli and multinucleated tumor cells in dense collagenous stroma.4,9,10,14 Histochemical, immunohistochemical, and transmission electron microscopic procedures are provided in a supplementary file (a supplemental appendix to this article is published electronically only at http://vet.sagepub.com/supplemental).
Results
Signalment, clinical features, and outcome of the 8 horses are summarized in Table 1 . Each neoplasm was classified as embryonal rhabdomyosarcoma, except in Case 6, which was a pleomorphic rhabdomyosarcoma.
Signalment, Clinical Features and Outcome in 8 Horses with Rhabdomyosarcoma
Abbreviations: TAMU, Texas A&M University; UCD, University of California–Davis; UF, University of Florida; UK, University of Kentucky; Penn, University of Pennsylvania.
Case 1
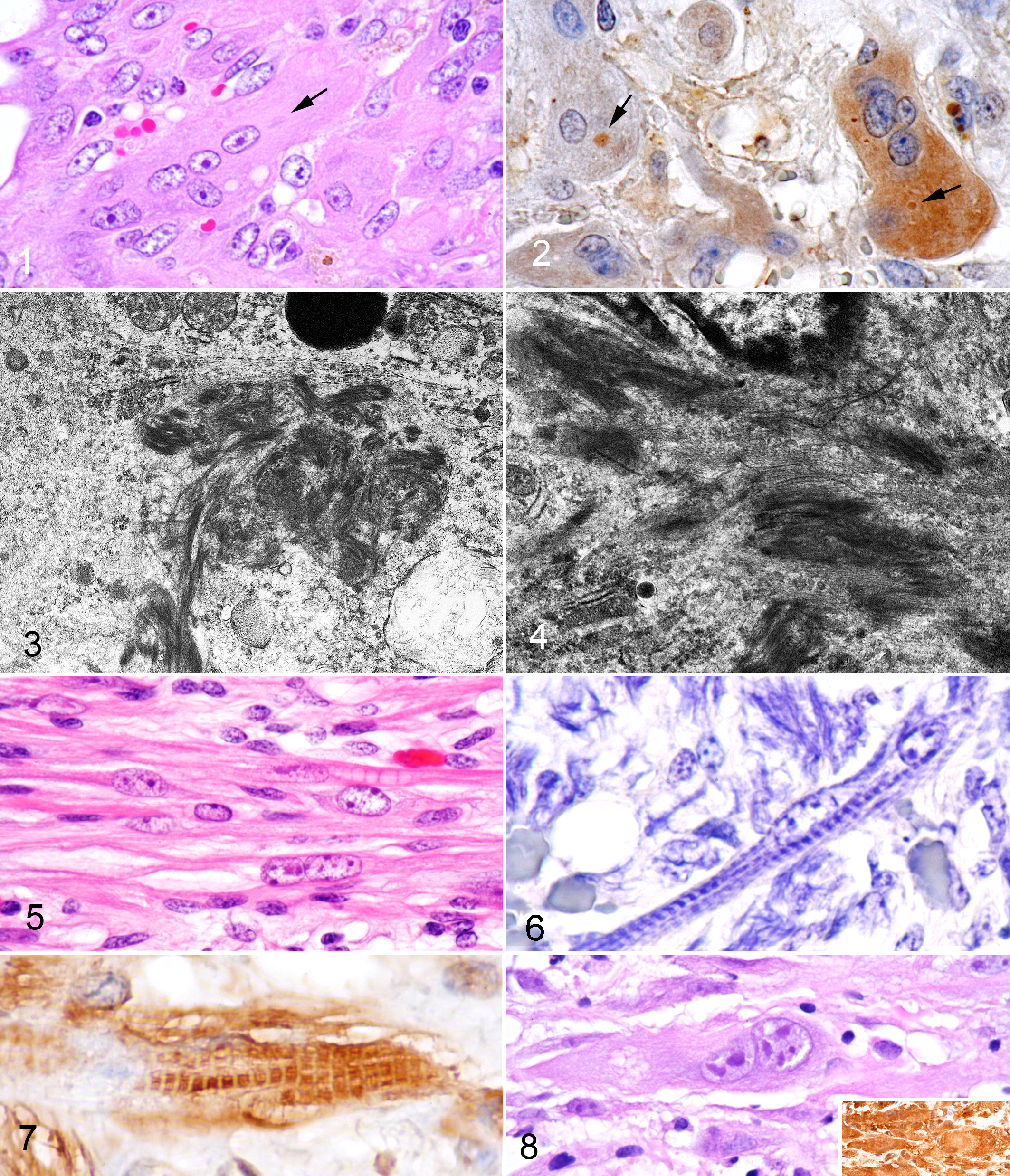
The ventral abdominal subcutaneous mass, visible from the skin surface, appeared to be surrounded by a fibrous capsule that separated easily from surrounding tissues. The fixed specimen contained a dark tan, firm, flattened spherical mass. Histologically, a well-circumscribed, densely cellular mass was surrounded by collagen-rich connective tissue that formed an almost complete capsule, breached multifocally by neoplastic cells that were still bordered by 2-3 mm of more loosely arranged connective tissue. The densely cellular areas were composed of aggregates of large round to spindle to elongate tubular cells arranged in confluent sheets with occasional whorled arrays. Many elongate tubular multinucleated cells contained up to 7 ovoid nuclei that were often arranged in tandem array resembling embryonic muscle (Fig. 1). Anisocytosis and anisokaryosis were moderate; the mitotic index (number of mitotic figures per 10 high-power [400×] fields) was 4. The fibrovascular stroma had scattered aggregates of lymphocytes, macrophages, and plasma cells with multifocal hemorrhage. No striations were identified in HE or PTAH-stained sections. However, globular eosinophilic cytoplasmic inclusions were identified in some multinucleated cells (Fig. 1). Tumor cells had strongly positive diffuse cytoplasmic reactivity for vimentin, weakly positive diffuse cytoplasmic reactivity for desmin, and were uniformly negative for smooth muscle actin. Cells had variably positive cytoplasmic reactivity for sarcomeric actin; multinucleated cells had the strongest reactivity (Fig. 2). Globular cytoplasmic inclusions were strongly reactive for sarcomeric actin (Fig. 2). The cytoplasmic structures in transmission electron micrographs that best corresponded to the globular inclusions in histologic sections were dense aggregates of thick (13–15 nm in diameter) and thin (8–10 nm in diameter) electron-dense filaments with scattered denser aggregates of filaments forming electron-dense mats (Figs. 3 and 4 ). Although the ultrastructure and sarcomeric actin immunoreactivity were consistent with differentiation toward striated muscle cells, no well-formed sarcomeres with Z-band material oriented perpendicular to thin and thick filaments were identified. The cells contained abundant rough and smooth endoplasmic reticulum and many mitochondria.
Case 2
A bright red, soft, multilobulated nodule in the musculature 4 cm caudal to the tip of the tongue was an incidental finding during an insurance necropsy. The mass did not extend into the mucosa but was unencapsulated and infiltrative. The neoplastic cells varied from spindled to larger multinucleated strap cells with cytoplasmic striations (Fig. 5) and tandem nuclear arrangement. Cells had moderate anisokaryosis. No mitotic figures were found. Strap cells had prominent Z-band striations that were visible in HE-stained sections and accentuated with PTAH (Fig. 6). The cytoplasm was strongly positive for vimentin and sarcomeric actin (Fig. 7). Many spindle cells had vacuolated cytoplasm (spider web cells). Well-differentiated fibroblasts, collagen fibers, and capillaries, as well as few lymphocytes, were interspersed among neoplastic cells.
Case 3
This abdominal wall mass was discovered by ultrasound in a horse with colic and abdominal distension, and diagnosed from percutaneous needle biopsy samples. The horse was euthanized without treatment for the tumor; necropsy was not permitted. The biopsy samples contained scanty normal skeletal muscle with areas of necrotic skeletal muscle surrounded by neutrophils and macrophages with interspersed dense populations of spindle cells and elongated multinucleated cells with large, hyperchromatic nuclei (Fig. 8). Anisocytosis and anisokaryosis were marked; the mitotic index was 4.5. Multipolar mitotic figures with 3 centrioles were found. No striations were identified in HE or PTAH-stained sections. The neoplastic cells were strongly positive for vimentin and sarcomeric actin (Fig. 8).
Case 4
The tumor involved muscle in the right ventral aspect of the tip of the tongue. Mechanical trauma during mastication had resulted in hemorrhage. The tongue was partially amputated as treatment, and fixed tissue was submitted for diagnosis. Histologically, the mass was composed predominantly of elongate spindle cells with elongate ovoid nuclei and tubular cytoplasm, as well as round cells with round nuclei and moderate amounts of cytoplasm. Anisocytosis and anisokaryosis were marked. The mitotic index was 3. Multinucleated cells with tandem nuclear arrangements were lightly scattered through the neoplasm. Neoplastic cells infiltrated irregularly into surrounding tissue and impinged multifocally on blood and lymphatic vessels; however, neoplastic tissue remained covered by endothelial cells, and free tumor emboli were not found. No striations were identified in HE- or PTAH-stained sections. The tumor cells were weakly positive for desmin and uniformly positive for sarcomeric actin.
Case 5
A tumor in the right pectoral muscle had increased in size over 3 months. A surgical biopsy specimen was obtained for diagnosis, but, because of the proximity of the neoplasm to the jugular vein and carotid artery, complete excision was not attempted, and the horse was euthanized. At necropsy, the well-demarcated, smooth-surfaced mass was tan with linear streaks and few scattered cysts up to 3 cm in diameter that contained gelatinous yellow-tan material. The lateral aspect of the mass was less defined where it transitioned to non-neoplastic skeletal muscle. Histologically, neoplastic spindle cells, often resembling myotubules, were arranged in interlacing bundles in a myxoid, vascularized stroma. Neoplastic cells had variably distinct cell borders and contained moderate to abundant eosinophilic fibrillar cytoplasm, rarely with cross-striations, and an oval to elongated nucleus with finely stippled chromatin and occasional small nucleoli. Multinucleate cells formed occasional strap cells. The mitotic index was 1. Few lymphocytes and macrophages were scattered throughout the stroma. The neoplastic cells were immunoreactive for vimentin, desmin, muscular actin, myoglobin, and calponin.
Case 6
This slowly expanding mass in the left masseter muscle was composed of pleomorphic round, spindle, and polygonal cells with numerous multinucleated cells. Strap cells, but no cross-striations, were present. Anisocytosis and anisokaryosis were marked. No mitotic figures were found. There was focal necrosis with lymphocytic infiltration. The mass was partially encapsulated with multifocal capsular invasion. The adjacent skeletal muscle was multifocally atrophied and fibrotic, but without evidence of neoplastic infiltration. Neoplastic cells were weakly immunoreactive for vimentin, actin, and myoglobin, and negative for desmin.
Case 7
Incisional biopsy was repeated on this oral mass, which had been diagnosed as rhabdomyosarcoma by an outside pathology service. The tumor was composed of haphazardly arranged bundles of neoplastic cells that infiltrated skeletal muscle. A capsule was not identified. Neoplastic cells were predominantly round to polygonal with rare spindloid cells, multinucleated myotubular cells, and strap cells with striations visible in PTAH-stained sections. Mitotic figures were not found. Neoplastic cells were positive for desmin and sarcomeric actin by immunohistochemistry.
Case 8
This neonatal foal with urachal infection and peritonitis was euthanized because of deteriorating clinical condition. At necropsy, diffuse and irregular pallor was noted in much of the left ventricular myocardium. Histologically, affected myocardium was diffusely infiltrated by neoplastic spindle cells with multifocal mineralization. Tandem nuclei were noted in some cells. No strap cells or myotubes were observed. Cross-striations were not seen in PTAH- or HE-stained sections. The mitotic index was 10. Neoplastic cells were immunohistochemically positive for actin and vimentin, weakly positive for myoglobin, and negative for desmin.
Discussion
Rhabdomyosarcoma is a rare neoplasm in horses with little information in texts or review articles on clinical presentation, pathologic manifestations, or biological behavior.4,14 The signalment, clinical features, and outcome in 9 published cases1–3,5–8,11,13 of equine rhabdomyosarcoma are summarized in supplementary Table 2 (a supplemental appendix to this article is published electronically only at http://vet.sagepub.com/supplemental). Age at presentation in our 8 cases varied from newborn to 21 years (median and mean, 5 and 8 years, respectively). Previously published cases had comparable age ranges with median and mean ages of 3.5 and 5.6 years, respectively. Median and mean ages at presentation for all 16 horses with reported age were 5 and 6.4 years, respectively. No sex or breed predisposition was apparent. All 8 neoplasms in this study were classified as embryonal rhabdomyosarcomas, except for 1 pleomorphic rhabdomyosarcoma. Previously published cases included 4 embryonal, 2 pleomorphic, 2 alveolar,3,6 and 1 unclassified rhabdomyosarcoma.
The most common sites of rhabdomyosarcoma in this study were the tongue or other oral tissues and the head (4/8) and abdominal wall (2/8). The site distribution for all neoplasms from this and previously published cases was: limb muscle (5/17); tongue (4/17); abdominal wall (2/17); and 1 each in the buccal wall, masseter area, heart, thoracic wall, uterus, and urinary bladder. The neoplasms in the uterus and the urinary bladder were botryoid rhabdomyosarcomas.11,13
Metastasis was not found in any of the 8 cases in this report but was documented in 4 of the previously published 9 cases: 2 from alveolar rhabdomyosarcomas in the hind limbs,3,6 1 each from an embryonal rhabdomyosarcoma in the bladder, 13 and a pleomorphic rhabdomyosarcoma in the abdominal wall. 7 No obvious features in those cases, other than alveolar subtype, were strongly associated with metastasis.
In this study, clinical presentation was as a slow-growing, externally visible mass (4/8), ulcerated oral mass (1/8), ascites and edema with colic (1/8), or incidental finding at necropsy (2/8). Four neoplasms were <10 cm in diameter and were treated successfully by surgery or radiation. In 2 cases, masses >10 cm diameter in the right shoulder area and in the abdominal wall were considered poor surgical risks or inoperable and resulted in decisions to euthanize the horses.
Surgical treatment was attempted in 4 of the previously reported 9 cases, but long-term remission was achieved in only 1 horse with a lingual mass. 8 The other 3 horses either had large masses (≥ 10 cm diameter) that were incompletely resected or experienced surgical complications that led to death or the decision to euthanize.1,11,13 In 6 of the 9 horses, death or the decision to euthanize was attributed to the rhabdomyosarcoma.1,3,6,7,11,13 Of the 4 horses in this study that were treated with surgery or radiation, the rhabdomyosarcoma did not recur during the 7-month to 4-year follow-up period. It is reasonable to attribute this therapeutic success at least partially to early identification and treatment of the neoplasm before it exceeded 10 cm in diameter. It is also possible that the difference in outcome reflects differences in the rhabdomyosarcomas in our study and those of previous reports. In previous reports, 7 of 8 rhabdomyosarcomas were diagnosed based on histomorphology with identification of striations or ultrastructural evidence of actin- and myosin-like filaments (in some cases, with Z-band structures). Immunohistochemistry was used in only 3 cases.1,8,13 One published case presented no criteria for diagnosis. 2 In our study, histomorphology was coupled with identification of striations or ultrastructural myofilaments in 5 of 8 cases. Immunohistochemistry was critical to diagnosis in the absence of striations or myofilament-like structures in 3 cases. Two of the surgically treated tumors without recurrence were neoplasms for which the diagnosis was based on histomorphology and immunohistochemistry alone without identification of striations. It is possible that immunohistochemistry detects neoplastic cells with early muscle gene activation in addition to neoplastic cells that express actin and myosin filaments and striations demonstrable by ultrastructure and light microscopy. 10 These potentially less-advanced stages of rhabdomyosarcoma may be more responsive to treatment than better-differentiated rhabdomyosarcomas with microscopically detectable sarcomeric filaments and striations.
Mitotic index and cellular pleomorphism are 2 other features used to grade rhabdomyosarcomas and other soft tissue sarcomas. 4 The mitotic index was 0 to 1 in 4 of the 8 tumors in this study. The mitotic index was 4.5 in Case 3, which had an inoperable neoplasm in the abdominal wall, and 10 in Case 8, in which the neoplasm infiltrated throughout the left ventricular myocardium. In the previous reports, frequent mitotic figures were associated generally with infiltrative and metastatic behavior, but numeric data were rarely provided.3,5–7,11 Pleomorphism of neoplastic cells, including anisocytosis and anisokaryosis, was found in neoplasms that responded well to surgical treatment in this study (eg, Case 1 and Case 6) and in a previous report, 8 and apparently it was not a reliable single criterion of malignant behavior.
In conclusion, analysis of our 8 cases and 9 other reported cases indicates that equine rhabdomyosarcomas occur with low prevalence in horses from birth to advanced age. They have been found most frequently in the limbs, the tongue, and other structures of the head. Small neoplasms (< 10 cm diameter) that were treated by surgery or radiotherapy did not recur or metastasize. Neoplasms larger than 10 cm in diameter were most frequently associated with infiltrative behavior or growth that made surgical excision difficult. Four metastatic rhabdomyosarcomas were either ≥ 10 cm diameter or were classified as alveolar rhabdomyosarcomas. Cellular pleomorphism did not appear to be a useful indicator of biologic behavior or response to surgical treatment. High mitotic index may be associated with infiltrative and metastatic behavior. However, this and other neoplastic features must be critically evaluated as additional cases of equine rhabdomyosarcoma become available for study and treatment.
Footnotes
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.