
Abstract
Ménétrier disease is a rare hypertrophic gastropathy that is characterized by hyperplasia of the mucous cells with concurrent loss of chief and parietal cells within the gastric glands. There are few reports of this disease in dogs, and little is known about the clinical presentation and progression of canine Ménétrier disease. Three Cairn terrier littermates developed hypertrophic gastropathy with histological features of Ménétrier disease. One dog remained clinically asymptomatic for 2 years after diagnosis. The development of this disease in 3 siblings suggests a possible inherited predisposition. All 3 dogs also developed gastric neoplasia, which has been reported in human Ménétrier disease but has not been associated previously with hypertrophic gastropathy in domestic species.
In hypertrophic gastropathy, thickening of the gastric wall is due to epithelial hyperplasia, which imparts a diffuse or localized cerebriform appearance to the mucosal surface. 5 The hypertrophic gastropathies can be subclassified according to the hyperplastic cell type. 2 In Ménétrier disease, the gastric mural thickening is due to hyperplasia of the mucous cells with concurrent loss of chief and parietal cells. 1,11 Human Ménétrier disease is usually idiopathic, develops in older adults, and predisposes to gastric cancer. 8,11
In dogs, there are few reports of Ménétrier disease. 7,12 This report describes 3 Cairn terrier littermates with hypertrophic gastropathy that was histologically consistent with Ménétrier disease. All 3 dogs also developed gastric adenocarcinoma. Because the dogs were siblings, this suggests a possible inherited predisposition to Ménétrier disease.
Case Reports
Case No. 1
A 10-year-old intact female Cairn terrier dog developed intermittent vomiting. The dog was lethargic; no weight loss had been observed, and physical examination findings were otherwise unremarkable. Changes to the diet, which was formulated by the owner, initially reduced the frequency of vomiting; however, 4 months after presentation, the vomiting increased in frequency and was accompanied by hematemesis, abdominal pain, and anorexia. Serum albumin concentration (31 g/L; reference, 25–44), serum globulin concentration (38 g/L; reference, 17–39), packed cell volume (PCV), and serum biochemistry were within reference ranges. At exploratory laparotomy, 6 months after onset of clinical signs, the gastric wall was diffusely thickened with a poorly defined 2-cm-diameter firm mass in the body of the stomach in the lesser curvature. The thickened gastric wall immediately adjacent to the mass was biopsied and submitted for histological examination.
In histologic section, the gastric mucosa was 6 mm thick; the entire gastric wall was 12 mm thick. Gastric glands were elongated (Fig. 1), especially in the neck and base, with the gastric pits unaffected. The elongated gastric glands had fewer parietal and chief cells and increased numbers of mucous cells. The loss of parietal and chief cells was most marked in the deeper aspects of the gastric glands. The base of gastric glands had dilatation from mild to cystic proportions up to 3 mm in diameter. Most cystic glands were lined entirely by mucous cells that resembled the gastric mucous neck cells and, like the neck cells, produced abundant periodic acid-Schiff-positive material (Fig. 2). The elongated gastric glands were supported by increased quantities of pale loose stroma with moderate numbers of lymphocytes and plasma cells, including Mott cells, that were mostly scattered diffusely through the lamina propria. Neither neutrophils nor necrosis were noted. Microorganisms were not detected by Warthin-Starry histochemistry.
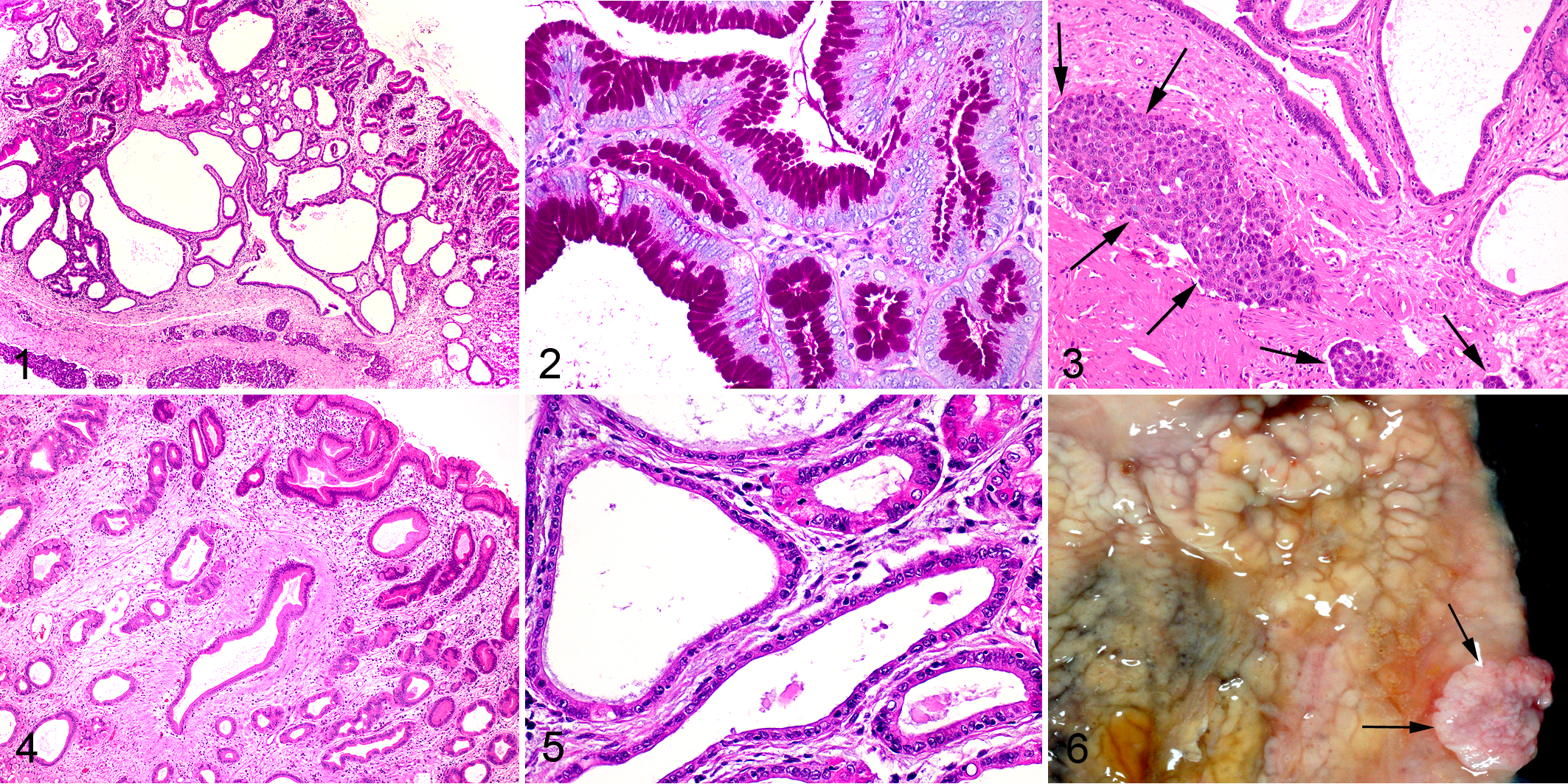
Submucosal lymphatic vessels contained rafts of neoplastic epithelial cells (Fig. 3). The polygonal to pleomorphic cells had ample vacuolated eosinophilic cytoplasm, a large round central nucleus, prominent or multiple nucleoli, and 5 mitotic figures per high power field (hpf). The histological diagnoses were hypertrophic gastropathy and gastric adenocarcinoma. Because of the increased numbers of mucous cells and decreased numbers of parietal and chief cells in the elongated gastric glands, the hypertrophic gastropathy was classified as Ménétrier disease. The dog was euthanatized; postmortem examination was not performed.
Case No. 2
Two months after dog No. 1 developed disease, a male sibling developed vomiting and weight loss over a 10-day period. The dog was in poor body condition and appeared lethargic. This dog was from a different household than dog No. 1 and mainly ate commercial dog food. Marked cystic thickening of the gastric wall was detected by ultrasound. Serum total protein and PCV were within normal limits. Although the dog was treated with a gastric protectant and dietary modification, weight loss and occasional vomiting continued over the next 3 weeks. At exploratory laparotomy, there was marked diffuse thickening of the gastric wall and enlargement of the gastric lymph nodes. Samples of stomach and gastric lymph node were submitted for histological examination.
Histologically, gastric glands were elongated with replacement of chief and parietal cells by mucous cells and cystic dilatation of the base of the glands (Fig. 4). The glands were separated by pale stroma with scattered lymphocytes and plasma cells. Neoplastic epithelial cells were not found in gastric submucosal lymphatic vessels but were present in the gastric lymph nodes. Ménétrier disease and lymphatic metastasis of a gastric adenocarcinoma were diagnosed. The dog was euthanatized; postmortem examination was not performed.
Case No. 3
Ten months after dog No. 1 developed disease, a female littermate developed lethargy, without history of vomiting. Serum albumin concentration (43 g/L), serum globulin concentration (29 g/L), and PCV were within reference ranges. The dog was from the same household as case No. 1, so gastric disease was suspected. Cystic thickening of the gastric mucosa was found by ultrasound. The gastric wall was biopsied for histological examination.
As in case Nos. 1 and 2, elongation and cystic dilatation of the gastric glands was the salient histologic feature; the cystic gastric glands were lined predominantly by mucous cells (Fig. 5). Compared with the other 2 dogs, mucosal stroma was less abundant and infiltrated by fewer lymphoid cells. The diagnosis was Ménétrier disease. No evidence of neoplasia was observed. Although the cause for lethargy was not determined, the dog made a complete clinical recovery without treatment.
Because its littermates with Ménétrier disease had developed gastric adenocarcinoma by the time of diagnosis, the gastric lesions in dog No. 3 were considered potentially pre-neoplastic. To try to prevent neoplasia, the dog was treated with a gastric protectant, a proton pump inhibitor to reduce gastric acidity, and a nonsteroidal anti-inflammatory drug. The dog had no clinical evidence of gastrointestinal disease for the following 2 years. However, ultrasound examinations at 6-month intervals showed slowly progressive thickening of the gastric wall. Two years after the diagnosis of Ménétrier disease, a focal loss of normal layering of the stomach wall was detected using ultrasound. Over the next 3 months, increasingly frequent vomiting was observed. The dog became anorexic and was euthanatized.
At necropsy, the gastric wall was markedly thickened with a cerebriform appearance of the mucosa (Fig. 6), particularly in the body of the stomach where the wall was up to 15 mm thick. The wall of the gastric fundus and cardia was also thickened, albeit to a lesser degree. Mild thickening was detected in the antrum, whereas the pylorus was grossly normal. An exophytic 2-cm-diameter mucosal mass was in the body of the stomach.
Histologically, the body, cardia, fundus, and antrum all had elongation and cystic dilatation of the gastric glands. The dilated glands were lined by mucous cells. The cystic change was most extensive in the body of the stomach, where loss of chief and parietal cells was conspicuous. The gastric mass was a poorly differentiated gastric adenocarcinoma that appeared as a polypoid proliferation of tightly packed neoplastic cells arranged in poorly formed glands. The neoplastic cells were mildly pleomorphic with 4 mitotic figures/hpf. Neoplastic cells were in lymphatic and small blood vessels in sections from all gastric specimens.
The 3 affected dogs were from a litter of 6; the other 3 littermates could not be located. The sire of this litter died after a period of intractable vomiting and weight loss, without diagnostic testing. No gastric abnormalities were detected by ultrasound of a 10-year-old daughter of dog No. 1.
Discussion
In all 3 Cairn terriers, the prominent gastric mucous cell hyperplasia with loss of chief and parietal cells is consistent with descriptions of human Ménétrier disease. 2,5 Ménétrier disease is typically a disease of older people with an average age at diagnosis of 55 years. 1,5 Similarly, all 3 Cairn terriers of this report were old dogs (10 or 11 years old) at diagnosis. In humans, Ménétrier disease often initially presents with mild nonspecific clinical signs that include abdominal pain, nausea, and vomiting. 8 In many patients, clinical signs are present for years or decades prior to diagnosis. 8 In the 3 Cairn terriers with Ménétrier disease, 2 had vomiting and 1 had weight loss. However, as a gastric adenocarcinoma was also present in all 3 dogs, it is uncertain whether the clinical signs were due to Ménétrier disease or to gastric neoplasia. The third dog had Ménétrier disease for 2 years without clinical signs of the disease and only developed clinical signs of gastrointestinal disease around the time that gastric neoplasia was diagnosed. The Ménétrier disease in this dog might have remained undetected during the preclinical stage if 2 littermates had not developed the disease.
Ménétrier disease was reported in an 11-year-old Old English Sheepdog with a 1-month history of weight loss, anorexia, and vomiting, and death 4.5 months later. 7 Ménétrier disease resulted in weight loss, anorexia, and vomiting in a 7-year-old Boxer that died 5 months after the onset of clinical signs. 12 The disease has also been reported in Drentse Patrijshonds as a component of the familial stomatocytosis-hypertrophic gastritis syndrome. 10
People with Ménétrier disease can develop hypoproteinemia and anemia due to protein and blood leakage through the altered gastric mucosa. 1,8 Neither hypoproteinemia nor anemia developed in the Cairn terriers. It appears that the Cairn terriers developed gastric cancer before gastric mucosal damage was severe enough to result in leakage of protein or blood. This suggests that neoplasia may develop earlier in Ménétrier disease in Cairn terriers than in humans.
Ménétrier disease in humans is attributed to overexpression of transforming growth factor (TGF)–α with excessive stimulation of gastric epidermal growth factor receptors. 1 Most cases are considered to be idiopathic, but rare inherited forms of this disease have been reported. 4 As the 3 Cairn terriers in this report were siblings, an inherited predisposition to Ménétrier disease seems likely. Two of the Cairn terriers lived in the same household and received the same diet, but the third dog did not share this household or diet. This makes an environmental or dietary cause of Ménétrier disease less likely. Some cases of Ménétrier disease in children are caused by cytomegalovirus infection; 6 thus, the possibility that the disease in the Cairn terriers was due to viral infection cannot be excluded.
All 3 dogs of this report died because of gastric neoplasia. Gastric adenocarcinoma is uncommon in dogs, 3 so its development in all 3 littermates suggests a predisposition to neoplasia. Gastric neoplasia is a known sequel of Ménétrier disease in people. 8,11 Therefore, it is possible that the dogs had an inherited predisposition to Ménétrier disease that subsequently also predisposed them to gastric neoplasia. Gastric neoplasia has not been previously associated with canine hypertrophic gastropathy.
People with clinical Ménétrier disease typically undergo a partial or complete gastrectomy. 8 Although gastrectomy was considered the best option to prevent gastric neoplasia in case No. 3, this surgery is associated with significant morbidity in dogs. 9 The use of anti-inflammatory and gastric acid–reducing treatment has not been consistently efficacious in people with Ménétrier disease. 1 Such treatments were used in case No. 3, but it is unknown whether they prevented clinical signs of Ménétrier disease or affected disease progression.
In conclusion, this is the fourth report of canine hypertrophic gastropathy with histological features of Ménétrier disease and the first report of an association between hypertrophic gastropathy and gastric adenocarcinoma in a domestic species. As this disease developed in 3 siblings, an inherited predisposition appears likely. In 1 dog, Ménétrier disease remained asymptomatic for 2 years.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.