
Abstract
A 4.5-year-old intact male Labrador Retriever dog had a 1-month history of right forelimb lameness with painful swelling of the elbow. The radiographic findings of increased synovial mass with mineralized opacities and the gross and histologic findings in the synovial biopsy specimens were consistent with a diagnosis of primary (idiopathic) synovial osteochondromatosis. Twenty months after initial presentation, based on progression of clinical signs and radiographic evidence of marked bone lysis in the distal aspect of the humerus and proximal aspects of the radius and ulna, the affected leg was amputated. The histologic diagnosis was chondrosarcoma with fibroblastic differentiation and bone lysis. The chondrosarcoma was interpreted as malignant transformation of primary synovial osteochondromatosis.
Keywords
Primary synovial chondromatosis is a rare monoarticular disease characterized by intra-articular production of cartilage nodules (chondromas), some of which ultimately ossify, leading to the term osteochondromatosis. Less commonly, this lesion develops in the synovium of tendon sheaths or bursae. 10 Intra-articular chondromas often become loose bodies within the joint and continue to grow, nourished by synovial fluid. Once the nodules start to calcify, they must reattach to the synovium to grow further or ossify. 11
Secondary synovial chondromatosis is a sequel of joint abnormalities such as mechanical or arthritic conditions that result in intra-articular chondral bodies and is therefore more common than the primary form. 18 Predisposing conditions include osteoarthritis, osteochondritis dissecans, neuropathic osteoarthropathy, trauma, rheumatoid arthritis, osteonecrosis, and tuberculosis. 18
The classification of primary synovial chondromatosis remains controversial; evidence exists for both a reactive process and a “primary” metaplastic/proliferative one. 3 Recent cytogenetic studies suggest that primary osteochondromatosis is a benign neoplastic disease. This was supported by demonstrating that a subpopulation of cells interpreted as mesenchymal stem cells underwent clonal proliferation. 13
Malignant transformation of primary synovial chondromatosis in humans is considered extremely rare and is treated by amputation. 1 Most human patients have a long-standing disease history with multiple local recurrences. 12 Histologically, malignant transformation is hard to distinguish from the primary lesion due to overlapping cellular features. 3 In veterinary medicine, malignant transformation to chondrosarcoma has been reported only once, in a dog with intra- and extra-articular synovial chondromatosis. 4 The present report describes a case of primary synovial osteochondromatosis in the elbow of a dog that also underwent malignant transformation to chondrosarcoma.
Case History, Radiographic and Microscopic Findings
A 4.5-year-old neutered male Labrador Retriever dog was presented for an acute onset of lameness and swelling of the right elbow of 1 month’s duration. Synovial fluid culture results were negative. On physical examination, marked swelling and crepitus were noted around the elbow; palpation seemed to cause pain. Six days later, numerous cartilaginous fragments and irregular articular surfaces were encountered upon surgical exploration of the elbow joint. The cartilaginous fragments were submitted to a private pathology practice and diagnosed as “mildly disorganized fibrocartilage and chondro-osseous tissue and reactive, chronic, hyperplastic, erosive/ulcerative synovitis/joint capsulitis.” On reexamination, the dog was still moderately lame, but the swelling had markedly decreased.
Six months after initial presentation, the dog had an acute onset of non-weight-bearing lameness in the right foreleg with a firm swelling of the elbow. Radiographically (Fig. 1), abundant lobular, heterogeneous, mineral-opacity material had accumulated along the distal aspect of the humerus and proximal aspects of the radius and ulna. The soft tissues surrounding the elbow joint were swollen. Multiple 5 to 35 mm-diameter nodules were surgically removed and submitted to a private pathology practice. The histologic diagnosis was “multiple intra-articular hyaline cartilaginous fragments (presumptive fragmented chondroma).” Postsurgery radiographs demonstrated that most of the mineral-opacity material had been removed. The soft tissues surrounding the elbow joint remained swollen.
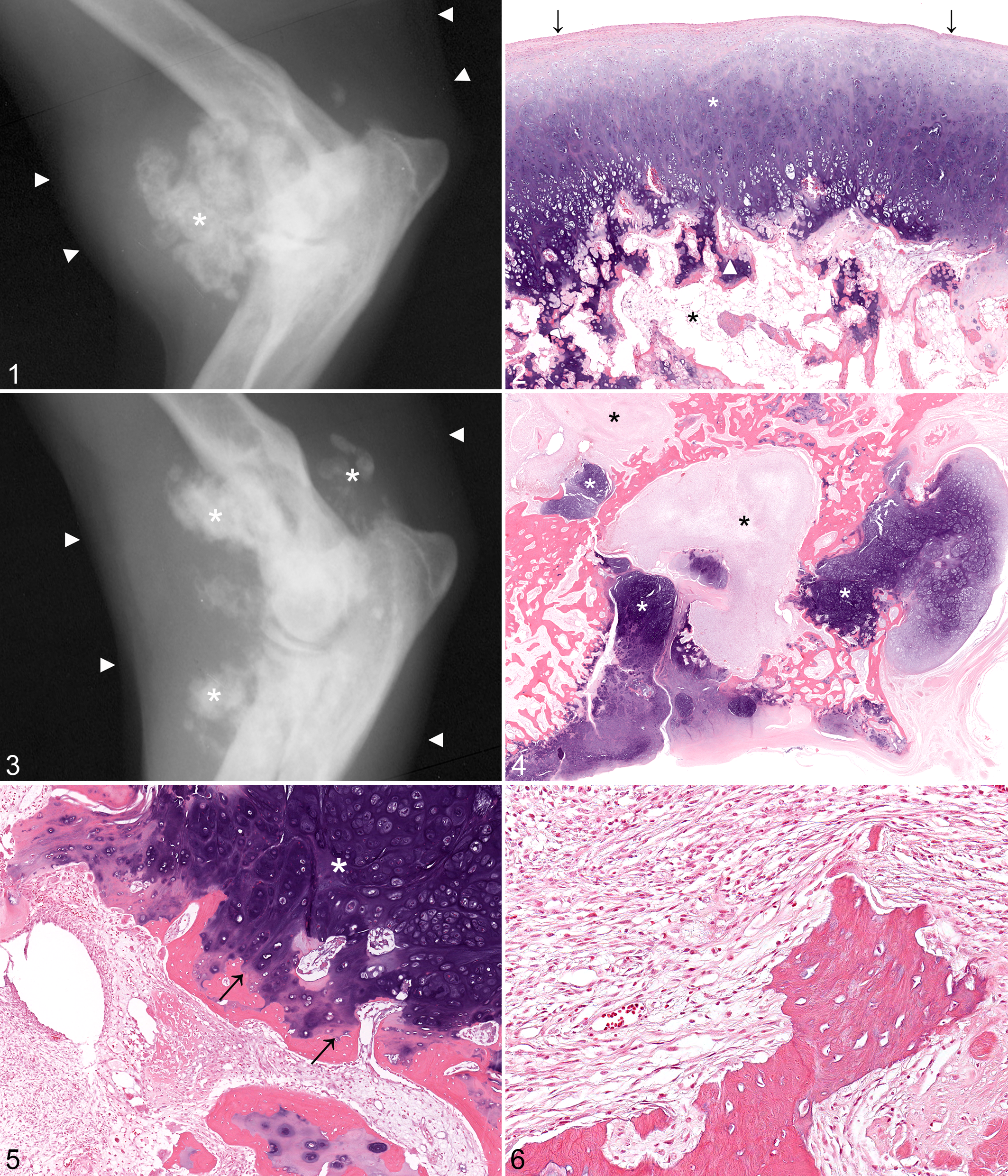
Eight months after initial presentation, the dog was mildly lame in the right foreleg, with reduced range of motion of the elbow. A sample of joint capsule containing firm nodules was submitted for histologic evaluation. Specimens were received in 10% neutral buffered formalin, decalcified in formic acid/sodium citrate solution (50%/20%), routinely processed, embedded in paraffin, sectioned at 5 μm, and stained with hematoxylin and eosin. Histologically, polypoid to multinodular masses ranged in diameter from 4 to 30 mm. The abnormal tissue consisted of well differentiated hyaline to fibrocartilage with variable chondrocyte cluster formation in the hyaline cartilage and areas of endochondral ossification that comprised 0% to 60% of the individual fragments. The surface of the fragments was bordered by 1 to 2 layers of fibrous tissue that blended with synoviocytes at the margins of some fragments. Fragments with more extensive endochondral ossification had a fatty marrow with myxomatous metaplasia (Fig. 2). The sections were without cellular atypia, mitotic figures, or necrosis. The diagnosis was synovial osteochondromatosis. Radiography was repeated 17 months after initial presentation (Fig. 3); the mineral-opacity deposits extended more distally along the forelimb in comparison to previous radiographs. Bony lysis was evident in the medial humeral epicondyle, cranial and medial aspect of the radial head, and the anconeal process. The subchondral bone of the ulnar notch was ill-defined. Soft tissue swelling surrounded the elbow joint and extended distally and laterally.
At 20 months after initial presentation, lameness was severe with decreased range of motion in the elbow and a firm swelling on its medial aspect. Radiographic evaluation showed that the mineralization and bony lysis had progressed. The limb was amputated 2 days later and submitted to The Ohio State University for pathologic evaluation. In sections of the proximal aspect of the radius and ulna, irregular islands of well-differentiated chondrosarcoma invaded the bone with areas of endochondral ossification and contiguous intraosseous areas of an invasive, moderately differentiated fibroblastic component (Fig. 4). Zones of transition between the well-differentiated chondrosarcoma and the fibroblastic component were not observed. There were 3 mitotic figures per 10 high-power fields in the fibroblastic component. There was no evidence of necrosis or inflammation. The margin between adjacent bone and chondrosarcoma was either regular or had areas of penetration of chondrosarcoma into dilated marrow sinusoids. Most margins of the chondrosarcoma were lined by well-differentiated bone secondary to endochondral ossification or osseous metaplasia at the periphery of the tumor (Fig. 5). The margins of bone at the interface with the fibroblastic portion of the chondrosarcoma were scalloped, indicating osteoclastic resorption (Fig. 6). The bone between areas of neoplastic tissue varied among compact, lamellar, osteonal, or woven. The diagnosis was synovial osteochondromatosis with malignant transformation to well differentiated chondrosarcoma with areas of fibroblastic differentiation.
According to the owners, the dog survived for 1 year after the amputation, when it developed labored breathing and abdominal distention as well as loss of mobility in the hind quarters. The local veterinarian considered this to be consistent with metastatic disease, and the dog was euthanized without additional diagnostic studies or postmortem examination.
Discussion
Based on the history, the presence of nodules and loose bodies of cartilage within the joint, and the radiographic and histologic appearance of the lesions, the diagnosis was primary synovial osteochondromatosis (intra-articular) with malignant transformation to chondrosarcoma. Surgery to remove the synovial lesion was performed at initial presentation, as well as 6 and 8 months later. By 17 months after initial presentation, bone lysis had developed. At 20 months, the leg was amputated due to marked bone lysis.
Histologically, primary synovial chondromatosis presents as lobules of hyaline cartilage with overlying synovial lining that is often attenuated. The hyaline cartilage is usually hypercellular with nuclear atypia (multinucleated cells, nuclear crowding, nuclear enlargement and hyperchromasia). These features make it hard to distinguish this benign condition from a malignant cartilaginous neoplasm. 12 In human medicine, features of neoplastic transformation include replacement of the typical “clustering” pattern with a more sheetlike arrangement of chondrocytes, changes in the matrix, spindle cell proliferation of the chondrocytes, foci of necrosis, and bone invasion. 1
In veterinary medicine, primary synovial (osteo-) chondromatosis has been described in dogs, 4 –7,16 horses, 9,14,15 pigs, 19 and raptors (mainly great horned owls). 8,17 There appears to be no age, breed, or species predilection. A case of malignant transformation to chondrosarcoma was reported in a dog with intra- and extra-articular primary synovial chondromatosis of the stifle joint. 4
The differential diagnosis in this case included secondary synovial osteochondromatosis, soft tissue chondromas, and primary synovial chondrosarcoma.
The history did not include trauma. Although mild to moderate degenerative changes were grossly evident in the articular cartilage at the first surgery, there was no clinical evidence of preexisting degenerative joint disease, and the cartilage surface changes were insignificant compared with the massive proliferations in the synovium. Secondary synovial chondromatosis was considered unlikely because the nodules are reportedly less numerous (< 5), 10 whereas this case had more than 10 nodules. Furthermore, histologic characteristics (eg, concentric laminations in the cartilaginous nodules 12 ) of secondary synovial chondromatosis were absent in this case.
The histologic distinction between synovial chondromatosis and synovial chondrosarcoma is unclear. All reports of human synovial chondrosarcoma were considered cases of malignant transformation of synovial (osteo-) chondromatosis. In the veterinary literature, only 1 synovial chondrosarcoma was included in a series of synovial tumors. Details of the case were not presented; however, there was no indication that it was preceded by synovial chondromatosis. 2
Because this chondrosarcoma had 2 distinct tissue components (cartilaginous and fibroblastic) without an apparent transition zone, the coexistence of 2 independent neoplasms is possible but unlikely. Coincidental and independent synovial chondromatosis and synovial chondrosarcoma also remain a theoretical possibility in this case; however, this has not been reported and could be difficult to distinguish from malignant transformation.
Footnotes
Acknowledgements
We thank Idalia Romero for providing medical records and follow-up information on the dog, as well as Astrid Bonnegarde for her translation of the French literature.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.