
Abstract
Lymphoma in the left femoral nerve of a 10-year-old English Cocker Spaniel caused complete paralysis of the affected limb. Neoplastic cells were immunopositive for CD79a and Pax5 and negative for CD3. Neoplastic cells were in multiple lymph nodes and one kidney but spared bone marrow. The clinical and histologic features in this case resemble those of the rare human condition of neurolymphomatosis.
Neurolymphomatosis is a rare condition defined as infiltration of peripheral nerves or nerve roots by neurotropic lymphoma or leukemia. 1–3 In humans, there are 4 basic clinical presentations: painful polyneuropathy or polyradiculopathy, cranial neuropathy, painless polyneuropathy, and peripheral mononeuropathy. 1 The syndrome may occur as the initial manifestation of neoplastic disease, present concurrently with systemic neoplasia, or represent progression of disease in patients diagnosed and previously treated for lymphoma or leukemia. 1,3,7,8 Most human neurolymphomatosis cases are diffuse large B-cell lymphomas when classified by the Revised European-American Lymphoma or World Health Organization system. 3,4
Lymphoma and leukemia are well recognized in veterinary medicine, and lymphoma is one of the most common neoplasias of cats and dogs. The majority of lymphomas in these species occur in parenchymatous organs and/or peripheral lymph nodes, with occasional primary or secondary involvement of the brain and spinal cord. 5 , 9–12 Involvement of peripheral nerves (neurolymphomatosis) is rarely reported in veterinary species. We report a case of a dog with multicentric B-cell lymphoma involving the left femoral nerve and compare its gross, histologic, and immunohistochemical features to those of previous canine and human cases.
Case History
A 10-year-old spayed female English Cocker Spaniel was presented to the Colorado State University Veterinary Teaching Hospital for evaluation of left pelvic limb lameness. Prior history included protein-losing nephropathy, hypertension, and intermittent spinal pain with medically managed episodes of spinal hyperpathia and moderate paraparesis in the past 6 years. The dog had been treated surgically for intervertebral disk disease by L3-L4 hemilaminectomy and rhizotomy of the right L3 nerve root 3 months before presentation. Upon examination, the dog had severe weight-bearing lameness and muscle atrophy in the left pelvic limb. Evidence of pain could not be elicited on manipulation of the stifle and tarsal joints nor the long bones, but inconsistent pain was elicited upon extension of the left hip. Consistent painful response was elicited by palpation of the left mid to caudal lumbar epaxial muscles. The lameness progressed insidiously for several months despite institution of prednisone, increasing doses of tramadol and gabapentin, and incorporation of methocarbamol and amantadine. Eventually, the dog lost the patellar reflex in the affected limb. A left femoral neuropathy or L4-L6 radiculomyelopathy was suspected. The dog became lethargic and anorexic and was euthanized due to poor quality of life.
Pathologic Findings
Methods
At necropsy, representative sections of lesions and routine organs were collected and fixed in 10% neutral buffered formalin. Fixed tissues were trimmed, processed routinely, sectioned at 4 μm, and stained with hematoxylin and eosin for histologic evaluation. Immunohistochemistry was performed with standard alkaline phosphatase methods for detection of CD79a (CM067C, Biocare Medical, Concord, CA) and CD3 (A0452, Dako, Carpenteria, CA). Standard horseradish peroxidase methods were used for detection of Pax5 (610863, BD Biosciences, San Diego, CA). All immunohistochemistry preparations were counterstained with hematoxylin, dehydrated, and mounted in xylene-based mounting medium. Canine lymph node was used as positive control tissue. For negative controls, normal mouse and rabbit sera were substituted for the CD79a and CD3 primary antibodies, respectively.
Gross Findings
At necropsy, a thick cordlike subcutaneous mass extended from the left inguinal area to a point just caudomedial to the stifle. This cylindrical mass, 1.0 cm in greatest diameter, paralleled the femoral artery for a short distance before coursing superficially under the subcutis (Fig. 1). The mass had a blunt end proximally and multiple flattened branches distally, which coursed through the subcutaneous tissue and between muscle bundles. The mass was white to tan, firm, and homogeneous on cut section. No gross lesions were identified in the spinal cord, spinal nerve roots, peripheral nerves, or ganglia. Additional gross findings included mild systemic lymphadenomegaly, chronic intervertebral disk protrusion with mild spinal cord impingement at L2-L3, duodenal lymphangiectasia, and an evenly enlarged pituitary gland (1.0 × 0.6 × 0.6 cm).
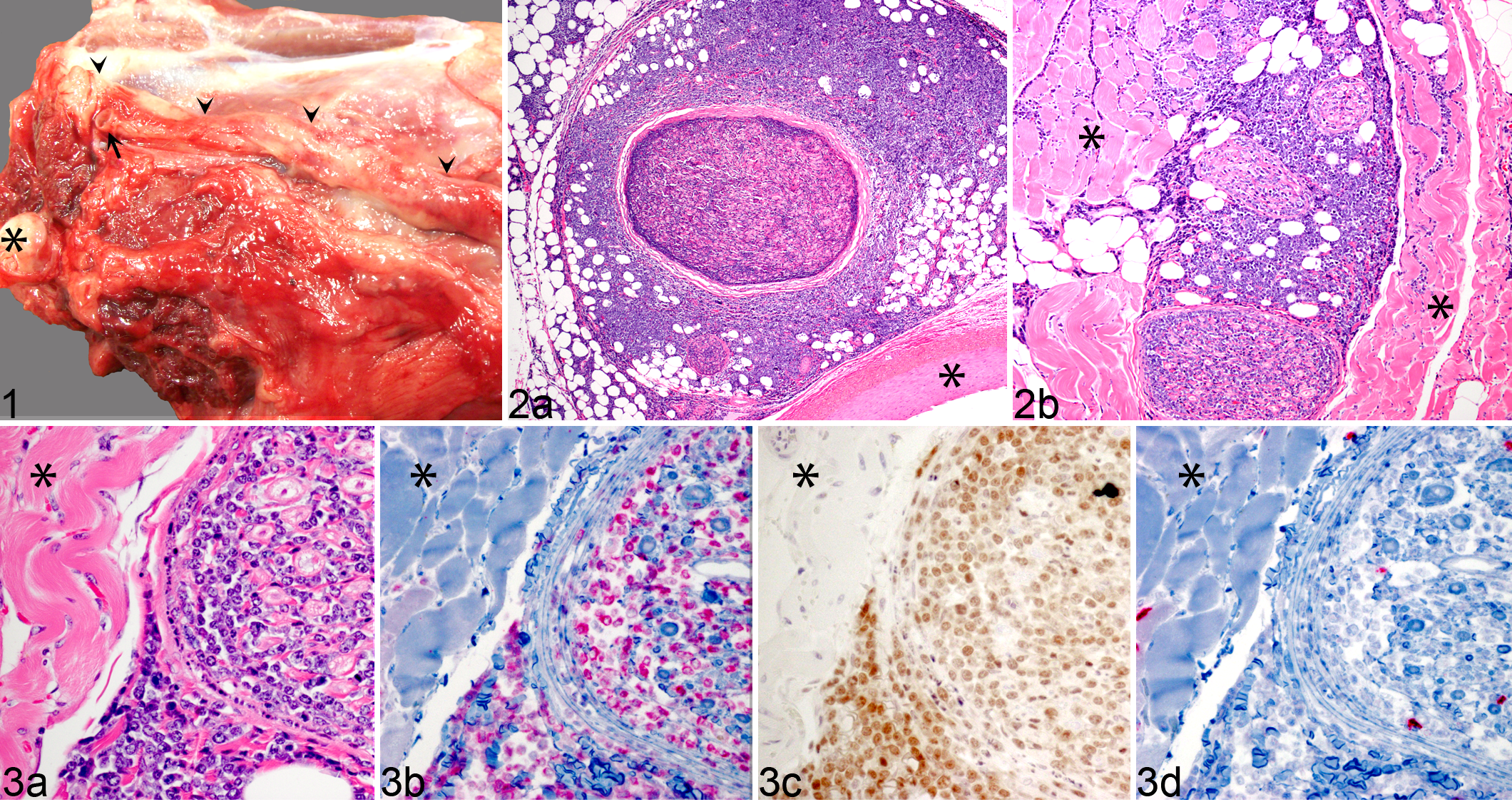
Dog, neurolymphomatosis. Left pelvic limb, medial view. Neoplastic infiltration has resulted in thickening of the exposed segment of femoral nerve (arrowheads). Note femoral artery (arrow) and femoral head (asterisk).
Histologic Findings
Medium-sized neoplastic lymphocytes expanded the endoneurium and perineurium of the left femoral nerve and multiple intramuscular nerve branches and deeply infiltrated adjacent muscle and adipose tissue (Fig. 2a, b). These neoplastic cells had discrete cell borders, scant to moderate amounts of amphophilic cytoplasm, and round nuclei with vesicular to coarsely clumped chromatin and 1 to 2 nucleoli. There was mild anisocytosis and anisokaryosis, with cells measuring 1 to 1.5 times the diameter of a red blood cell. Mitotic figures were in excess of 50 per 10 fields (400×). Apoptotic bodies were scattered throughout the neoplastic tissue. Marked axon loss was observed in affected nerve branches. Remaining axons were separated by neoplastic lymphocytes; myelin sheaths were dilated. Where neoplastic cells invaded muscle, there was moderate variation in myofiber cross-sectional area, and many fibers were markedly attenuated due to the compressive effects of the neoplastic cells. Many myocytes were necrotic with variable cytoplasmic hypereosinophilia, loss of cross striations, and pyknosis. Other myofibers had multiple central, linearly arranged vesicular nuclei with prominent nucleoli and subtle cytoplasmic basophilia (regeneration).
Additional histologic findings included infiltration and effacement of multiple lymph nodes (submandibular, mesenteric, and popliteal) by neoplastic lymphocytes. The peripelvic medullary interstitium of 1 kidney was moderately expanded by sheets of neoplastic cells. The interstitium of both renal cortices was multifocally infiltrated by reactive lymphocytes. Both kidneys had moderate diffuse global membranoproliferative glomerulonephritis with mild glomerulosclerosis. Sections of the spinal cord distal to L2 had few scattered spheroids and rare digestion chambers. Incidental findings included mild eosinophilic enteritis, mild centrilobular hepatocellular vacuolar degeneration, splenic and adrenocortical extramedullary hematopoiesis, and a craniopharyngeal pituitary cyst.
Immunohistochemistry
Neoplastic cells in the nerve, nerve branches, adjacent muscle, and submandibular and mesenteric lymph nodes had strong diffuse cytoplasmic and membranous expression of CD79a and strong nuclear expression of Pax5 (Fig. 3b, c). The cells were negative for CD3 (Figure 3d). Neoplastic cells near the renal pelvis also were CD79a positive and CD3 negative. In both kidneys, scattered small CD3-positive lymphocytes colocalized with CD79a-positive lymphocytes in the cortical interstitium, consistent with chronic lymphoplasmacytic interstitial nephritis.
Discussion
Reports of lymphoma involving peripheral nerves are rare in veterinary medicine. Neurotropic lymphoma has been reported in one dog with progressive weight loss and bilateral trigeminal neuropathy. 6 The distribution of lymphoma in that dog was extensive, with histologic effacement of the trigeminal nerves and infiltration of the recurrent laryngeal, mesenteric, vagus, and spinal nerves; trigeminal musculature; lymph nodes; bone marrow; and meninges. Neoplastic cells were detected in cerebrospinal fluid but not in the parenchyma of the central nervous system. Immunohistochemistry was not reported; thus, the immunophenotype of the lymphoma in that dog is unknown.
In contrast to the previously reported canine case, no nerves other than the femoral nerve and no nerve roots were involved in the dog of this report. Bone marrow was not involved, and dissemination to the meninges was not detected grossly or histologically. Cranial nerves were not evaluated histologically, but the dog had no apparent cranial nerve deficits. As in most human cases, the lymphoma in this dog had a histologic and clinical pattern consistent with diffuse non-Hodgkin large B-cell lymphoma. Because this lymphoma was detected postmortem, it is not known whether the case represents primary peripheral nerve involvement with secondary systemic spread or nodal lymphoma with progression to peripheral nerve involvement. Chronic prednisone treatment may have hampered the antemortem identification of peripheral lymphadenomegaly.
Though rare, neurolymphomatosis should be considered in the differential diagnosis for chronic progressive peripheral mononeuropathy or polyneuropathy, with or without a history of lymphoma. As in human medicine, magnetic resonance or other imaging and biopsy of affected nerves may facilitate antemortem diagnosis in veterinary patients. Further characterization of neurolymphomatosis in veterinary species will depend on identification of additional cases antemortem, a challenging task given the rarity of the condition, low index of clinical suspicion, and variable clinical presentation.
Footnotes
Acknowledgement
We thank Charlie Kerlee and Jay Oaks for assistance with images.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.