
Abstract
An 8-y 9-mo-old male Pug dog was presented because of anorexia, hindlimb ataxia, vomiting, and progressive weight loss. Clinical examinations revealed atrophic hindlimb muscles with decreased postural reaction, enlargement of the cardiac silhouette and megaesophagus on radiograph, and reduced cardiac contractility on ultrasonography. The dog died 10 d after the initial examination, and an autopsy was performed. Grossly, the heart was enlarged, with multifocal-to-coalescing extensive plaque-like areas of discoloration on the epicardial surface. On cross-section, the ventricles were moderately dilated, and discoloration extended into the myocardium. Peripheral lymph nodes were of normal size. Histologically, atypical lymphoid cells replaced the myocardium and also extensively infiltrated peripheral nerve bundles in various organs. With immunohistochemistry, the neoplastic cells exhibited strong immunoreactivity for CD3 and CD20, and were negative for CD8, granzyme B, CD79α, and Pax5. Double-label immunofluorescence confirmed co-expression of CD3 and CD20 by the neoplastic cells. Molecular clonality analysis presented a clonal T-cell receptor gamma gene rearrangement. The case was diagnosed as a CD3+/CD20+ peripheral T-cell lymphoma with prominent cardiac and peripheral nerve involvement, indicating neurolymphomatosis.
A 6.16-kg, 8-y 9-mo-old male Pug dog was presented to the Veterinary Medical Center of Obihiro University of Agriculture and Veterinary Medicine because of anorexia, hindlimb ataxia, vomiting, and progressive weight loss. On physical examination, bilateral atrophy of the hindlimb muscles and a decreased postural reaction were noted. Radiography showed enlargement of the cardiac silhouette and megaesophagus. Myasthenia gravis was unlikely, as the acetylcholine receptor antibody value was within the normal range, at 0.02 nmol/L (reference interval [RI]: 0.0–0.6 nmol/L). Cardiac ultrasonography confirmed reduced cardiac contractility with left ventricular fractional shortening of 11.3%, and did not detect significant pericardial effusion. Complete blood count and serum biochemistry did not reveal any disease-specific abnormalities, with an elevated platelet count (706 × 109/L, RI: 200–500 × 109/L), alanine transaminase activity (ALT; 129 U/L, RI: 10–100 U/L), aspartate transaminase activity (AST; 83 U/L, RI: 0–50 U/L), and creatine kinase activity (CK; 342 U/L, RI: 10–200 U/L). Reduced levels of total protein (50 g/L, RI: 60–80 g/L), albumin (20 g/L, RI: 22–39 g/L), and total cholesterol (2.43 mmol/L, RI: 2.85–8.29 mmol/L) were present. The patient was prescribed pimobendan at a daily dosage of 0.4 mg/kg, but died 10 d after the initial examination, and an autopsy was performed.
At autopsy, the heart was round and enlarged. Multifocal-to-coalescing plaque-like areas of pale-yellow discoloration were seen extensively on the epicardial surface and extended into the myocardium (Fig. 1A). The ventricular lumens were bilaterally and moderately dilated. Peripheral lymph nodes were of normal size, and the thymus was not visible. Other gross findings included a dilated esophagus, multiple ulcers and erosions of the esophageal mucous membrane, and a 28 × 25× 22 mm polycystic structure in the cranial mediastinum.
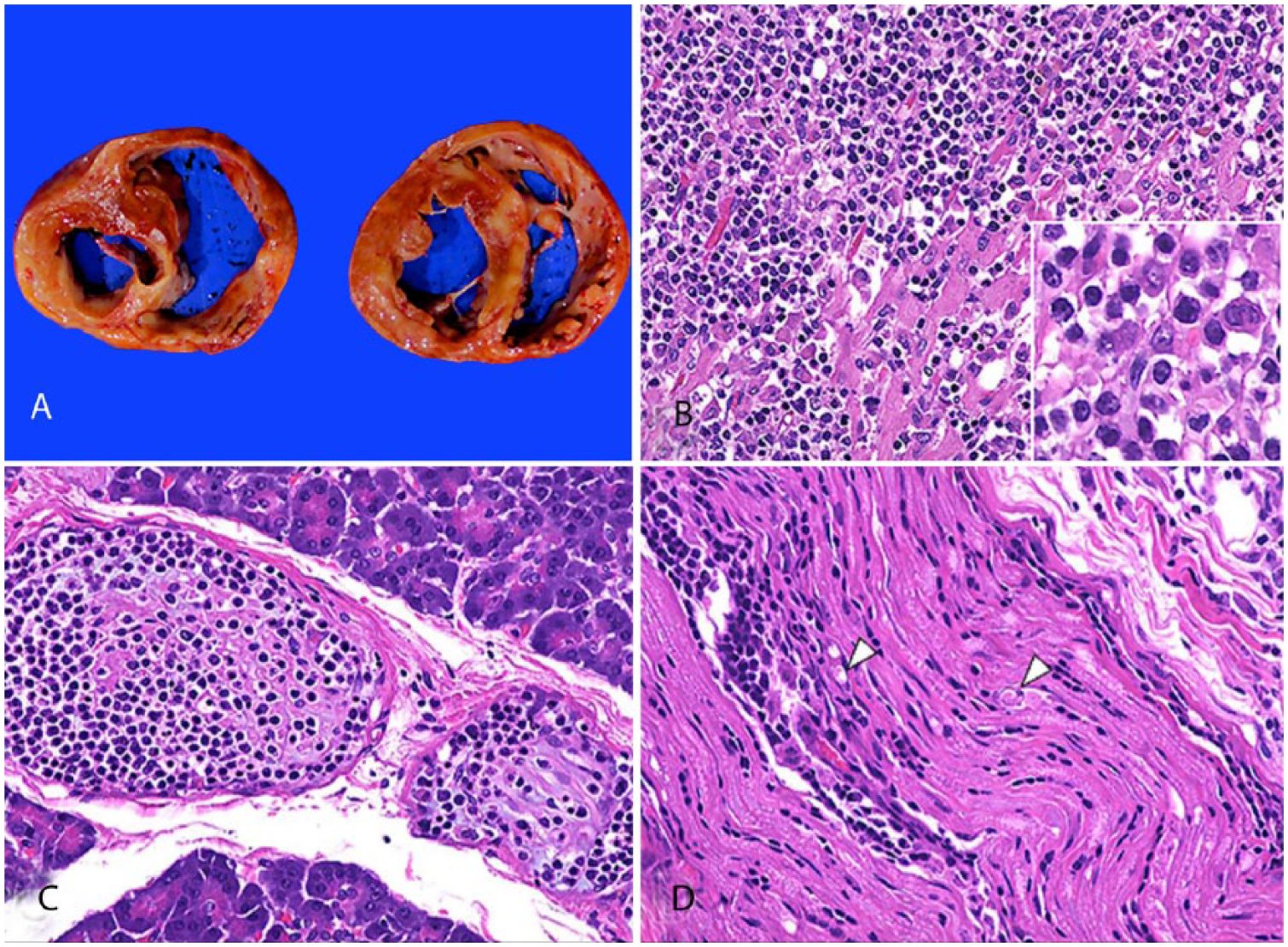
Peripheral T-cell lymphoma with cardiac and peripheral nerve involvement in a Pug dog.
Tissues were fixed in 15% neutral-buffered formalin and processed routinely, sectioned at 4 μm, and stained with hematoxylin and eosin. Histologic examination of the heart revealed densely packed small (~1.2 times the size of erythrocytes), round, atypical lymphoid cells infiltrating and replacing the myocardium. The neoplastic cells had discrete cell borders, variable amounts of slightly eosinophilic cytoplasm, and pleomorphic, often hyperchromatic, nuclei with moderate anisokaryosis (Fig. 1B). There were 10–20 mitotic figures per high-power field (400×). Uniform medium-sized lymphocytes, plasma cells, histiocytes, mast cells, and occasional eosinophils moderately infiltrated the neoplastic foci. The neoplastic cells also extensively infiltrated peripheral nerve bundles in various organs including the liver, spleen, kidney, heart, lung, pancreas (Fig. 1C), adrenal gland, and the gastrointestinal tract (esophagus, stomach, duodenum, jejunum, ileum, cecum). Additionally, the sciatic nerves (Fig. 1D), trigeminal nerves, and the cervical spinal nerves of C4 and C5 were bilaterally infiltrated by small numbers of neoplastic cells. The sciatic nerve had axonal degeneration and mild macrophage infiltration. No neoplastic infiltration was detected in the brain (at levels of frontal lobe, corpus striatum, diencephalon, occipital lobe, mesencephalon, pons, medulla oblongata, cerebellum) or spinal cord (from cervical cord to cauda equina, at levels of every spinal nerve). The kidney (interstitium), pituitary gland (pars distalis), gastrointestinal tract (lamina propria, submucosa, muscularis of stomach, duodenum, jejunum, ileum, cecum, colon), and urinary bladder (muscularis) were organs other than the heart with neoplastic lymphocyte infiltrates in the parenchyma, in addition to peripheral nerve involvement in each organ. Histopathologic findings were consistent with a diagnosis of lymphoma with prominent myocardial and peripheral nerve involvement.
Additional major histologic observations included group atrophy of triceps brachii and biceps femoris muscle fibers. Splenic nodular hyperplasia, thyroidal cysts, and epididymo-orchitis and testicular granuloma were incidental findings. The polycystic structure observed in the mediastinum was diagnosed as multiple thyroglossal cysts.
For further characterization of the neoplastic lymphocytes, immunohistochemistry was performed on serial sections of the heart and hepatic peripheral nerve bundle according to a protocol described previously. 13 The antibodies used were as follows: monoclonal mouse antibody against CD3 (1:100, clone F7.2.38; Dako, Tokyo, Japan); polyclonal rabbit antibody against CD8 (1:200; Abcam, Tokyo, Japan); polyclonal rabbit antibody against granzyme B (1:400; Spring Bioscience, Pleasanton, CA); polyclonal rabbit antibody against CD20 (1:400; Thermo Fisher Scientific, Fremont, CA); monoclonal mouse antibody against CD79α (ready-to-use, clone JCB117; Dako); and polyclonal rabbit antibody against Pax5 (1:500; Thermo Fisher Scientific). Antigen retrieval involved microwave heat pretreatment at 97°C, for 15 min in citrate buffer solution (pH 6.0) for CD3, CD8, granzyme B, CD20, and Pax5, and in target retrieval solution (pH 6.1; Dako) for 20 min for CD79α. Slides with each primary antibody were incubated overnight at 4°C in a humidified chamber. The secondary antibodies were incubated for 30 min at room temperature. Tissue sections in which the primary antibodies were replaced by phosphate-buffered saline served as negative controls; a normal canine lymph node and spleen were used as positive controls.
The neoplastic cells, both in the myocardium and around peripheral nerve bundles, consistently expressed CD3 (Fig. 2A) and CD20 (Fig. 2B). No immunoreactivity was observed to CD8, granzyme B, CD79α, or Pax5 in the neoplastic cells. Given the apparent co-expression of CD3 and CD20 antigens by the neoplastic cells, a double immunofluorescence staining protocol was performed. Briefly, following antigen retrieval, the slides were incubated with 25% Block Ace solution (DS Pharma Biomedical, Osaka, Japan) for 20 min at room temperature, in order to reduce nonspecific binding. The CD3 (1:100) and CD20 (1:400) antibodies were applied as a mixture overnight at 4°C. Alexa Fluor 488–conjugated goat anti-mouse IgG (1:200; Thermo Fisher Scientific) and Alexa Fluor 594–conjugated goat anti-rabbit IgG (1:200; Thermo Fisher Scientific) were applied as secondary antibodies as a mixture and incubated for 30 min at room temperature. Nuclei were counterstained with 4′,6-diamidino-2-phenylindole (Vector Laboratories, Burlingame, CA), and antigen localization was evaluated (BZ-X700 all-in-one fluorescence microscope, Keyence, Osaka, Japan). Negative and positive controls were run as described above.
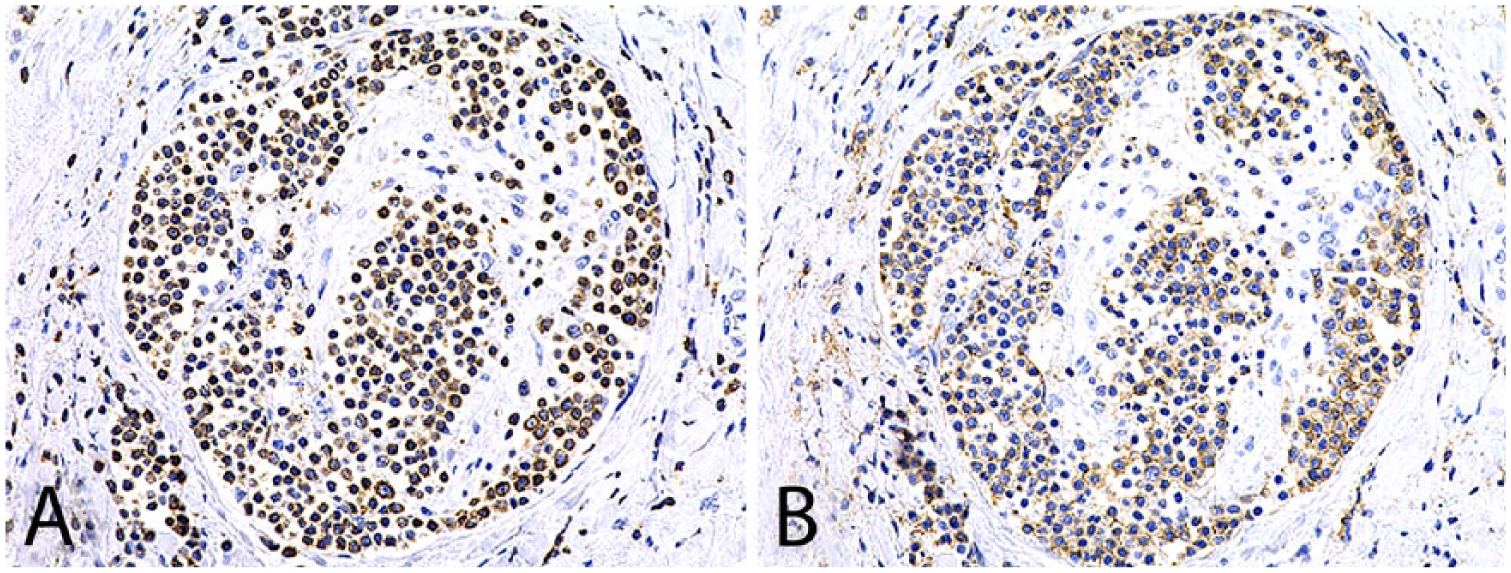
CD3+/CD20+ peripheral T-cell lymphoma with cardiac and peripheral nerve involvement in a Pug dog. Neoplastic lymphocytes in a hepatic peripheral nerve bundle show strong immunoreactivity to both CD3
Co-expression of CD3 and CD20 was confirmed in >90% of the neoplastic cells; positivity to CD3 was shown in the cytoplasm, and CD20 in the cell membrane (Fig. 3). Subsequently, a PCR for antigen receptor rearrangement was performed as described previously. 5 Genomic DNA was extracted from the heart stored at −80°C (QIAamp DNA mini kit, Qiagen, Hilden, Germany), according to the manufacturer’s instructions. Analysis of the neoplastic lymphocytes detected a clonal T-cell receptor gamma (TCRγ) locus rearrangement; there was no amplification of the immunoglobulin heavy chain (IgH) minor gene and a smear indicating a polyclonal rearrangement of the IgH major gene (Fig. 4). Duplicate samples were tested for validation of results. Based on morphologic and immunohistochemical staining characteristics with confirmation of a TCRγ locus rearrangement, the final diagnosis of the neoplasm was a CD3+/CD20+ peripheral T-cell lymphoma, with prominent cardiac and peripheral nerve involvement.
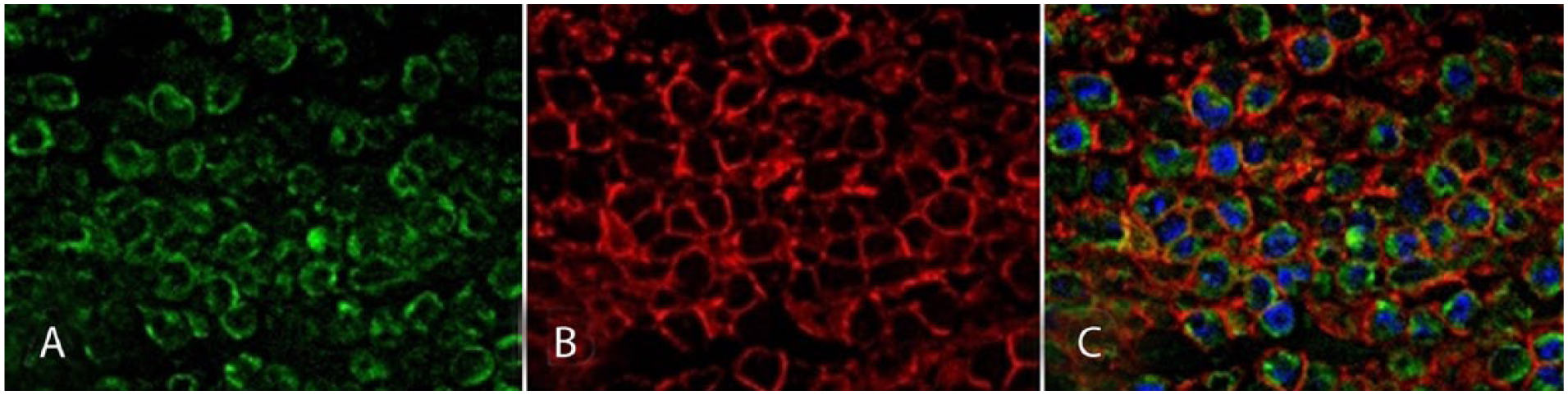
CD3+/CD20+ peripheral T-cell lymphoma with cardiac and peripheral nerve involvement in a Pug dog. Labeling of neoplastic lymphocytes in the heart with anti-CD3 (green;
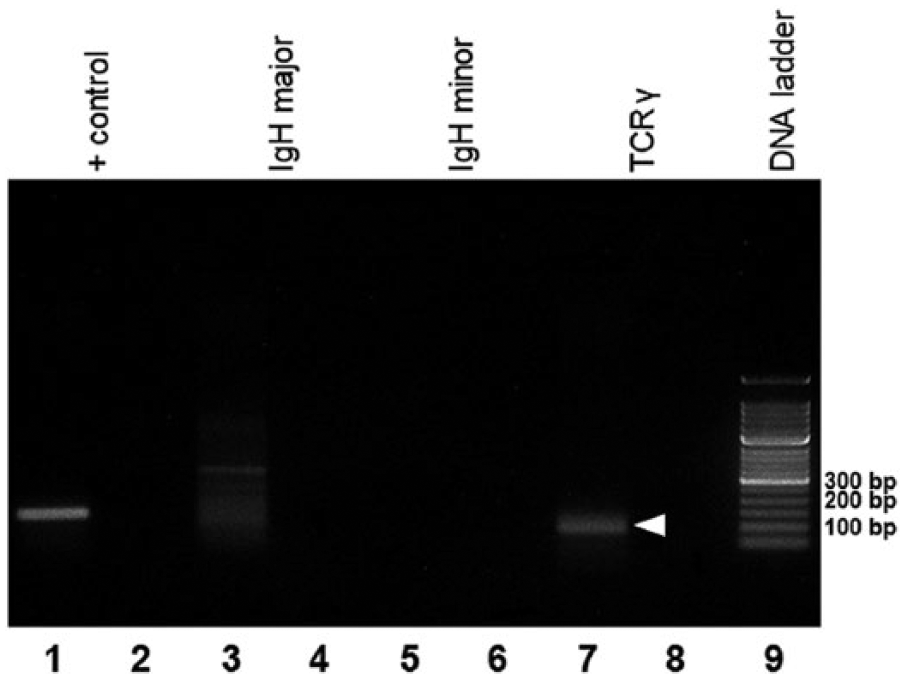
Agarose gel electrophoresis demonstrating results of PCR for antigen receptor rearrangements. Lanes 1, 2: positive control Cμ; lanes 3, 4: immunoglobulin heavy chain (IgH) major; lanes 5, 6: IgH minor; lanes 7, 8: T-cell receptor gamma (TCRγ); lane 9: 50-bp DNA ladder marker. For each primer, the first lane shows the case material, and the following lane shows the negative control. A single, monoclonal band is confirmed only for the TCRγ locus at ~90 bp (arrowhead).
Our case emphasizes the importance of combining immunohistochemical analysis and clonality testing for the accurate diagnosis of lymphoma. The neoplastic cells of our case were immunoreactive to CD3 and CD20, through an immunohistochemical panel (anti–T-cell antigen antibodies: CD3, CD8, granzyme B; anti–B-cell antigen antibodies: CD20, CD79α, Pax5). Meanwhile, duplicate samples subjected to clonality testing confirmed a clonal TCRγ gene rearrangement and a lack of IgH gene rearrangement of the infiltrating neoplastic cells, therefore indicating a T-cell lymphoma with an aberrant immunophenotype of CD20 expression. The occurrence of T-cell lymphomas co-expressing T- and B-cell markers has been described as rare cases in the veterinary literature. Although extremely limited, dogs have the most reported cases including the following: CD3+/CD79α+ T-cell lymphoblastic lymphoma 18 ; CD3+/CD20+/Pax5− mycosis fungoides 4 ; CD3+/CD20+/CD79α− and CD3+/CD20+/CD79α+/Pax5+ lymphomas. 15 Although ours was a case of CD3+/CD20+ T-cell lymphoma, CD3+ B-cell lymphomas have also been described in dogs and cats.3,7,22
CD20 has long been designated as a pan–B-cell antigen, consistently expressed from the pre–B-cell to mature B-cell stages. 6 On the other hand, CD3 is a T-cell–specific marker present from the early prothymocyte to mature T-cell stages and in natural killer (NK) T-cells.2,6 Cellular localization of this antigen depends on the stage of the cell, where cytoplasmic expression appears before its detection in the cell surface of thymocytes, as reported in humans. 21 The neoplastic cells in our case presented with CD3 expression localized in the cytoplasm. In view of the cytoplasmic CD3 expression and negative immunoreactivity to CD8 and granzyme B (antigens of cytotoxic T-cells and NK-cells), the neoplastic cells likely retained immature, lymphoblastic properties.
The co-expression of T- and B-cell markers identified in our case may be explained by 1 of 2 main hypotheses proposed in human cases. The first describes an existing small subpopulation of T-cells expressing CD20 in the peripheral blood and bone marrow.1,9 Also, a study using T-cells in lymph nodes of rhesus monkey models demonstrated that lymphocyte activation would induce the expression of CD20 in T-cells. 12 Thus, a CD3+/CD20+ T-cell lymphoma may originate from either a normal subpopulation of CD20+ T-cells or from activated T-cells through neoplastic transformation. The second hypothesis is that the aberrant expression of CD20 in the neoplastic T-cells was acquired during malignant transformation of these cells. This idea is supported by a study reporting that up to 60% of human mycosis fungoides cases with large cell transformation pick up CD20 expression that was not present in the initial biopsy sample. 10 Although the exact explanation to the CD20 expression in T-cells of our case is unknown at this time, it is noteworthy that other B-cell markers (CD79α and Pax5) were negative on these neoplastic cells.
The uniqueness of our case is not limited to the co-expression of CD3 and CD20 but also includes neurotropism of the neoplastic cells. Although lymphoma is one of the more common types of cardiac tumors, 19 nervous system involvement is rarely reported in canine lymphoma cases.14,16,17,20 Neurolymphomatosis refers to a rare manifestation of lymphoma or leukemia involving neoplastic infiltration of peripheral nerves. 8 The clear involvement of the peripheral nervous system, but not the central nervous system, in our case is compatible with a diagnosis of neurolymphomatosis. Multiple organ involvement including the liver, spleen, kidney, pancreas, and pituitary gland has been described previously in a case of canine neurolymphomatosis, 20 but cardiac involvement is an unusual presentation.
The hindlimb ataxia was thought to be the result of direct axonal damage in the sciatic nerves by infiltrating neoplastic cells plus neurogenic muscle atrophy. Additionally, neuropathic pain as reported in dogs, horses, and humans with neurolymphomatosis may have contributed to this presentation.8,11,17 The neoplastic lymphocytes infiltrating the peripheral nerves innervating the esophagus may have led to its marked dilation; however, this was not confirmed. Furthermore, the low levels of total protein, albumin, and total cholesterol identified during initial examination could be explained by the direct and indirect effects of intestinal infiltration of neoplastic lymphocytes, including possible intestinal mucosal leakage. Despite the rarity of occurrence, neurolymphomatosis should be considered as a differential diagnosis for progressive neuropathy, including conditions such as lameness and megaesophagus.
Footnotes
Acknowledgements
We thank Ms. Akiko Tomikawa for her assistance in histologic processing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.