
Abstract
A 3-year-old Cairn Terrier dog that had been in contact with sea water containing cyanobacteria (blue-green algae) was euthanized because of acute hepatic failure and anuria after a 5-day illness. Histologic findings included lytic and hemorrhagic centrilobular hepatocellular necrosis and renal tubular necrosis. The cyanotoxin nodularin was detected in liver and kidney by high-performance liquid chromatography–mass spectrometry. Nodularin is a potent hepatotoxin produced by the algal species Nodularia spumigena. The intensity of algal blooms has increased during the past decades in the Baltic Sea region, thus increasing the risk for intoxications in domestic and wild animals. The authors describe the pathologic findings of cyanobacterial toxicosis in a dog with direct identification of the toxin from organ samples.
Keywords
Hepatic necrosis due to toxins produced by blue-green algae (cyanobacteria) is a well-known cause for acute hepatic failure and death in wild and domestic animals. Although at least 40 species of cyanobacteria, with worldwide distribution, can synthesize a range of hepatotoxins, neurotoxins, and dermatotoxins, the threat of cyanotoxin-contaminated water is often ignored. 3,24
Blooming of blue-green algae, especially the toxigenic species Nodularia spumigena, occurs annually in the Baltic Sea region, presenting a threat for animals exposed to contaminated water. Previously, the identification of blue-green algal toxin was laborious, requiring water samples and the use of experimental animals; 5,6,10,16,25,26 algal toxins have not been analyzed routinely from animal tissues in diagnostic cases. In this report, blue-green algal toxicosis was confirmed by direct toxin analysis from organ samples.
Case History
A 3-year-old female Cairn Terrier weighing 9.6 kg was exposed to sea water containing blue-green algae in the Finnish southwest coastal region of the Baltic Sea. The exact route of exposure is uncertain; the dog was not seen swimming in the sea but may have consumed algal scum or drunk contaminated water. Subsequently, the dog became acutely lethargic with vomiting and inappetence. Initially, it was treated supportively with antiemetics and fluid therapy. Three days after the onset of clinical signs, the dog was admitted to the university hospital because of further clinical deterioration.
Upon physical examination, the dog was lethargic, dehydrated, and icteric. Abnormal hematologic findings included mild nonregenerative anemia (packed cell volume, 32%; reference range, 38%–57%; mean corpuscular volume and hemoglobin within reference ranges) with normal leukocyte count (14.0 × 109/liter; reference range, 5.4–17.4 × 109/liter). Serum biochemistry profile abnormalities included elevated alanine aminotransferase (6211 U/liter; reference range, 18–77 U/liter), alkaline phosphatase (392 U/liter; reference range, 33–215 U/liter), total bilirubin (272.5 μmol/liter; reference range, 1.7–8.5 μmol/liter), blood urea nitrogen (57.7 mmol/liter; reference range, 2.4–8.8 mmol/liter), creatinine (644 μmol/liter; reference range, 57–116 μmol/liter), and phosphate (3.71 mmol/liter; reference range, 0.93–2.25 mmol/liter). The following coagulation parameters were abnormal: activated partial thromboplastin time (23.0 seconds; reference, < 16 seconds), D-dimer (0.7 mg/liter; reference, < 0.3 mg/liter), and thrombin time (30 seconds; reference, < 23 seconds). Serology for Leptospira interrogans serovars was negative.
Intensive intravenous fluid therapy with crystalline and colloid solution was initiated. The dog received supportive treatment of intravenous ampicillin, antiemetic medication (metoclopramide, ranitidine), acetylcysteine, and repeated doses of furosemide, intravenous mannitol, and dopamine. Despite intensive rehydration and diuretic medication, no urination was observed for 24 hours. The general condition of the dog continued to deteriorate, and the owner elected euthanasia 5 days after the onset of illness.
At necropsy, samples of liver, lung, spleen, heart, kidney, stomach, intestine, pancreas, adrenal gland, skeletal muscle, and brain were fixed in 10% neutral buffered formalin and processed routinely for histopathology with a hematoxylin and eosin stain. Liver sections were also stained with Gomori's method for reticulin fibers, periodic acid–Schiff (PAS) with diastase treatment, Perl's Prussian blue for iron, and Fouchet van Gieson for bile. The kidney sections were also reacted with PAS.
Cyanobacterial Toxin Analysis
Based on the clinical history and the pathologic findings, cyanobacterial intoxication was suspected. Frozen samples of liver, kidney, and small intestine were submitted for cyanobacterial toxin analysis. Portions of each tissue were freeze-dried in 2-ml plastic tubes. The dried samples were weighed; glass beads were added to the tubes; and the samples were homogenized with a FastPrep instrument (Savant Instruments, Hicksville, NY; 15 seconds, speed = 6.5 m/s). For toxin extraction, 1 ml of methanol was added to the tubes. The tubes were then shaken, centrifuged, and the supernatant was analyzed (injection volume, 10 μl) with an Agilent 1100 Series LC/MSD Trap System high-performance liquid chromatograph (Agilent Technologies, Palo Alto, CA), which has an XCT Plus model ion trap as a mass detector (ie, liquid chromatography–mass spectrometry [LC-MS]). Positive-mode electrospray ionization was used. The instrument was equipped with a Phenomenex Luna C8 column (150 × 2.0 mm, 5 μm) (Phenomenex, Torrance, CA). The mobile phase was composed of 0.1% formic acid in water (A) and 0.1% formic acid in 2-propanol (B). The gradient run was from 5% B to 65% B over 40 minutes at a flow rate of 0.15 ml · min–1 at 40°C. Ion source nebulizer gas (N2) pressure was 35 psi; desolvation gas flow rate, 8 liters · min–1; and desolvation temperature, 350°C. The capillary voltage was set to 5000 V; the capillary exit, 300 V; the skimmer potential, 66 V; and the trap drive value, 73. Spectra were recorded from 50 to 1200 m/z and a scanning rate of 26 000 m/z · s–1. The MS 2 fragmentation amplitude was 0.75 V. Peaks were identified by liquid chromatography—tandem mass spectrometry (LC-MS/MS) according to characteristic protonated molecular ions [M+H]+ and the product ion spectra from the precursor [M+H]+. Mass data were compared to published data of nodularin from the reference strain N. spumigena AV1 from the Baltic Sea. 9 Purified nodularin from N. spumigena AV1 (a gift from Z. Grzonka, Faculty of Chemistry, University of Gdansk, Poland) was used as a standard for quantification. Nodularin concentration was determined in the freeze-dried specimens.
Results
On gross examination, the carcass was icteric with approximately 1.4 liters of serous fluid in the abdominal cavity; abdominal viscera had marked subserosal edema. The liver was brownish red, swollen, and fragile with a prominent lobular pattern and miliary dark areas (Fig. 1). Bile flow to the duodenum could be induced by manual pressure of the gall bladder. The kidneys were swollen and pale with a mildly prominent corticomedullary junction. Gross lesions were not observed in other organs.
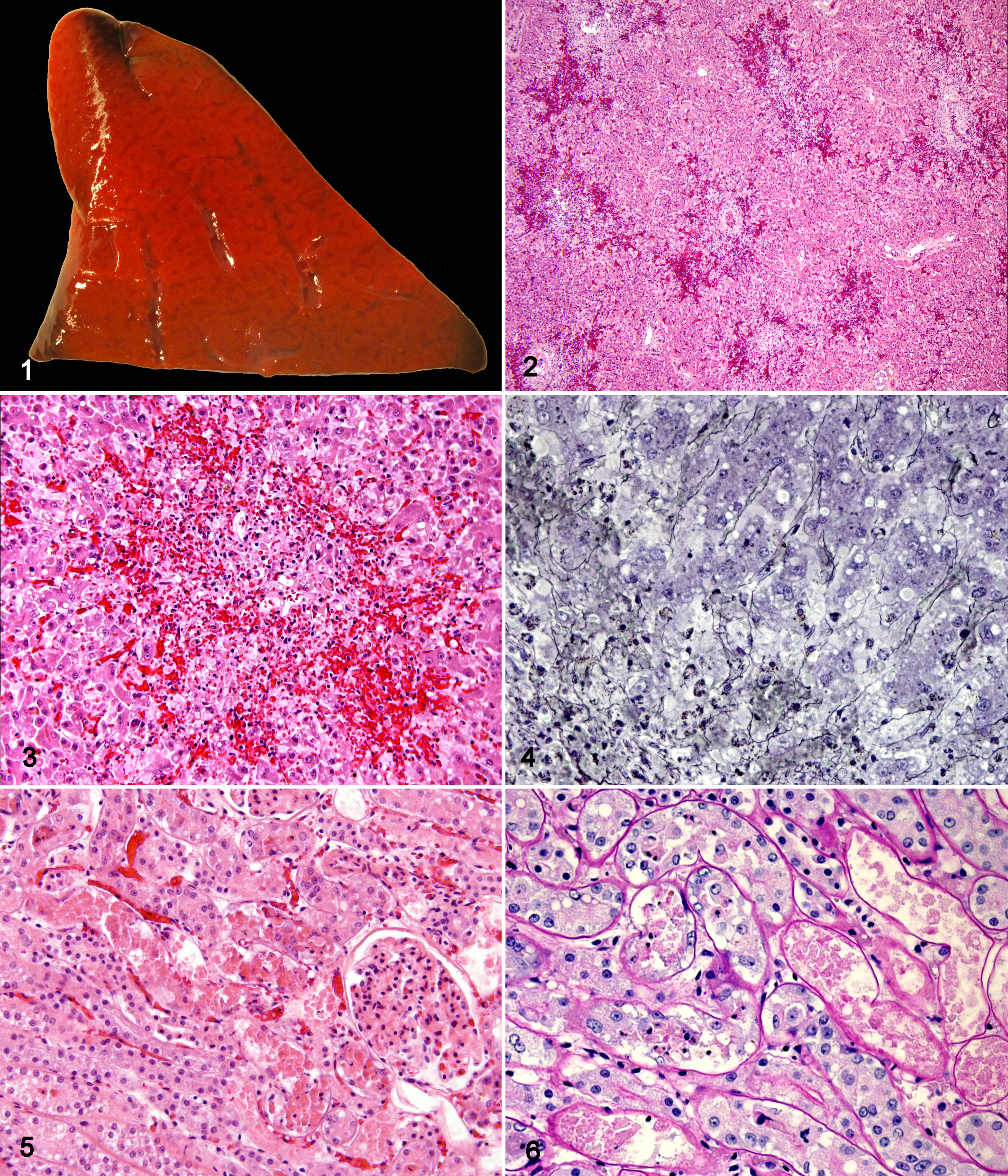
Liver; dog. The liver is brownish red with a prominent lobular pattern and miliary dark foci.
Histologically, acute lytic centrilobular hepatocellular necrosis associated with central–central bridging between some lobules was seen (Fig. 2). Hepatocytes were lost from lobular centers where only blood and cellular debris remained (Fig. 3). The loss of hepatic parenchyma with stromal collapse was accentuated by silver impregnation of reticulin fibers (Fig. 4). In the periphery of the necrotic areas, bile distended some canaliculi, and scattered macrophages contained bile pigment, hemosiderin, and amorphous PAS-positive material, interpreted as cellular debris. Surviving hepatocytes around the necrotic areas were dissociated and rounded with cytoplasmic vacuoles that were PAS-negative, consistent with fatty change or hydropic degeneration. Scattered hepatocytes had a large nucleus with prominent nucleoli and increased mitotic activity. Some sinusoids contained fibrin thrombi.
The renal cortex had radiating streaks of acute tubular necrosis. Affected tubules contained intraluminal granular and hyaline material and sloughed epithelial cells (Fig. 5). The necrosis extended multifocally into collecting ducts. Regenerative tubular epithelial cells were flattened with enlarged hyperchromatic or vesicular nuclei. The tubular basement membranes were intact, consistent with toxic tubulonephrosis (Fig. 6). The heart had scattered necrotic myocardial fibers. Other organs were without significant histologic lesions.
The dry weights of the liver, kidney, and intestine specimens for LC-MS were 78.4, 88.5, and 89.9 mg, respectively. A protonated molecular ion of nodularin (m/z 825) was detected in all samples. The product ion spectra were nearly identical to the spectrum of the reference nodularin (Fig. 7). Nodularin concentrations (dry weight) in liver, kidney, and intestine were 490, 500, and 5 μg/kg, respectively. No metabolic products of nodularin or microcystins were detected.
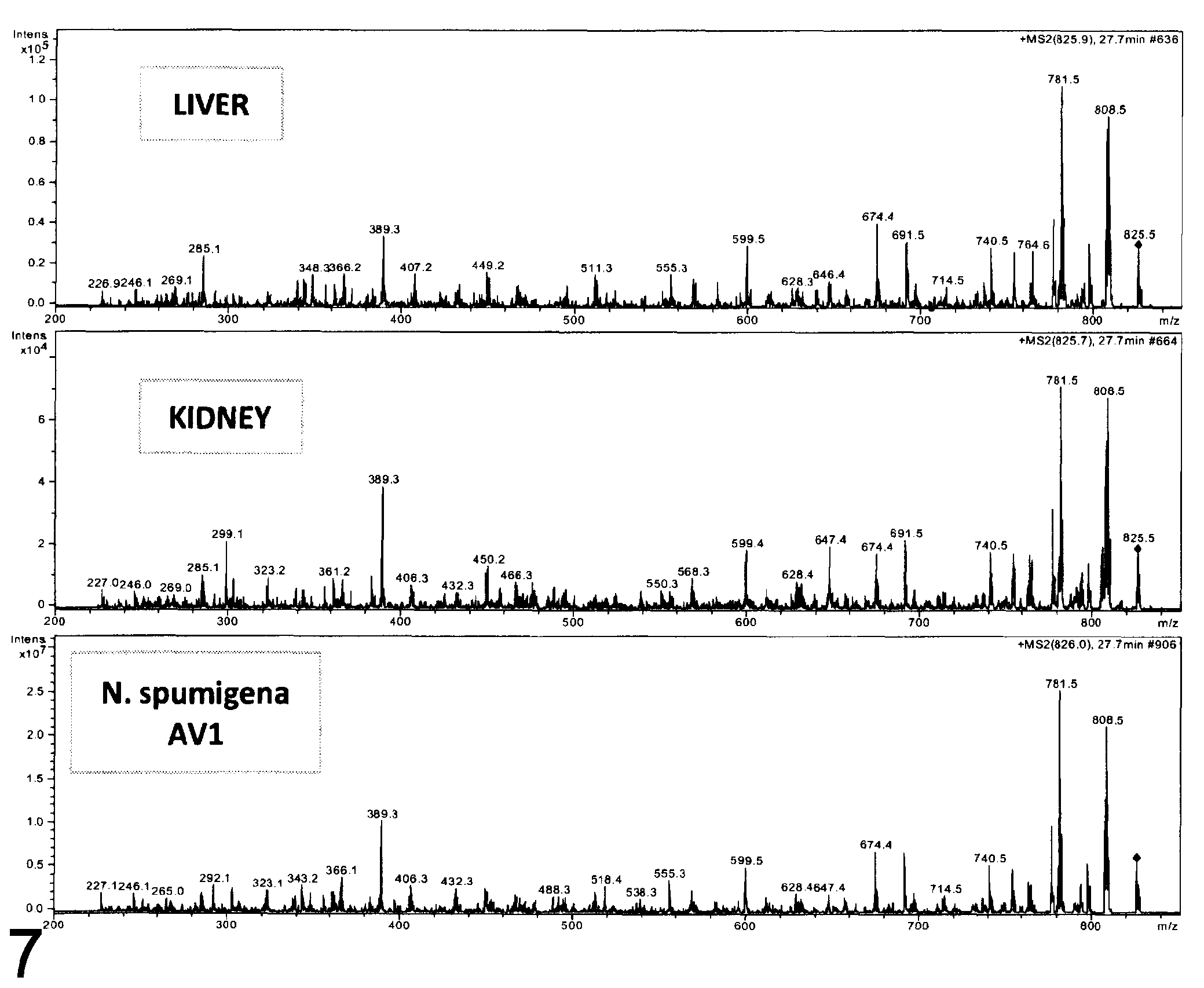
Product ion spectra of protonated molecular ion of nodularin (m/z 825) from liver, kidney, and the reference Nodularia spumigena AV1 are almost identical.
Discussion
Nodularin was confirmed as the cause of hepatic injury in this dog. Nodularin is the main toxin produced by the cyanobacterium N. spumigena. This species is found mainly in brackish water and is the main toxin-producing species in the Baltic Sea area. 14,21 Large mass occurrences (blooms) of cyanobacteria modulated by environmental factors are an annual late summer event in the Baltic Sea. The toxicity of algal blooms is also influenced by local conditions; 13,14 toxin production by N. spumigena tends to be highest under conditions that also favor its growth. 13 The intensity of blooms has increased considerably during recent decades in the Baltic Sea region and the Gulf of Finland, 8,23 creating an accessible source of environmental toxin for domestic animals. However, there are few descriptions of the lesions in natural nodularin intoxications in domestic animals, mainly livestock and dogs. 6,10,15,25
Nodularin is a cyclic pentapeptide toxin that is released when the cyanobacteria disintegrate in either the water or the alimentary tract after ingestion. 21 The chemical structure and mechanism of action of nodularin resemble those of another cyanobacterial hepatotoxin, microcystin, produced by several cyanobacterial genera, including Microcystis aeruginosa. 3,24 Nodularin is absorbed from the ileum by bile acid carriers. The toxin enters the liver with portal blood flow and is transported into hepatocytes via bile acid carriers. Nodularin inhibits serine/threonine protein phosphatases 1 and 2A in rat liver epithelial cells. 11 This inhibition leads to hyperphosphorylation of cytoskeletal proteins in hepatocytes. A rapid loss of hepatic architecture and accumulation of blood in the sinusoids follows. Death is usually attributed to hypovolemic shock with intrahepatic hemorrhage or hepatic insufficiency.
Nodularin is considered extremely toxic, 3 with an intraperitoneal median lethal dose of 50 to 70 μg/kg in mice. 7,20 Although the median lethal dose has not been determined for nodularin in dogs, based on the hepatic injury in this dog, the detected nodularin concentrations (490 μg/kg in the liver and 500 μg/kg in the kidney, dry weight) were considered toxic, especially when considering that the analysis was at least 5 days after exposure. Cattle, sheep, dogs, pigs, and waterfowl are susceptible to toxicosis due to ingestion of wet algae cells. Laboratory animals are more resistant to oral administration and require higher doses to be affected; however, they are highly susceptible to parenteral administration of cyanotoxins. 1 The nodularin concentration in the Baltic Sea water and blooms varies from < 100 to 2400 μg/g, dry weight, 21 indicating a high toxic potential in small water volumes. The highest reported concentration of nodularin was 18 000 μg/g, dry weight, in a cyanobacterial bloom. 12 Importantly, growth and accumulation of algae can result in scum formation and concentration of the toxin. 4
In conclusion, domestic and wild animals can be exposed to high concentrations of cyanobacterial toxins, and the requisite water volume for acute nodularin intoxication can easily be acquired. In dogs, toxicosis is usually a result of drinking contaminated water or accidental ingestion during swimming. 5,10,19,26 The algal material can also adhere to the fur and be ingested when the animal licks its coat. 6 Water containing the algal material might be more palatable to animals. 4,25 In this case, no swimming was observed, but ingestion of algal scum or drinking of contaminated water or other material at the beach could not be excluded. Small breeds, such as the Cairn Terrier in our case, may be more susceptible to nodularin toxicosis because the toxic dose can be more easily acquired.
The clinical findings in this dog were mainly attributed to hepatic injury. Nevertheless, an important clinical sign, as well as a major reason for euthanasia was anuria, which correlated histologically with renal tubular necrosis. The lack of renal interstitial reaction or basement membrane damage is consistent with toxic tubular insult. Tubulonephrosis has been described in canine nodularin toxicosis, but the cause for the lesion was not elucidated. 6 Although the liver is considered the main target organ of nodularin because of the requirement of a bile acid carrier for intracellular uptake, 3 Zhang et al. demonstrated, by a radioisotope study, that nodularin is also distributed to the kidneys in mice. 27 Renal tubular epithelial cells have a bile transporter system like that of intestinal cells; 22 thus, it is likely that transport of nodularin also occurs in the kidney. In our case, renal nodularin concentration was comparable with that of the liver. These findings suggest that kidneys are also primarily affected in canine nodularin intoxication. Renal perfusion is decreased in microcystin toxicosis. 2 Based on its similar mechanism of action, nodularin toxicosis may also cause decreased renal perfusion. The myocardial lesions and subserosal edema in this dog also suggest the possibility of a prerenal component in the renal failure.
In this case, identification of cyanobacterial toxin from organ samples confirmed the diagnosis of nodularin toxicosis. Toxin detection in animal tissues by LC-MS is a sensitive alternative to former methods that required water samples. 17,18 In this study, liver and kidney were the best samples for toxin detection at 5 days postexposure. Intestinal toxin concentration was almost undetectable at 5 days, but gastric or intestinal content might have been a useful sample earlier in the toxicosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.