
Abstract
The objective of this study was to describe chronological changes in infection status and enteric lesions of sheep naturally exposed to Mycobacterium avium subspecies paratubercuolosis. Samples of terminal ileum (TI) and mesenteric lymph node (MLN) were collected from 77 Merino sheep via surgical biopsy at 12, 18, and 24 months of age and necropsy at 36 months of age. Infection status at each sampling period was determined by fecal, TI, and MLN culture. Quantitative grading schemes were used to gauge the severity of granulomatous inflammation and degree of mycobacterial colonization affecting TI and MLN sections. Incidences of infection and disease were steady throughout the study; 46 of the 77 (59.7%) sheep became infected, and 30 of the 77 (39.0%) developed Johne’s disease. Infection was first detected after 18 months of age in many sheep, and age when infection was first detected was not associated with clinical outcome. Culture of MLN detected 44 of the 46 (95.6%) infected sheep and initial lesions always involved MLN. Sheep typically developed lesions within 6–12 months following detection of infection by culture. The severity of enteritis and mycobacterial colonization progressed at variable rates among sheep. Severe multibacillary enteritis never regressed, and affected sheep expressed clinical signs within the following 12 months. Lymphocyte-rich paucibacillary enteritis was observed in 3 sheep, causing clinical signs in one and progressing to severe multibacillary enteritis in another. Six of the 46 (8.7%) biopsy-culture–positive sheep later had negative cultures at necropsy, suggesting recovery from infection. Further study is needed to identify factors associated with clearance of infection or progression of disease.
Ovine Johne’s disease (OJD) is caused by Mycobacterium avium subspecies paratuberculosis (MAP). Over time, infected sheep develop granulomatous enteritis and mesenteric lymphadenitis, which can eventually result in emaciation and death. In high-prevalence areas, there can be substantial economic loss due to the high mortality rates attributable to OJD. 5
Although OJD has been studied for decades, many details of its pathogenesis remain speculative. Sheep are believed to become infected through fecal–oral infection, typically as neonates. 8 Clinically evident disease develops after a variable incubation period, usually lasting 2–4 years. The nature of the intestinal inflammation and the degree of mycobacterial colonization vary among MAP-infected sheep. 7,9,20,21 Parallels have been made between the spectrum of OJD lesions and those seen in leprosy, 9,21 leading to the use of the terms paucibacillary or tuberculoid to describe lesions that are presumably associated with strong cell-mediated immunity, comprised of lymphocytes and small collections of epithelioid macrophages and low numbers of mycobacteria, and multibacillary or lepromatous to describe lesions that are presumably associated with weak cell-mediated immunity, containing extensive granulomatous infiltrate and large numbers of mycobacteria. 1 Both forms have been associated with clinical signs. 7,9 Because histopathological studies to date have examined tissues collected at necropsy, it is unknown which, if any, of these lesions represent irreversible end-stage lesions. Furthermore, it is unknown whether certain lesions reflect a latent or initial state of OJD.
The objective of the present study, the only large cohort study to evaluate repeated surgical biopsies, was to chronologically describe the occurrence of infection and the progression of histopathological lesions affecting terminal ileum and caudal mesenteric lymph node in sheep naturally exposed to MAP.
Methods
Animals
Seventy-seven Merino lambs from a heavily MAP-infected flock were enrolled in the study. These sheep were born in September 2000 and were 9–10 months old when enrolled in the study. As age of sheep from a common lambing group spans several weeks, age to the nearest month is reported herein. They were excluded from an OJD vaccination program that began on the farm in September 2000. Experimental design was informed by prior research on this farm, where approximately 10% of unvaccinated 3-year-old sheep were positive in the agar gel immunodiffusion test (AGID), mortalities due to OJD occurred in this age class, and about 20% of sheep had infection detectable by necropsy and culture of intestinal tissues at 6 months of age. The experimental lambs were grazed with 150 three-year-old ewes, about 10% of which were AGID positive, suggesting that lambs were likely to receive a high level of exposure to MAP. The sheep were grazed under normal farm conditions on unimproved pasture, except that ewes were not mated. They received no supplementary feeding during the trial. The sheep were examined closely at least weekly by the farmer, and condition scores were recorded at the time of each biopsy examination to detect the clinical signs of OJD.
Study sheep were examined using a range of tests, including clinical examination, fecal culture, and biopsy of terminal ileum (TI) and mesenteric lymph node (MLN), performed at regular intervals (12, 18, and 24 months of age). TI and MLNs associated with the TI and ileocecal valve were biopsied for histopathology and tissue culture. These tissues were selected on the basis of being the sites that most consistently harbor lesions of OJD in infected sheep 16 and the ileum being the site that presents the most advanced intestinal lesions. 4,9,21 During clinical examination, a sheep was designated as having clinical signs consistent with OJD if it had a body condition score noticeably lower than the majority of flock mates or if it was weak and depressed. Such sheep were humanely euthanatized with intravenous barbiturate when recognized.
All research was undertaken with approval of the Animal Care and Ethics Committee, NSW Department of Primary Industries, Elizabeth Macarthur Agricultural Institute.
Biopsy of Intestine and Lymph Node
Laparotomy and biopsy of TI and MLN associated with the ileocecal valve and TI were performed on all study sheep at 12 months of age, a subset of 20 sheep at 18 months of age (consisting of all sheep that were classified as infected according to previous test results), and the 73 sheep surviving at 24 months of age. The flank laparotomy and surgical procedure were described previously in detail. 17 A 1-cm3 portion of tissue was excised from an MLN associated with the TI or ileocecal valve. A 2-mm-thick transverse section was cut from the excised lymph node and placed in 10% neutral buffered formalin. The remaining lymph node was placed in a sterile container for culture and held at 4°C. A V-shaped piece of ileum was resected 5–10 cm from the ileocecal valve, with its apex at the mesenteric border. The resulting biopsy was 1–1.5 cm long at its antimesenteric margin. A 2-mm-wide portion of tissue was circumferentially cut from 1 side of the ileum sample and placed in 10% neutral buffered formalin. The remaining ileum sample was placed in a sterile container for culture and held at 4°C. Although ileum that had been biopsied previously often had a mild focal serosal fibrosis or rarely minor mesenteric adhesions, there was little interference with subsequent surgical procedures and there was no difficulty avoiding a previous biopsy site while taking another biopsy from the same region of ileum. Postsurgical complications were limited to a few cases of mild lameness that resolved without treatment. 17
Necropsy
At any point during the study, sheep observed to have clinical signs consistent with OJD (as defined above) were euthanatized and necropsied immediately. Sheep that died in the paddock were not available for necropsy (because of the presence of advanced postmortem decomposition when found). At 36 months of age, all surviving study sheep were humanely euthanatized with intravenous barbiturate and were necropsied immediately. Sheep were examined for gross lesions suggestive of OJD (intestinal mucosal thickening, enlarged MLN, and cording of serosal lymphatics), but this did not influence sample collection. During necropsy of all sheep, portions of TI (a pool of 3 segments about 100, 200, and 300 mm proximal to the ileocecal valve) and MLN (a pool of segments from 3 lymph nodes, including an ileocecal valve and caudal jejunal nodes) were collected into sterile containers for culture. Samples of tissues adjacent to these sites, resembling biopsies, were taken and placed in 10% neutral buffered formalin for histopathology.
Culture of MAP
Clinical samples were held at 40°C and processed within 48 hours or frozen at –800°C for up to 3 months until processed. Fecal samples were cultured as previously described. 30 Tissues from biopsy and necropsy were processed using a standard technique, 30 with addition of a centrifugation step. 26 BACTEC vials were incubated for 12 weeks, and growth of MAP was confirmed by IS900 polymerase chain reaction and restriction enzyme analysis.
Histopathologic Examination
Tissues were processed routinely for histopathology, sectioned at 5 μm, and stained with hematoxylin and eosin and a Ziehl-Neelsen acid fast stain.
For this analysis, histopathologic examination of all sections was completed by 1 pathologist (MMD). Sections were examined for the presence of granulomatous inflammation and for acid fast bacilli (AFB). Tissues were each graded for severity of granulomatous inflammation. When more than 1 section of a tissue was available for evaluation (ie, multiple samples collected from necropsied sheep, or when biopsies were of sufficient size to make >1 section), the section with the greatest degree of inflammatory infiltrate was graded; however, there were rarely appreciable differences in severity between sections, and there was never an appreciable difference in the type of inflammatory infiltrate. Points were assigned to each tissue according to the quantity and the microanatomical location of epithelioid macrophages (Table 1 ). The levels of leukocyte location were selected to reflect the range of lesion severity observed in experimental and natural OJD. 9,15,21 For each tissue, tallied points comprised the lesion grade that was used to ascribe a level of lesion severity. A grade of 0 corresponded to severity of none, grades 2–3 corresponded to mild, grade 4 corresponded to moderate, and grades 5–7 corresponded to severe. An AFB grade was assigned to each histopathologically evaluated tissue based on the subjective quantities of AFB identified (Table 2 ). AFB grades of 0–2 were considered paucibacillary, whereas AFB grades of 3–4 were considered multibacillary. This is similar to the method of Clarke and Little, 9 who categorized lesions containing on average 10 or fewer AFB per macrophage as paucibacillary and those containing more than 10 AFB per macrophage as multibacillary.
Lesion Grading System for Severity of Granulomatous Inflammation in Terminal Ileum and Mesenteric Lymph Node Sections
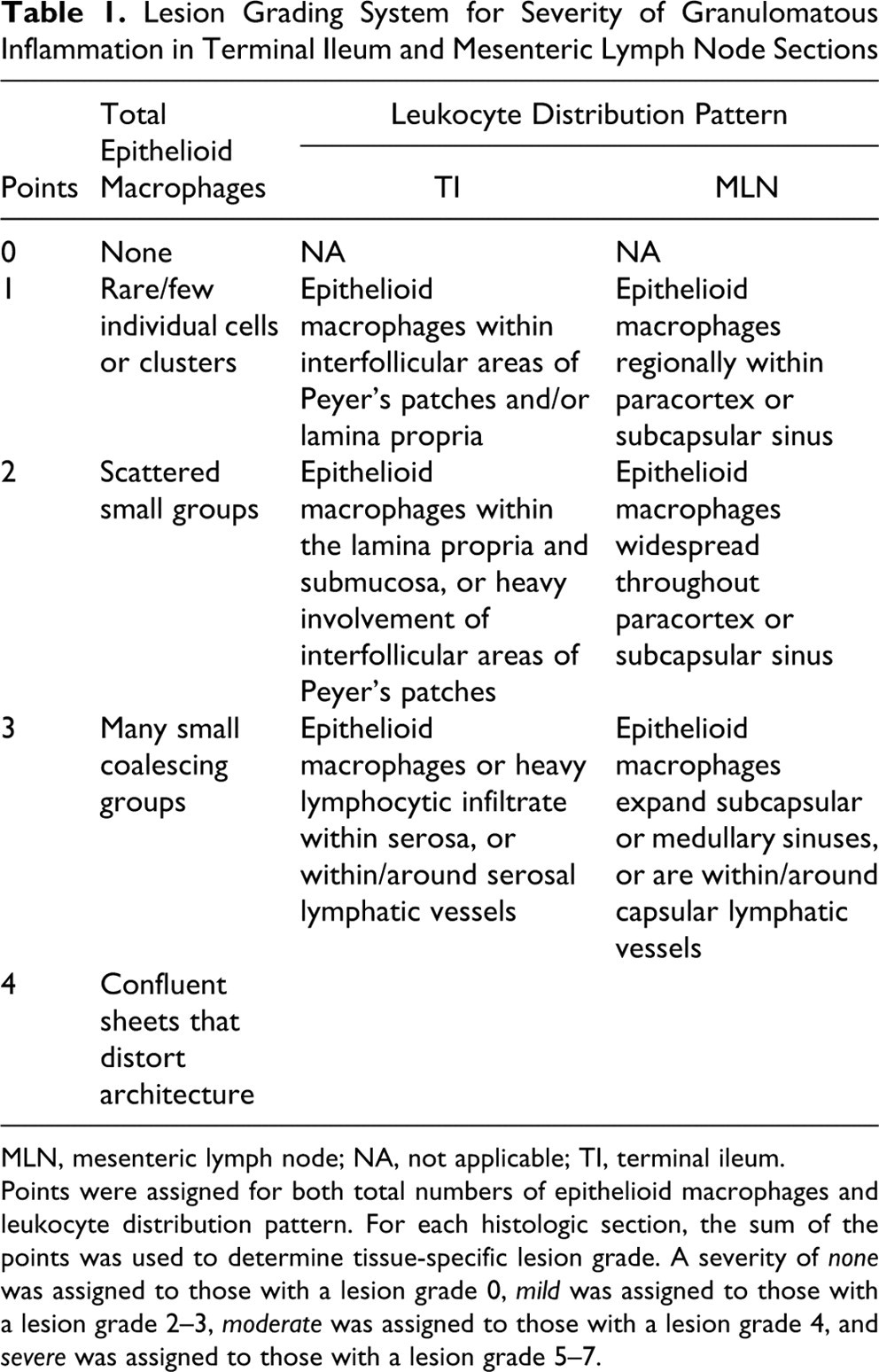
MLN, mesenteric lymph node; NA, not applicable; TI, terminal ileum.
Points were assigned for both total numbers of epithelioid macrophages and leukocyte distribution pattern. For each histologic section, the sum of the points was used to determine tissue-specific lesion grade. A severity of none was assigned to those with a lesion grade 0, mild was assigned to those with a lesion grade 2–3, moderate was assigned to those with a lesion grade 4, and severe was assigned to those with a lesion grade 5–7.
Acid-Fast Bacilli (AFB) Grading System for Terminal Ileum and Mesenteric Lymph Node Sections
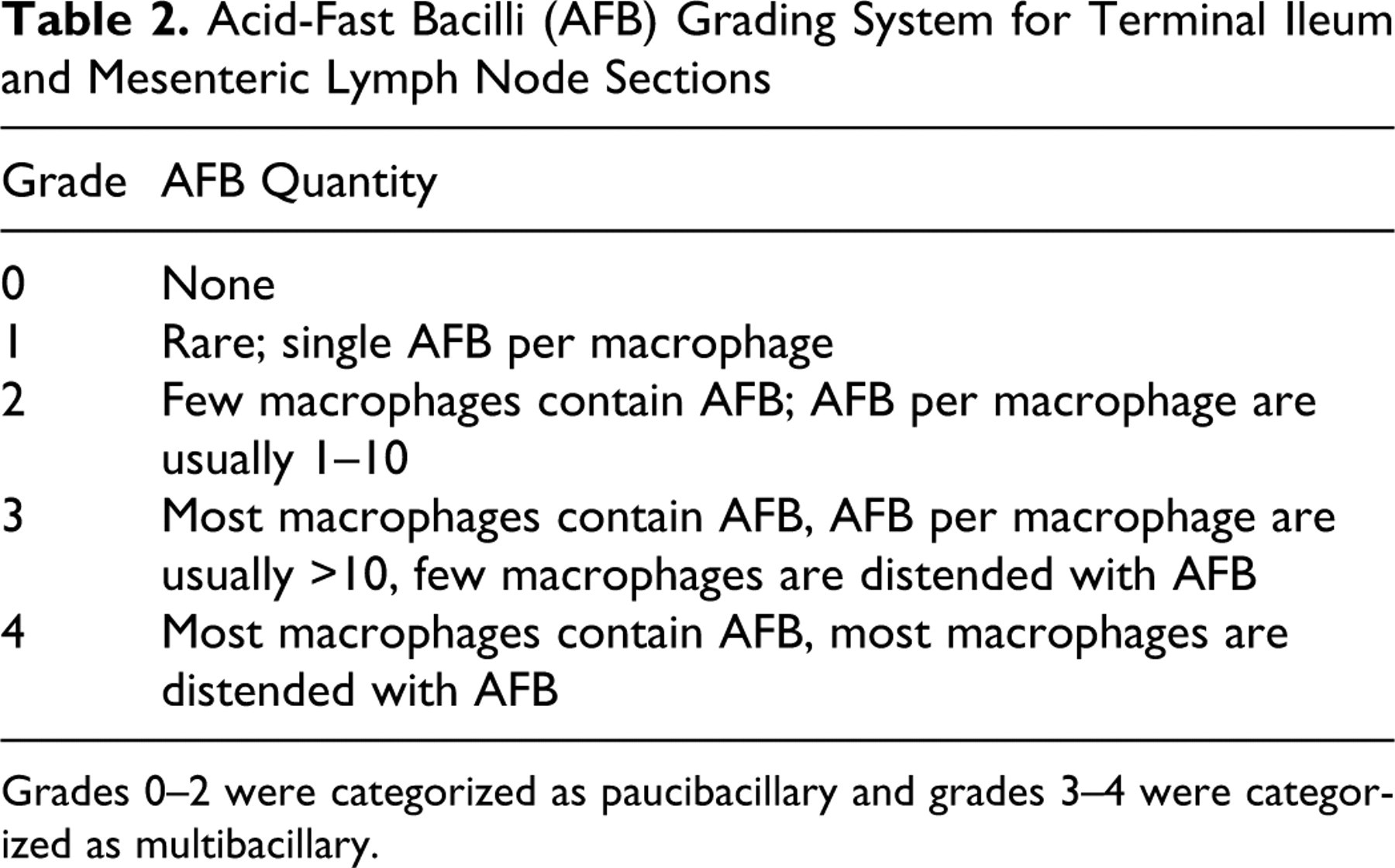
Grades 0–2 were categorized as paucibacillary and grades 3–4 were categorized as multibacillary.
Small nests of macrophages that contained granular yellow-green refractile pigment, colorless crystals, or granular brown-black pigment (consistent with a foreign body reaction to exogenous material) were considered nonindicative of MAP infection and were excluded from the grading system.
Classification of Sheep
A sheep was classified as infected if, at any time during the study, MAP was cultured from tissue or feces. Conversely, a sheep was classified as not infected if all tissue and fecal cultures performed throughout the study failed to grow MAP and microscopic examination of tissues failed to reveal inflammation of grade ≥1 AFB.
An infected sheep was further subclassified as having clinical infection if clinical signs were noted or as having subclinical infection if clinical signs were not evident. Findings were considered suggestive of recovery from infection if a sheep had been previously categorized as infected but necropsy failed to identify lesions consistent with OJD and produce positive tissue cultures.
Statistical Analysis
The proportion of sheep that developed clinical infection was compared between groups of sheep first recognized to be infected at 12, 18, and 24 months of age using a Pearson chi-square. A P value of <.05 was considered to be statistically significant.
Results
The study population consisted of 77 sheep (30 males, 33 females, 14 sex not recorded). Forty-six of the 77 (59.7%) sheep were characterized as being infected at some point during the study. New infections were recognized at each sampling period (Table 3 ), and both prevalence and incidence rate of infection increased throughout the study period.
Status of the Study Population at Four Sampling Periods, in Terms of Microbiological Evidence of Mycobacterium avium Subspecies Paratuberculosis (MAP) Infection and Histopathological Lesions of Ovine Johne’s Disease (OJD)
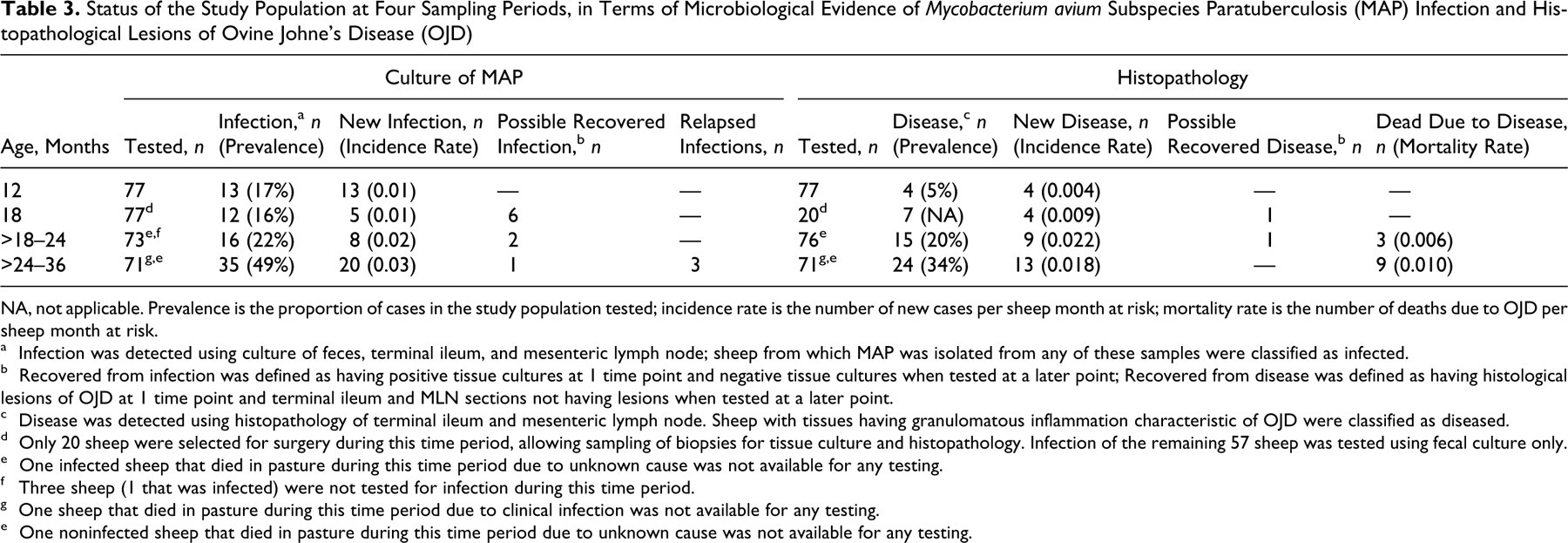
NA, not applicable. Prevalence is the proportion of cases in the study population tested; incidence rate is the number of new cases per sheep month at risk; mortality rate is the number of deaths due to OJD per sheep month at risk.
a Infection was detected using culture of feces, terminal ileum, and mesenteric lymph node; sheep from which MAP was isolated from any of these samples were classified as infected.
b Recovered from infection was defined as having positive tissue cultures at 1 time point and negative tissue cultures when tested at a later point; Recovered from disease was defined as having histological lesions of OJD at 1 time point and terminal ileum and MLN sections not having lesions when tested at a later point.
c Disease was detected using histopathology of terminal ileum and mesenteric lymph node. Sheep with tissues having granulomatous inflammation characteristic of OJD were classified as diseased.
d Only 20 sheep were selected for surgery during this time period, allowing sampling of biopsies for tissue culture and histopathology. Infection of the remaining 57 sheep was tested using fecal culture only.
e One infected sheep that died in pasture during this time period due to unknown cause was not available for any testing.
f Three sheep (1 that was infected) were not tested for infection during this time period.
g One sheep that died in pasture during this time period due to clinical infection was not available for any testing.
e One noninfected sheep that died in pasture during this time period due to unknown cause was not available for any testing.
Of the 46 infected sheep, 30 (65.2%) developed characteristic histopathological lesions (grade ≥1). Histological lesions of OJD manifested within 6–12 months of infection being detected by culture in 29 of the 46 (58.7%) infected sheep and were detected as early as 12 months of age (Tables 4 and 5 ). The only sheep that had developed lesions >12 months after infection was detected by culture (sheep No. 21) did not have detectable infection at 18 and 24 months of age and infection was again detected at 36 months of age. Of the 16 infected sheep that did not develop lesions, 5 had absence of detectable infection in the final sampling period, and 11 were first detected as infected in the final sampling period, precluding follow-up for development of enteric lesions.
Progression of Granulomatous Enteritis in Infected Sheep That Developed Lesions of Ovine Johne’s Disease (OJD)
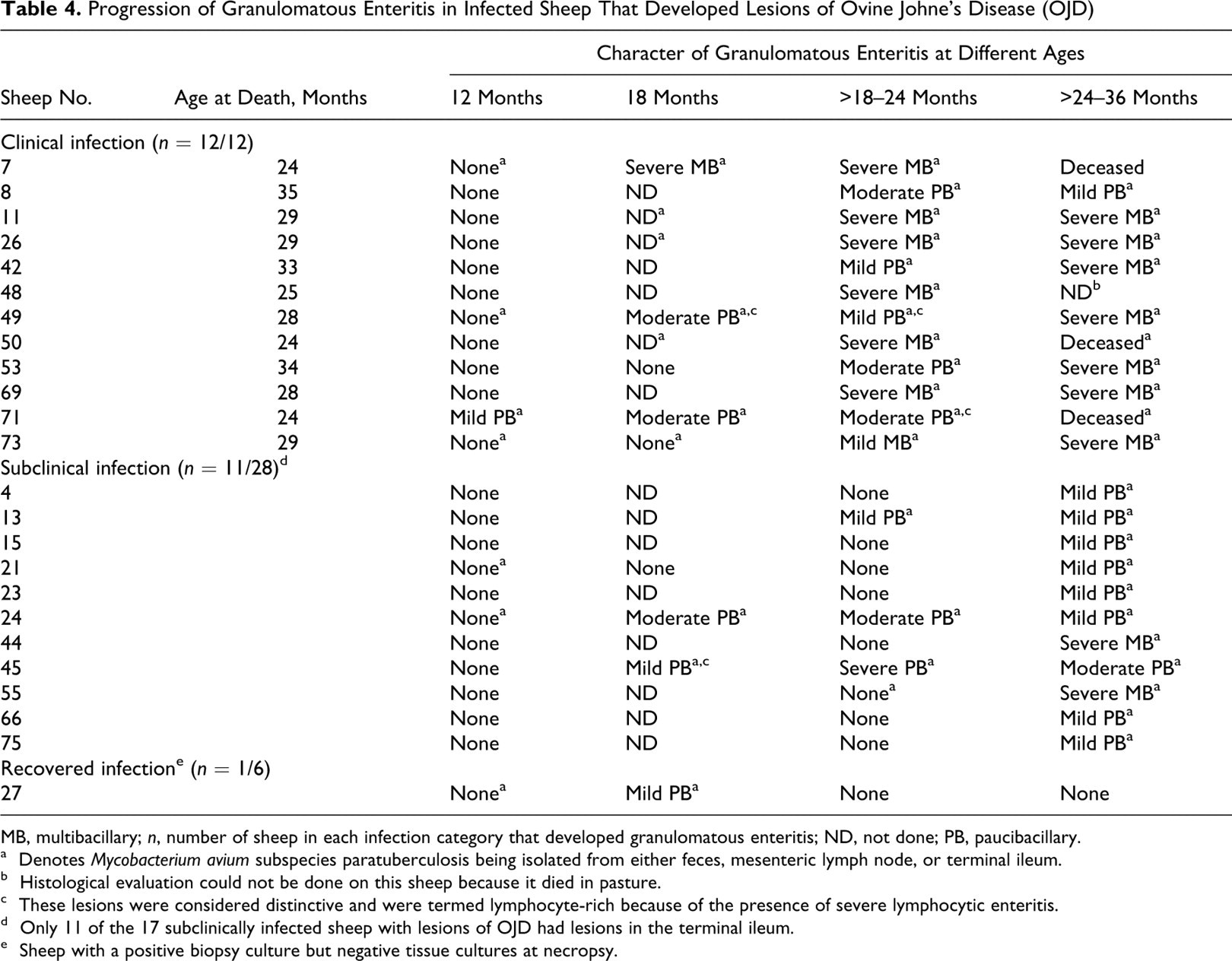
MB, multibacillary; n, number of sheep in each infection category that developed granulomatous enteritis; ND, not done; PB, paucibacillary.
a Denotes Mycobacterium avium subspecies paratuberculosis being isolated from either feces, mesenteric lymph node, or terminal ileum.
b Histological evaluation could not be done on this sheep because it died in pasture.
c These lesions were considered distinctive and were termed lymphocyte-rich because of the presence of severe lymphocytic enteritis.
d Only 11 of the 17 subclinically infected sheep with lesions of OJD had lesions in the terminal ileum.
e Sheep with a positive biopsy culture but negative tissue cultures at necropsy.
Progression of Granulomatous Mesenteric Lymphadenitis in Infected Sheep That Developed Lesions of Ovine Johne’s Disease (OJD)
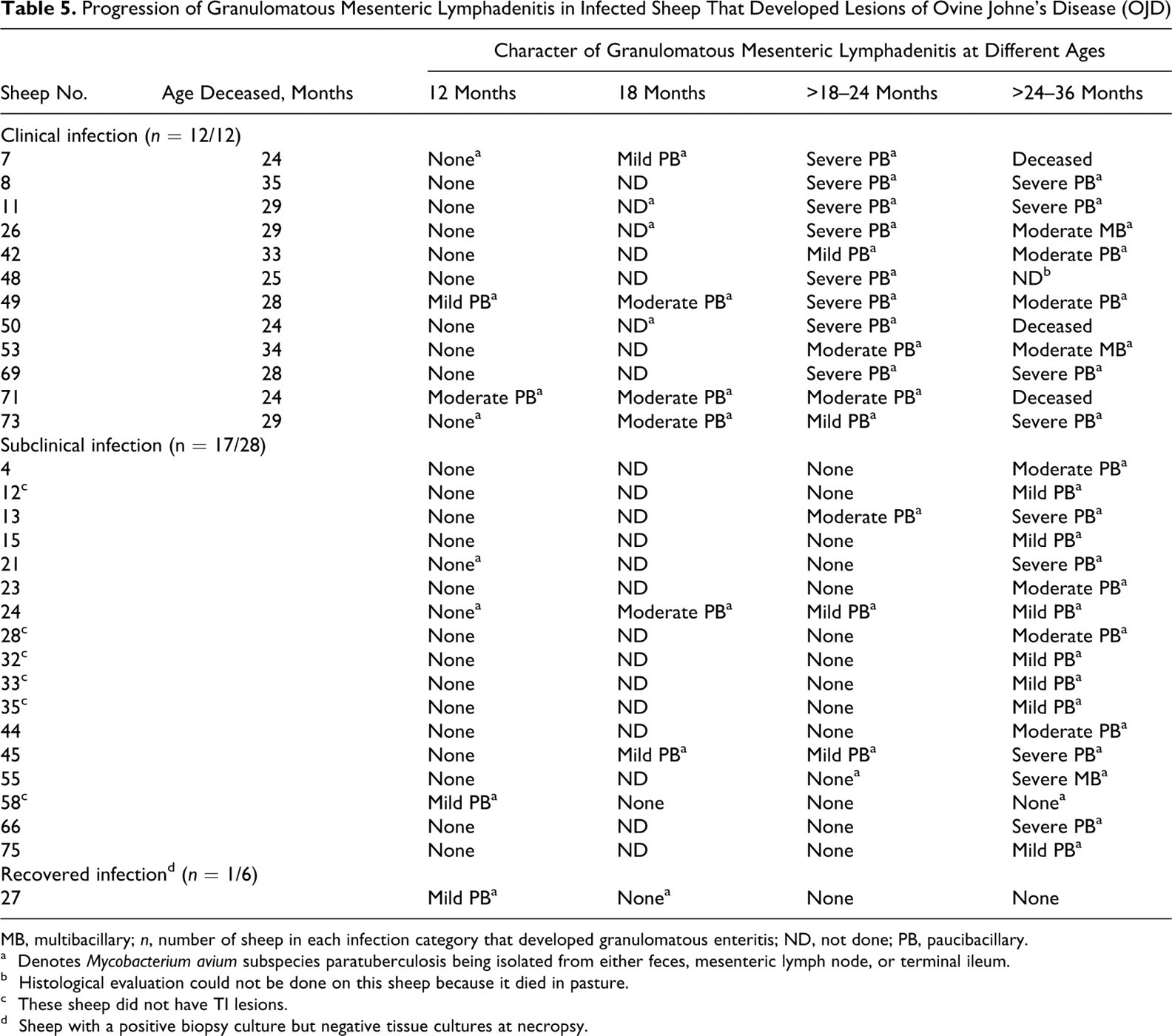
MB, multibacillary; n, number of sheep in each infection category that developed granulomatous enteritis; ND, not done; PB, paucibacillary.
a Denotes Mycobacterium avium subspecies paratuberculosis being isolated from either feces, mesenteric lymph node, or terminal ileum.
b Histological evaluation could not be done on this sheep because it died in pasture.
c These sheep did not have TI lesions.
d Sheep with a positive biopsy culture but negative tissue cultures at necropsy.
In infected sheep, MAP was isolated from MLN more frequently than TI, and in those sheep that developed lesions, these were often detected in MLN prior to TI. Infection was detected by isolating MAP at some point during the study from MLN in 44 of the 46 (95.6%) sheep and from TI in 30 of the 46 (65.2%) sheep. No additional sheep were detected using fecal culture, which detected 12 of the 12 (100%) sheep with clinical infection, 10 of the 28 (35.7%) with subclinical infection, and 1 of the 6 (16.6) sheep classified as having recovered infection. Lesions were initially detected in both MLN and TI in 21 of the 30 (70.0%) sheep, whereas lesions were initially limited to MLN in 9 of the 30 (30.0%) and were never limited to TI. The severity of the final lesions affecting MLN and TI were equal in 10 of the 30 (33.3%) and similar (within 1 level of severity) in 15 of the 30 (50.0%) sheep with OJD. At no point in the study did any sheep have OJD lesions in a tissue that MAP was not isolated from.
The degree of mycobacterial colonization of enteric lesions tended to progress over time but varied by tissue and by lesion severity. Sixteen of the 17 (94.1%) TI biopsies that had severe granulomatous inflammation were multibacillary, whereas 23 of the 24 (95.8%) TI biopsies that had mild or moderate inflammation were paucibacillary. In contrast, 46 of the 49 (93.9%) MLN biopsies with lesions were paucibacillary regardless of lesion severity (Fig. 1). The 3 sheep with multibacillary MLN lesions had concurrent severe multibacillary TI lesions. A progression from paucibacillary to multibacillary was observed in the TI lesions of 3 sheep (sheep Nos. 42, 49, and 53) and MLN lesions of 2 sheep (sheep Nos. 26 and 53), but no lesions in either MLN or TI changed from multibacillary to paucibacillary over time.
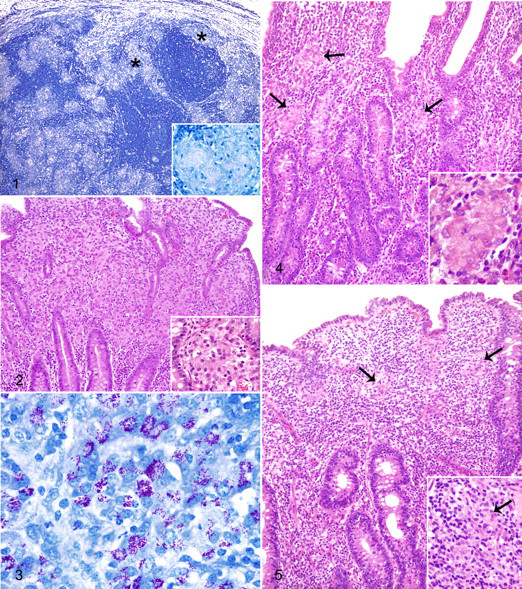
Once enteric lesions had manifested, they progressed at a variable rate. Eight of 30 (26.7%) sheep with OJD lesions rapidly developed severe multibacillary enteritis (Figs. 2 and 3 , referred to as type 3b 21 or multibacillary 9 lesions by others) within 6–12 months of infection being detected microbiologically (Table 4; sheep Nos. 7, 11, 26, 44, 48, 50, 55, and 69). In contrast, 4 of the 30 (13.3%) sheep with OJD lesions developed slowly progressing disease where enteritis persisted and fluctuated in severity over a period of 18–24 months following detection of infection (Table 4; sheep Nos. 24, 45, 49, and 71).
Clinical signs of OJD were first apparent around 24 months of age, following the development and persistence of severe enteric lesions. One sheep died of OJD and 11 were euthanatized because of clinical signs of OJD, reflecting a case fatality rate of 12 of 30 (40.0%). The proportion of sheep that developed clinical infection was not significantly different among groups that were first recognized as infected at 12, 18, or 24 months of age (P = .29). Ten of the 12 (83.3%) sheep with clinical infection had severe multibacillary enteritis; these sheep developed clinical signs or died from OJD within 12 months of severe multibacillary enteritis being recognized. For all sheep that developed clinical infection, during the final sampling period fecal culture and tissue culture were positive, and lesions were present in both TI and MLN, reflecting the diffuse nature of lesions at this stage of disease.
Sheep categorized as having subclinical infection typically reflected earlier stages of disease, where infection was more recent, and lesions were less prevalent and severe in sheep with subclinical infection compared with sheep with clinical infection. Twenty of the 28 (71.4%) sheep that had subclinical infection had been detected as infected in the final sampling period. Of subclinically infected sheep that had lesions in the final sampling period, most lesions (9/11 [81.8%] TI and 11/17 [64.7%] MLN) were mild or moderate in severity and most (9/11 [81.8%] TI and 15/17 [88.2%] MLN) were paucibacillary (Fig. 4 , TI lesions referred to as type 1, type 2, or type 3a by another study 21 ). For 3 sheep that were subclinically infected at 12 months of age, infection was not detected at 18 months of age but was identified again at a later date (sheep Nos. 21, 58, and 65). One of these sheep (sheep No. 58) had mild paucibacillary lymphadenitis, which resolved for the remainder of the study, and 1 (sheep No. 65) never developed lesions of OJD.
Three of the 4 sheep with non–rapidly progressing infection (sheep Nos. 45, 49, and 71) had distinctive lymphocyte-rich paucibacillary TI lesions at some point during the study (referred to by other investigators as type 3c 21 ; paucibacillary, tuberculoid 9 ; group II 24 ; or tuberculoid 5 lesions; Fig. 5.). In these lesions, individual or small groups of epithelioid macrophages were obscured by a dense lymphocytic infiltrate of the lamina propria that extended into the submucosa and sometimes the muscularis and serosa. Sheep 71 was euthanatized because of clinical signs associated with the lymphocyte-rich paucibacillary enteritis. In sheep No. 49, the lymphocyte-rich paucibacillary enteritis progressed over 12 months to severe multibacillary enteritis, apparent when necropsied at 28 months of age following expression of clinical signs. Sheep No. 45 maintained subclinical infection for the entire study while having progressed from lymphocyte-rich paucibacillary enteritis at 18 months of age to moderate paucibacillary enteritis when necropsied at 36 months of age.
Six sheep had findings suggestive of recovered infection. All were initially identified as infected by positive tissue culture, which occurred at 12 months of age for 5 sheep and 24 months of age for 1 sheep. Only 1 of the 6 (16.7%) sheep (sheep No. 27) with recovered infection had developed lesions of OJD; these consisted of mild paucibacillary enteritis and mesenteric lymphadenitis, which resolved within 12 months.
Discussion
The present study is the first to use sequential surgical biopsies to evaluate the chronological establishment of infection and OJD lesions affecting the TI and MLNs of sheep naturally exposed to MAP. This study design allowed detailed observation of the time course of infection and its relationship to OJD lesions, providing the basis to reexamine conventional beliefs regarding OJD pathogenesis which have remained speculative for decades.
The common view contends that sheep are typically infected as neonates. 1,3,11,15 Surprisingly, the incidence rate of microbiologically and histopathologically detectable MAP infection in the present study was steady over the 3-year study period. The largest incidence rate occurred between >18 and 24 months of age. Although neonatal sheep are probably more susceptible to infection than adults, the sheep in this trial were continuously exposed to sheep that were shedding MAP onto pasture, so they may have acquired successive doses of MAP while grazing. The results suggest progressive acquisition of infection, including by adults. The present study used culture methods that have high analytical sensitivity, and tissue culture is believed to be the most sensitive test for MAP infection; it is able to detect MAP in seronegative sheep and in sheep that lack histopathological lesions. 29 However, it is possible that some sheep that were classified as not infected were actually infected at a level below detection limits of this test or in a tissue that was not tested. Although the frequency with which sheep are infected as adults cannot be accurately measured by this study, infection of adult ewes has been observed in other studies, 18,25 and meta-analysis of data from cattle confirmed that adult ruminants may become infected. 28 Further research is needed to clarify the relationship between age of sheep and susceptibility to MAP infection.
A common view also contends that when infected as adults, sheep are less likely to develop disease. 3 In the present study, regardless of age when infection was first recognized, a roughly similar proportion of infected sheep went on to develop disease, either clinical or subclinical. This seems to indicate that the age of the host when infection commences does not necessarily dictate the course of the infection. However, the confidence of this conclusion is tempered by the above uncertainty regarding the timing of initial infection.
MAP infection in cattle and sheep is believed to begin in Peyer’s patches and mesenteric lymph nodes and then progress to involve the intestinal mucosa. 13,21 Consistent with this belief, lesions in the present study were limited to the MLN of several sheep during the early stages of infection (9/30, 30.0%), and at every sampling period, culture of MLN detected a higher proportion of infected sheep than did culture of TI. Little is known regarding the time course for development of lesions once infection is established. In the present study, lesions manifested within 6–12 months following detection of infection but progressed at a variable rate with a proportion of sheep developing severe multibacillary enteritis within 6–12 months of infection being detected and a proportion of sheep developing enteritis that persisted and fluctuated in severity for up to 24 months following the detection of infection. These findings are in agreement with the data in another study in which lesion severity and duration of infection did not correlate among experimentally infected sheep. 15
OJD is believed to result in clinically evident wasting due to malabsorption or protein losses that occur as a result of intestinal mucosal changes. 3 Most sheep in the present study with clinical infection had severe multibacillary enteritis (10/12, 83.3%), corresponding to the classical lepromatous lesions where there is striking distortion of mucosal architecture from diffuse granulomatous infiltrate. 7,9,24 In contrast, this lesion was uncommon among the final TI sections from sheep with subclinical OJD (2/11 TI sections with lesions from subclinical sheep, 18.2%). Because all sheep that were recognized as having severe multibacillary enteritis prior to the final sampling period died or were euthanatized because of clinical disease within 12 months of the lesion being detected, and because no cases of severe multibacillary enteritis regressed in severity or mycobacterial load over time, it appears that this lesion reflects an irreversible end-stage of disease. Notably, 5 of the 17 (29.4%) subclinically infected sheep had severe lesions in final MLN specimens. Therefore, the severity of enteritis seems a more important factor for determining clinical outcome than the severity of mesenteric lymphadenitis. As observed by others 7,9 and similar to observations for bovine Johne’s disease (BJD), 2,8 2 sheep developed clinical signs of OJD without severe enteric granulomatous inflammation or high visible mycobacterial loads. One of these sheep had lymphocyte-rich granulomatous enteritis (sheep No. 71), whereas the other had mild paucibacillary enteritis (sheep No. 8). It is possible that emaciation in sheep with mild enteritis is due to another disease or that MAP infection also causes emaciation through an alternate mechanism such as cytokine-mediated cachexia.
In the present study, much of the variability observed between the lesions of sheep with OJD was explained by the stage of infection. Mild and moderate paucibacillary enteritis is comparable to the early lesions reported by others studying experimental OJD 20 and in the present study occurred after prior microbiological evidence of infection. Furthermore, in 4 sheep, mild or moderate paucibacillary enteritis was observed to progress over time to severe multibacillary enteritis. Consequently, mild to moderate paucibacillary enteritis seems to represents a common initial response to infection that may persist for long periods of time, as hypothesized by others. 22,23 In this regard, the pathology of OJD is more similar to BJD than previously thought. 8
A transition in immune response driven by opposing T-helper (TH) lymphocyte subsets is believed to underlie the development of Johne’s disease in sheep and cattle. 27 Sheep with lesions similar to mild or moderate paucibacillary enteritis (termed type 1, type 2, or type 3a) have been demonstrated to have robust cell-mediated immunity and little humoral response to MAP, 22,23 as is common among sheep in early stages of infection. 31 On the other hand, sheep with lesions similar to severe multibacillary enteritis (termed type 3b) have been demonstrated to have robust humoral and poor cell-mediated immune response to MAP. 22,23 Taken together, these findings suggest that progression in the severity of enteritis and degree of intestinal mycobacterial colonization parallels a switch from a TH1 to a TH2 response.
Intralesional mycobacterial quantity could be expected to be greatest in the late stages of OJD when cell-mediated immunity is least effective. In the present study, most TI biopsies that had severe granulomatous inflammation were multibacillary (15/16, 93.8%), and most that had mild or moderate inflammation were paucibacillary (24/25, 96.0%). This is in concurrence with other investigators who have observed the presence of AFB to be correlated to the extent of intestinal epithelioid macrophage infiltration. 7,9,21,24 However, the biopsies from 2 sheep demonstrate that the level of inflammation is not always directly proportional to the degree of infection. Sheep No. 73 had mild multibacillary enteritis, whereas sheep No. 45 had severe paucibacillary enteritis, the latter being previously described. 19 However, it is possible that the mild multibacillary enteritis observed in sheep No. 73 may have represented an artifact of sampling from the edge of a more severe lesion. In contrast to TI, MLN biopsies were almost always paucibacillary regardless of lesion severity (46/49, 93.9%). This is in accord with others who observed mycobacteria to be more numerous in the intestinal mucosa than in the regional lymph nodes. 9 Perhaps the immune response elicited in proximity to lymphocyte tissue is more effective than that of the ileal mucosa, or perhaps the intestinal microenvironment is more favorable for mycobacterial growth.
There was some variation in lesion character among sheep that could not be explained by stage of disease alone, consisting of a few sheep that had TI lesions that did not fit into the lesion grading scheme used herein. These sheep, which were classified as having lymphocyte-rich granulomatous enteritis (referred to by others as type 3c 21 ; paucibacillary, tuberculoid 9 ; group II 24 ; or tuberculoid 4 lesions), had mild to moderate paucibacillary granulomatous enteritis containing few macrophages but many lymphocytes. Although a lymphocytic response is often difficult to gauge in the intestine given that lymphocytes are normal residents of the tissue, the degree of infiltrate in these cases was striking, causing villous blunting and extending into the submucosa in each case. It is unclear whether the infiltrate was causally related to MAP infection given that the lymphocytic response might have resulted from another cause, and the frequency of lymphocytic infiltrate in noninfected sheep is unknown. However, this lesion type has been described by others studying OJD 7,9,21 and has been postulated to reflect a unique phenotype of immune response where cell-mediated immunity is excessive, potentially comprising a persistent intestinal delayed-type hypersensitivity yet unable to clear MAP. 8,10,23 This lesion type has also been described in cattle (referred to as diffuse lymphocytic paucibacillary lesions), 14 but apparently it is less common in cattle than in sheep. In concurrence with other studies, 7,9 1 sheep (sheep No. 71) was euthanatized for clinical OJD associated with lymphocyte-rich granulomatous enteritis, confirming that these lesions may become clinically significant. However, 2 other sheep with this lesion did not have clinical signs. One (sheep No. 49) progressed to severe multibacillary granulomatous enteritis, and another (sheep No. 45) progressed to moderate paucibacillary enteritis, suggesting that the type of immune response present in lymphocyte-rich lesions is not irreversibly divergent. As none of the sheep with this lesion developed rapid progression of lesion severity, this variant of immune response may be associated with a more favorable prognosis than classical lepromatous enteritis.
It has long been suspected that infected sheep have the capacity to eliminate MAP. 12 In the present study, 6 of the 46 (13.0%) infected sheep had findings that suggested a recovery from infection. At 1 or more early time points, there was evidence of infection in the form of positive tissue culture for MAP with or without enteric lesions of OJD. At a later time points there was no evidence of infection. One of these sheep (sheep No. 27) had mild paucibacillary enteritis and lymphadenitis that had resolved within 12 months. Given the segmental nature of the early intestinal lesions of OJD 7,15,24 and the imperfect sensitivity of tissue culture, it is possible that in some of these sheep infection or lesions remained but were undetected. However, during a thorough necropsy, the most sensitive tests available were applied to show that infection was absent from predilection sites where it had previously been demonstrated. Furthermore, a greater amount of tissue was examined histologically and microbiologically at necropsy compared with biopsy at earlier time points. Therefore, although it is possible that these sheep were not free of infection, the extent of Johne’s disease had regressed. In line with these findings, regression of Johne’s disease has been described in a cow previously showing overt clinical signs. 6
In 31 of the 77 (40.3%) sheep, infection was never detected during the 3-year study period. Given that sheep were continuously exposed to MAP over the study period, this finding suggests that some sheep are resistant to infection.
In conclusion, enteric lesions of OJD typically develop within 6–12 months following initial detection of MAP infection. Some sheep develop severe granulomatous enteritis and substantial intestinal mycobacterial colonization within 12 months of infection, whereas in others, enteritis progresses from mild and paucibacillary to severe and multibacillary at a variable rate, potentially fluctuating in severity or in the character of the inflammatory infiltrate over a period of years. Clinical signs usually become evident in the months following the development of severe multibacillary enteritis. Some sheep may be capable of temporarily or permanently clearing the infection, especially during the early stages of MAP infection. Further study is needed to elucidate host or agent factors that are associated with resistance to infection and favorable prognosis following infection.
Footnotes
Acknowledgements
Special thanks are given to Terry and Cecily Hayes “Hillwood” via Goulburn for ongoing on-farm assistance and to Shayne Fell, Vanessa Saunders, Anna Waldron, Sue Austin, and Kerrie Fisher for skilled technical assistance. Biopsy surgeries were performed at Crookwell Veterinary Clinic by Rob Churchill, Madeline Richard, and Catherine Corkhill of Crookwell Veterinary Clinic and by Richard Whittington and Craig McConnel of the University of Sydney.
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
This study (OJD.020) was funded by Meat and Livestock Australia, NSW Agriculture and the University of Sydney.