
Abstract
Dilated cardiomyopathy (DCM) is the second-most-important acquired cardiovascular disease in dogs (excluding heartworm disease in some geographic regions) and a major cause of morbidity and mortality in Estrela Mountain Dogs. The objective of this study is to describe the histologic features of DCM in Estrela Mountain Dogs, with special attention to the localization and quantification of attenuated wavy fibers (AWFs), fibrosis, and fatty infiltration. Myocardial samples from 10 areas were collected from the hearts of 10 dogs with DCM and 7 dogs without signs of cardiac disease—namely, the basal, middle, and apical portions of the free wall of both cardiac ventricles and the interventricular septum, as well as the left ventricular papillary muscle. In each sample, the presence or absence of AWFs was noted, and fatty infiltration and fibrosis were quantified. Fatty infiltration, fibrosis, and AWFs were observed in the myocardium of all dogs with DCM, in contrast to what has been described in other breeds. The left ventricular myocardium was the best tissue for diagnosis of DCM, based on these histologic features. The authors concluded that quantification of fibrosis and observation of AWFs in the left ventricular myocardium are useful in the histologic diagnosis of DCM in Estrela Mountain dogs.
Dilated cardiomyopathy (DCM) is a primary myocardial disorder characterized by dilation and reduced contractility of the left ventricle (LV) or both ventricles, with an unknown or familial origin. 17 It is the second-most-important cardiovascular disease in dogs (excluding heartworm disease in some geographic regions) 21 and a major cause of morbidity and mortality in Estrela Mountain Dogs (personal observation). The Estrela Mountain Dog is a large molossoid breed thought to have been used for sheepherding since ancestral times. Originating from Portugal and spreading through Europe, it has recently increased in popularity in the USA. The molossoid group, whose archetypical breed is the Tibetan Mastiff, includes breeds that share similar physical characteristics with Estrela Mountain Dogs, such as the Great Pyrenees and the Pyrenean Mastiff, but it also includes other related breeds, such as the Newfoundland, Saint Bernard, and Bernese Mountain Dog. The Estrela Mountain Dog has a known predisposition for DCM, 13 –15 but to the best of our knowledge, the histologic features of DCM in this breed have not been reported.
In the clinical diagnosis of DCM, other causes of cardiac dilation and hypokinesis should be ruled out, and the diagnosis should be confirmed postmortem whenever possible. 6 Some dogs with DCM die unexpectedly in the preclinical, asymptomatic stage of the disease; 17,18 as such, the postmortem—specifically, histologic—examination is one of the most important tools in the diagnosis of the disease. Attenuated wavy fibers (AWFs), fibrosis, and fatty infiltration have been described as the main histologic abnormalities in canine DCM. Two histologically distinct forms of DCM are recognized: 6,24,28 the fatty infiltration–degenerative type, mainly seen in Boxers and Doberman Pinschers, and the AWF type, seen in many large or giant breeds. 1,5,22,26,27,32 These disparate histologic findings could reflect differences in pathogenesis, 28 but the progression from myocardial lesions to clinical disease is poorly understood, 12,25 and fatty infiltration and fibrosis are nonspecific responses to myocardial injury. 3,7,9,23,28,30,31 However, the quantification of these histologic features could provide insight into the pathogenesis and diagnosis of DCM in Estrela Mountain Dogs and other breeds of dogs. The objective of this study was to describe the myocardial lesions of DCM in Estrela Mountain Dogs, giving special attention to the presence, localization, and quantification of AWFs, fibrosis, and fatty infiltration.
Material and Methods
Animals
Hearts from 17 Estrela Mountain Dogs were collected at necropsy: 10 from dogs with DCM and 7 from control dogs without clinical DCM. The antemortem diagnosis of DCM was based on proposed guidelines 6 and published echocardiographic reference values for the breed. 13 All control dogs died from noncardiac causes: 1 was killed by vehicular collision; the others were euthanized because of neoplasia (n = 5) or hip dysplasia with cauda equina syndrome (n = 1). Each control dog had been subjected to clinical, echocardiographic, and electrocardiographic examinations that excluded DCM.
The age of dogs with DCM ranged from 4.6 to 14.5 years; control dogs were 1 to 13 years old. Control dogs were divided into 2 groups (< 18 months old, > 60 months old) to study the influence of age on myocardial fibrosis or fatty infiltration in dogs without DCM.
Pathologic Procedures
At necropsy, the heart was opened according to a transverse base-to-apex orientation and fixed in 10% buffered formalin for 72 hours, with replacement of the formalin after the first 24 hours. Myocardial samples for histologic processing were sliced from the basal, middle, and apical portions of the free wall of the LV, right ventricle (RV), and interventricular septum (IVS). A sample was also collected from the papillary muscle (PM) of the LV, making a total of 10 myocardial samples. From each sample, 2 cross-sectional specimens were collected to include the entire thickness of the ventricular wall. The specimens were processed by routine histologic methods, embedded in paraffin, sectioned at a thickness of 3 to 5 μm, and stained with HE and Masson’s trichrome. Each sampling site was evaluated for AWFs, fibrosis, and fatty infiltration.
Samples were considered positive for AWFs (myocardial cells < 6 μm in diameter with a wavy appearance) if at least half the thickness of the section was composed of AWFs. 6,25 The reference range for myocardiocyte diameter was 10 to 20 μm. 31
Fibrosis and fatty infiltration were quantified in Masson’s trichrome-stained sections at 100× magnification (Nikon Eclipse E600 microscope, Nikon, Tokyo, Japan). Ten fields were evaluated in both sections from each sampling site (ie, 20 fields per site). The number of microscopic fields with fatty infiltration or fibrosis was recorded, and affected fields were photographed (with care to exclude epicardial or perivascular adipose or fibrous tissue 3 ). Image analysis was performed by superimposing a 16-cell grid over the digital image. Results were recorded as the number of cells with fatty infiltration and/or fibrosis divided by 320 (the number of grid cells in 20 fields).
Statistical Analysis
The chi-square test was used to compare the association of fatty infiltration and fibrosis with DCM. Significance was defined as P < .05. Chi-square analysis was also applied to the 2 age groups of control dogs. For each parameter, odds ratios were calculated from 2 × 2 tables of contingency (based on number of fields or grid cells with either fibrosis or fatty infiltration) to evaluate the association between that parameter and the diagnosis of DCM.
Based on results, parameters from the middle LV were evaluated to determine whether differences between DCM and control dogs could be used to set a diagnostic cutoff value. For this purpose, 7 groups were formed on the basis of the highest Youden’s J statistic, as segregated by the number of affected microscopic fields: 0–2, 3–5, 6–8, 9–11, 12–14, 15–17, 18–20. 2 All parameters were computed for a level of confidence of 95% (Win Episcope computer software, version 2.0, CLIVE, Edinburgh, Scotland). 10
Results
The most relevant gross finding in DCM hearts was marked dilation with a rounded profile of the LV and thinning of the left ventricular wall (Fig. 1). In the control group, dog No. 16 had dilation of the RV. The median heart weight of DCM dogs exceeded that of control dogs (393.5 g vs 324.2 g, respectively). With regard to the median heart weight of dogs only in International Small Animal Cardiac Health Council (ISACHC) class II and III heart failure functional classification (464.1 g), 11 this difference was significant.
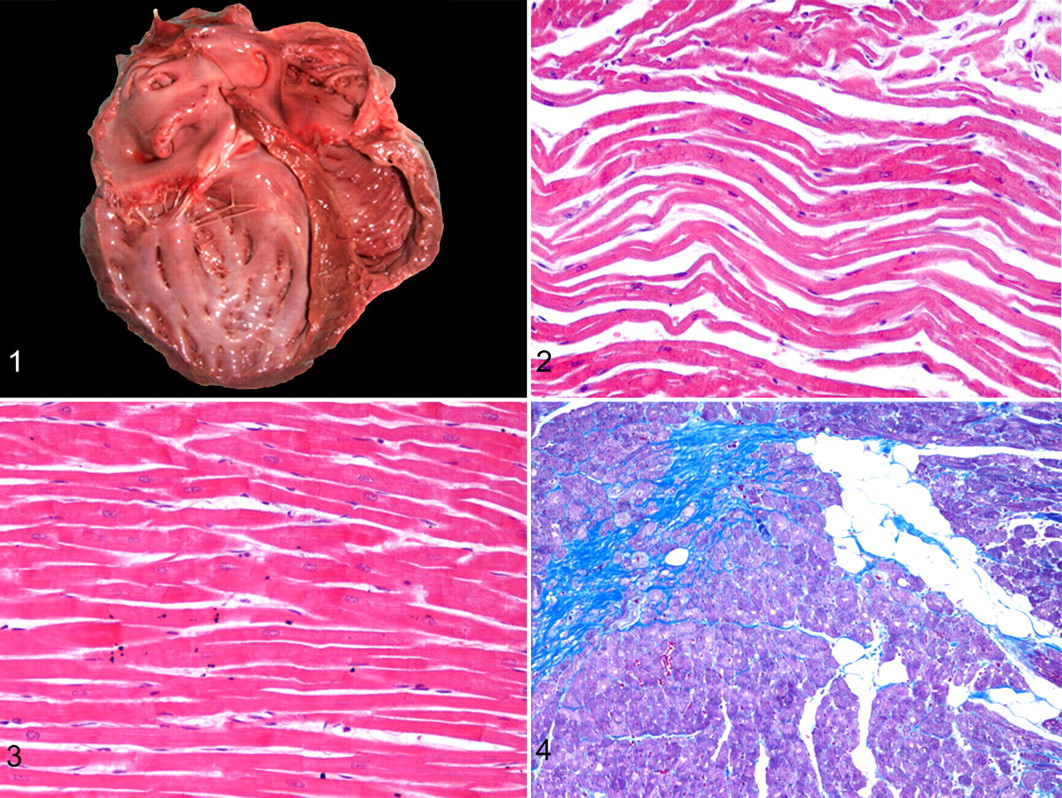
The observation of AWFs (Figs. 2, 3) was more frequent in DCM dogs than in control dogs for all myocardial sampling sites (Table 1). In control dogs, AWFs were observed in only the middle and basilar portions of the RV. The overall specificity of AWFs for the diagnosis of DCM was 57.1%. With only the LV for the diagnosis of DCM based on the presence of AWFs, the diagnosis sensitivity was 70% and specificity was 100%. The LV had the best combination of sensitivity and specificity for AWFs, with a Youden’s J statistic number of 0.7. (Youden’s J statistic combines information about sensitivity and specificity into a single number between 1 and –1. 2 ) Two DCM dogs (dog Nos. 5 and 7) were negative for AWFs. In these 2 dogs, AWFs were observed but did not fulfill the criteria for positivity (ie, at least half the thickness of the specimens composed of AWFs) in any sampling site.
Number of Dogs With Attenuated Wavy Fibers, by Myocardial Site a

a Number of dogs with more than half the myocardial thickness composed of attenuated wavy fibers. LV, left ventricle; RV, right ventricle; IVS, interventricular septum; PM, papillary muscle (left ventricular); A, apical; M, middle; B, basal.
The number of microscopic fields and grid cells with fatty infiltration or fibrosis (Fig. 4) was significantly higher in dogs with DCM than in control dogs (P < .0001). The odds ratio was higher with the field-counting method than with the grid method (2.5 vs 1.9 for fibrosis; 2.6 vs 2.0 for fatty infiltration). Therefore, results are presented as the proportion of affected fields.
The amount of fibrosis in the LV, RV, and IVS of DCM dogs was significantly higher (P < .0001) than in control dogs. No difference was detected between the groups for PM sections. Fibrosis was more severe (P < .05) in DCM dogs in each site from the LV, for the middle and apical RV sites, and for the middle site of the IVS. The odds ratio for fibrosis was highest for the middle LV—specifically, 17 times higher in DCM dogs than in control dogs. No significant difference between groups was observed in the basal RV (P = .165) or basal and apical IVS (P = .186 and .069, respectively). Fatty infiltration was also more severe in DCM dogs than in control dogs (P < .05) at all sites, with the highest odds ratio in the middle LV (5.018).
In control dogs, fibrosis was more severe (P < .05) in the older group in all sites except the middle and apical LV (P = .744 and .130, respectively), middle RV (P = .068), and PM (P = .090). Fatty infiltration was also more severe in older control dogs, except in the basal IVS (P = .270) and PM (P = .080).
When data from the middle LV (site with the highest odds ratio) were analyzed for a difference between DCM and control dogs in the number of microscopic fields with fibrosis, > 5 fields was set as the cutoff value for the diagnosis of DCM in Estrela Mountain Dogs, with sensitivity of 88.9%, specificity of 100%, and confidence level of 95%. The same cutoff value was set for fatty infiltration in the middle LV but with lower sensitivity (77.8%) and specificity (85.7%) for the same level of confidence.
Discussion
The presence of AWFs, fibrosis, and fatty infiltration has been used in different dog breeds for histologic characterization and diagnosis of DCM. 1,22,32 The 2 histologic types of DCM (fatty infiltration–fibrosis type and AWF type) are usually associated with different breeds of dogs, with each breed having a specific type of DCM. 4,6,8,16,19,24,26 –28 However, fatty infiltration, fibrosis, and AWFs coexisted in Estrela Mountain Dogs with DCM. In a study of Newfoundland dogs with DCM, AWFs and interstitial fibrosis were the major histologic changes; fatty infiltration was not observed. 27
AWFs have been attributed to chronic volume overload in DCM with stretching of cardiomyocytes. 20 A more recent study demonstrated AWFs in the myocardium of Newfoundland dogs without clinical or echocardiographic evidence of heart disease. 25 In another study of dogs with cardiac disease, AWFs were not found in dogs with cardiac disease other than DCM. 26 These observations suggest that, at least in some breeds, AWFs do not represent an end-stage response to chronic volume overload and myocyte stretching but are rather a histologic feature of DCM and could represent an early stage of the disease. In fact, the presence of AWFs has been used for diagnosis of DCM in various breeds of dogs, with sensitivity and specificity as high as 98% and 100%, respectively. 26,27 In the present study, sensitivity and specificity were 70% and 100%, respectively, in the LV. As based on the Youden’s J statistic, the index value was 0.7, which is acceptable for diagnostic purposes.
Two dogs in the DCM group had AWFs but did not meet the criteria for a positive score (at least half the thickness of the specimens composed of AWFs) in any sampling site. These criteria may be too strict for diagnosis of DCM in Estrela Mountain Dogs; perhaps a lesser degree of AWFs should render the dog positive for the disease. Those 2 dogs had similar clinical presentations: Both were functionally classified as ISACHC class Ib heart failure, 11 and both died of noncardiac causes (dog No. 5 died from an hematopoietic disease; dog No. 7 was euthanized because of severe hip dysplasia). In contrast, dog Nos. 3, 4, 8, and 10 died from end-stage heart failure attributed to DCM (ISACHC class III). Interestingly, these were the dogs with more positive sites for AWFs. These observations suggest a direct relationship between disease progress and presence of AWFs.
The data in Table 1 suggest that evaluation for AWF could be a sensitive method for the diagnosis of DCM. Nevertheless, given the observation of AWF in the RV of 3 control dogs, the overall specificity of this observation was low (57.1%). Dog No. 12 was an 8-year-old male euthanized for severe hip dysplasia and cauda equina syndrome. Dog No. 16 was a 11-year-old female euthanized for pulmonary neoplasia; this dog had echocardiographic signs of right heart dilation secondary to pulmonary hypertension. Dog No. 17 was a 14-month-old dog that died after being hit by a vehicle. The presence of AWF could represent an early lesion of DCM in dogs without any clinical, echocardiographic, or electrocardiographic signs of the disease. 26 Also, according to some authors, 20 the right ventricular dilation in dog No. 16 could explain the presence of AWF.
The process for preparation of histologic slides could produce artifactual waviness (but not attenuation) of cardiac myofibers. 29 However, this would not explain the presence of AWF in the dogs in this study, which had both waviness and attenuation in myofibers.
To the best of our knowledge, fatty infiltration and fibrosis in the myocardium of dogs with DCM have not been quantified. Previous investigators reported topographic distribution 8,27 or subjectively graded the lesions as mild, moderate, or severe. 4 In contrast, in human medicine, especially for arrhythmogenic right ventricular dysplasia, the quantification of fatty infiltration and fibrosis is important in diagnosis and in differentiation of arrhythmogenic right ventricular dysplasia from pure intramyocardial fat replacement. 3,23 Moreover, intramyocardial fat can be observed in healthy people, where it is thought to reflect the normal physiological process of involution that occurs with aging. 23 Fatty replacement of the RV, with no significant fibrosis, may be seen in patients who die of noncardiac causes. 22 Pure fat replacement may be considered a distinct clinicopathological entity but not necessarily a cause of arrhythmogenic death when identified at autopsy. 3 Adipocytes interposed between myocardial fibers have also been associated with obesity in veterinary medicine. 31
In the present study, 2 methods were used to quantify myocardial fatty infiltration and fibrosis: the field method and the grid method. Both methods were accurate in distinguishing DCM dogs from control dogs. The field method is easier and faster in a practical setting and resulted in a higher odds ratio.
Fatty infiltration in LV, RV, IVS, and PM was more severe in Estrela Mountain Dogs with DCM than in controls. In a study with Doberman Pinschers, fatty infiltration was rarely found. 4 Fibrosis was also found in all parts of the heart in Estrela Mountain Dogs, except in the left ventricular PM. Interestingly, this was the area with the most severe fibrosis in Doberman Pinschers. 4 However, in another study of Doberman Pinschers, fibrosis and fatty infiltration were exclusively in the left ventricular free wall. 8
In conclusion, both histologic types of DCM—fatty infiltration–degenerative and AWF—are concomitantly observed in Estrela Mountain Dogs. In this study, the middle portion of the left ventricular free wall had the most severe fibrosis and fatty infiltration. We propose that the middle portion of the left ventricular free wall is the best site for histologic evaluation in the diagnosis of DCM, at least in the Estrela Mountain Dog. Importantly, fibrosis in this cardiac region was not influenced by age in control dogs. Based on the results of this study, the finding of more than 5 of 20 microscopic fields (100×) affected by fibrosis in the middle LV warrants a diagnosis of DCM in Estrela Mountain Dogs. Quantification of fibrosis and observation of AWF in the LV facilitates the histologic diagnosis of DCM. Future studies should test the validity of these results in other dog breeds.
Footnotes
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.