
Abstract
In dogs, autoimmune subepidermal blistering diseases (AISBDs) encompass several distinct entities that exhibit varying clinical signs, microscopic characteristics, prognosis, and response to treatment. The identification of targeted autoantigens is usually required to make the diagnosis, but immunological tests to determine these antigens are not commercially available. Epidermolysis bullosa acquisita (EBA) is an AISBD characterized by the production of autoantibodies against collagen VII in sublamina densa anchoring fibrils. This article reports on the usefulness of collagen IV immunostaining on paraffin-embedded skin biopsies as an aid to diagnose EBA in dogs. In this disease, collagen IV, which forms the fibrous 2-dimensional network of lamina densa, is detected more commonly above subepidermal vesicles than below. In other canine AISBDs, this is rarely the case. Collagen IV immunostaining therefore offers an inexpensive means to help making a suggestive diagnosis of EBA in the absence of serological determination of the targeted autoantigen.
In human and animals, subepidermal blistering dermatoses are principally divided into those of genetic or autoimmune pathogeneses. Whereas genetic vesicular diseases (ie, mechanobullous dermatoses of the hereditary epidermolysis bullosa group) are classified on the basis of clefting level and causative mutated genes, autoimmune subepidermal blistering diseases (AISBDs) are separated on the basis of clinical signs and targeted autoantigens. At this time, canine AISBDs are a group of heterogeneous skin diseases that encompass, in order of historical description, bullous pemphigoid (BP), 1 epidermolysis bullosa acquisita (EBA), 9 type I bullous systemic lupus erythematosus, 10 linear immunoglobulin A bullous disease (LAD), 6 mucous membrane pemphigoid (MMP), 8 junctional EBA, and mixed AISBDs. 7 Whereas trained specialists can make diagnoses based on unique clinical phenotypes (eg, bilaterally symmetrical erosions and ulcers affecting several mucous membranes in MMP, blisters and erosions affecting friction areas and footpads in EBA) 8,9 or the presence of characteristic histological findings (eg, eosinophil-rich subepidermal vesicles in BP), 3 they cannot diagnose most entities without the identification of targeted autoantigens. Making a specific diagnosis is important because of the seemingly variable prognoses and responses to immunomodulating drugs among these diseases. For example, canine EBA appears to be more difficult to treat than MMP, and its lesions do not normally respond to tetra(doxy)cyclin-niacinamide combinations as MMP lesions usually do. 4,5 Unfortunately, immunological tests needed to establish the target of circulating autoantibodies are not commercially available. Pathologists and clinicians are therefore often left with a morphological diagnosis of “likely autoimmune subepidermal vesicular dermatitis” without confirmation of the specific diagnosis.
The objective of this article is to report the use of a simple immunohistochemical stain that allows the differentiation of canine EBA from other AISBDs. Indeed, in dogs with EBA, collagen IV is usually present above blister cavity, whereas it is usually seen below the clefts in the other entities.
Paraffin-embedded blocks or unstained sections of lesional skin biopsies were selected from 35 dogs with AISBDs based on the following criteria: First, a specific diagnosis had been made on the basis of suggestive clinical signs, histopathology, and identification of targeted autoantigens; second, subepidermal clefts were visible on microscopic examination of hematoxylin and eosin–stained sections. Among these 35 dogs, there were 14 with EBA, 13 with MMP, 4 with junctional EBA, 2 with mixed AISBDs, 1 with BP, and 1 with LAD.
Immunostaining for collagen IV was done on 4- to 6-μm paraffin-embedded sections per a 3-step immunoperoxidase technique. Briefly, sections were first deparaffinized and rehydrated, and endogenous peroxidase activity was quenched with hydrogen peroxide and sodium azide. Antigen retrieval was made with pepsin proteolysis (0.5% pepsin in 5mM HCl at pH 6.0 for 20 minutes at 37°C). The primary anti–collagen IV immunoglobulin M monoclonal antibody (MA1-35333, Affinity Bioreagents, Thermo Fisher Scientific, Rockford, IL) was applied overnight at 1:20 at room temperature. This antibody has been shown to recognize collagen IV in human and canine tissues. Later steps consisted of incubation with biotinylated rabbit anti-mouse immunoglobulin M (315-065-049, Jackson Immunoresearch, West Grove, PA; 1:100, 30 minutes at room temperature) followed by streptavidin-peroxidase (43-8323, Zymed Laboratories, South San Francisco, CA; 1:400, 30 minutes at room temperature) and amino-ethyl carbazole as needed (AEC substrate kit, HK 129-5K, Biogenex, San Ramon, CA).
Immunostained sections were examined for blister formation and the location of collagen IV at these sites. The latter was assessed as being located above and/or below any of the subepidermal clefts.
In 2 dogs with MMP, collagen IV could not be seen in any parts of the skin sections, presumably because a long duration of fixation had altered its antigenicity; tissues from these dogs were therefore removed from further analysis.
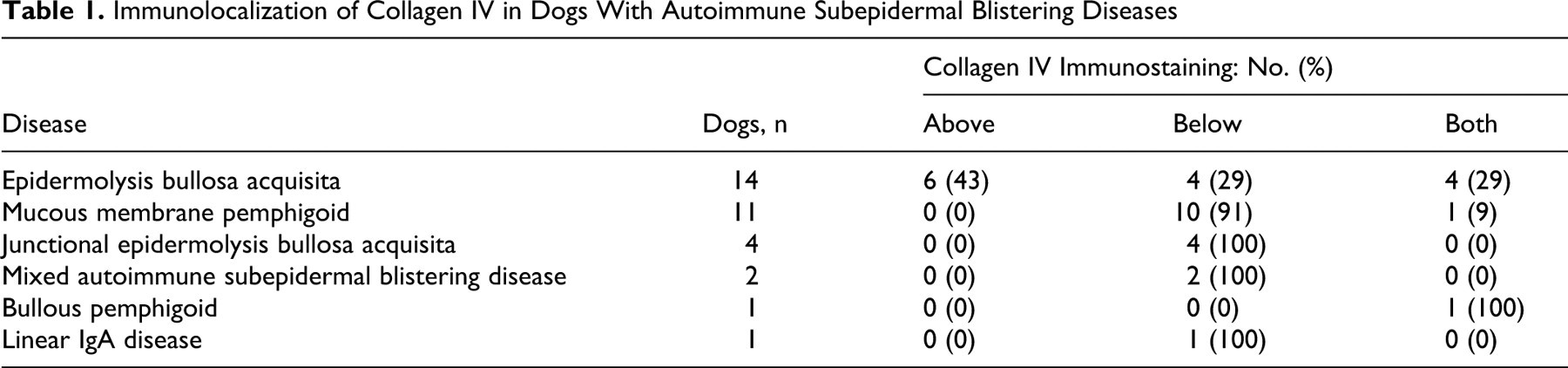
Table 1 presents the results of the immunolocalization of collagen IV. Collagen IV immunoreactivity was observed solely above subepidermal clefts in 6 dogs, all with EBA (Fig. 1A). It was present only at the base of vesicular lesions in 4 dogs with EBA (Fig. 1B) and in 17 dogs with other diseases (Figs. 1E, 1F). In 4 dogs with EBA (Figs. 1C, 1D), 1 dog with BP, and 1 with MMP, collagen IV was located on both sides of spontaneous vesicular lesions.
Immunolocalization of Collagen IV in Dogs With Autoimmune Subepidermal Blistering Diseases
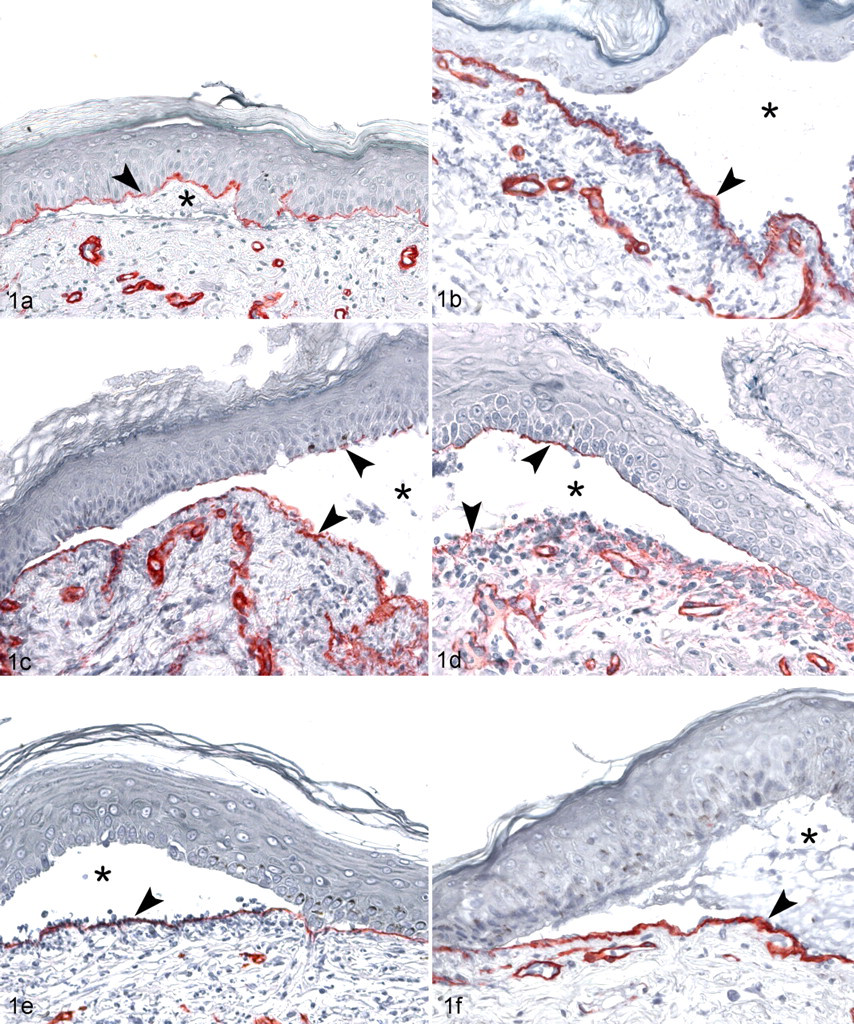
Skin; dogs with epidermolysis bullosa acquisita (EBA), bullous pemphigoid (BP), and linear IgA disease. In dogs with EBA, immunostaining for collagen IV (arrowheads) is most commonly seen above subepidermal vesicles (asterisks; A). In some dogs with EBA, collagen IV can be located below (B) or on both sides of the clefts (C, D). When present on both vesicle roof and floor, collagen IV staining will most often appear irregular and of varying intensity (perhaps digested) on the dermal side of the clefts (C, D). In contrast, in dogs with autoimmune subepidermal blistering diseases different from EBA, such as bullous pemphigoid (E) or linear IgA disease (F), immunostaining for collagen IV will usually be seen below subepidermal vesicles.
A 2 × 2 contingency table was generated for the parameter presence of collagen IV above a subepidermal cleft with 2 distinct groups of dogs: those with EBA (n, 14) and those with other diseases (n, 19) (Table 2 ). When collagen IV was observed on both sides of subepidermal vesicles (ie, above and below blister cavity), it was recorded in the yes column for this parameter.
Contingency Table for the Parameter Presence of Collagen IV Above a Subepidermal Cleft
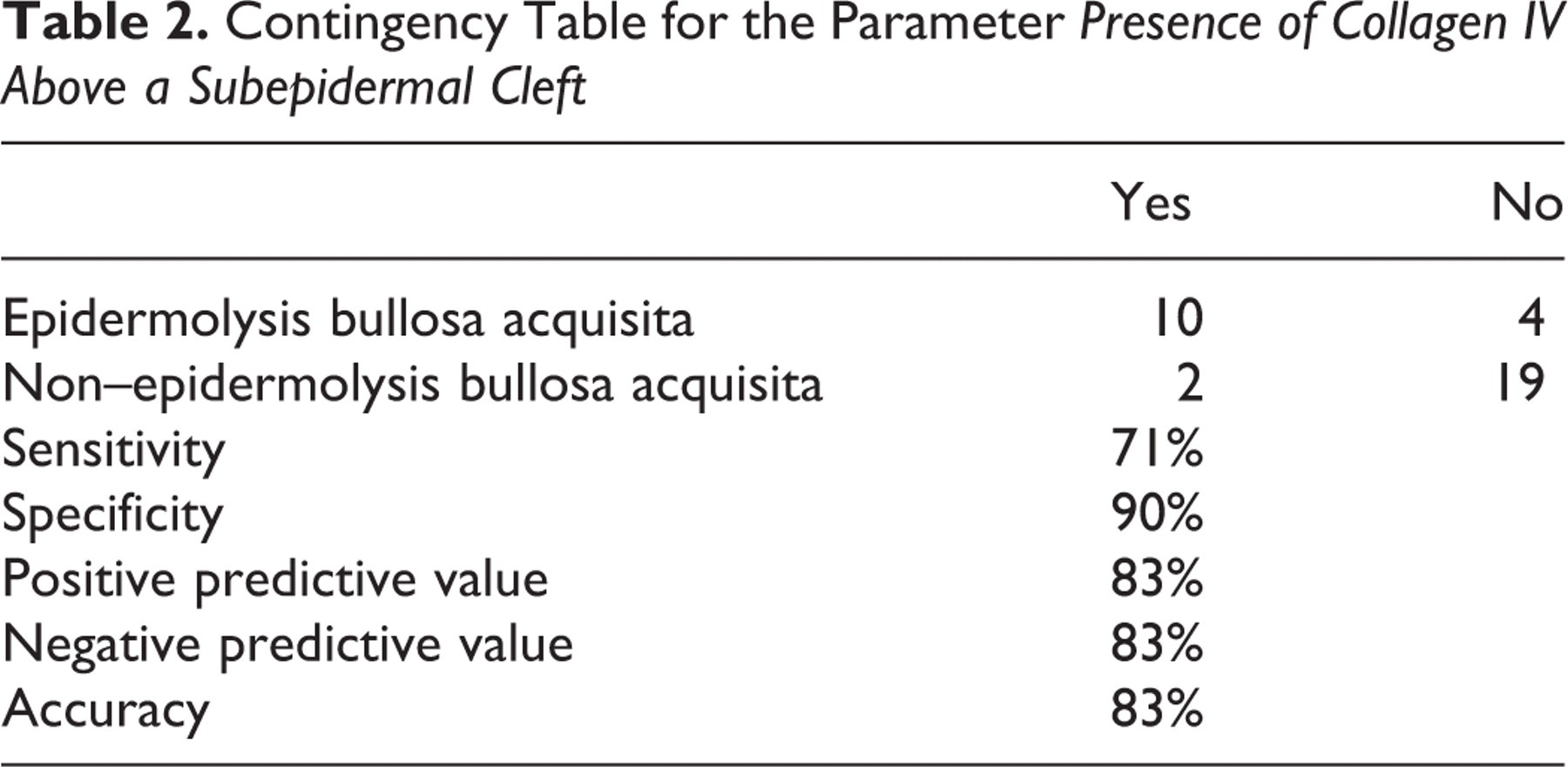
There was a significant difference in the prevalence of this parameter between the 2 groups of dogs (2-tailed Fisher test, P = .0003). Based on this table, the presence of collagen IV above subepidermal clefts was calculated to exhibit a sensitivity of 71%, a specificity of 90%, and a positive predictive value and accuracy of 83% for the diagnosis of canine EBA.
In dogs and humans with EBA, immunoglobulin G autoantibodies target collagen VII, the nearly exclusive component of anchoring fibrils in the lamina densa. 4,11 In both species, mapping studies have established the noncollagenous NC1 aminoterminal domain of collagen VII as the segment harboring major antigenic epitopes. 4,11 During anchoring fibril formation, 2 molecules of collagen VII assemble into antiparallel dimers linked at their carboxyterminal termini, thereby leaving a large globular NC1 domain protruding at each aminoterminal end. These NC1 ends bind to the beta-3 chain of laminin-332 (laminin-5) in the lamina densa. 2 Because anchoring fibrils have now been shown to form loops originating and terminating in the lamina densa of the epidermal basement membrane, it is not surprising that the binding of autoantibodies from patients with EBA to their NC1 targets results in the separation of dermal anchoring fibrils from the lamina densa. 2 During EBA, dermo-epidermal separation therefore most often occurs in the sublamina densa—that is, below collagen IV. 11 Because there is prominent infiltration—and presumed activation—of neutrophils in the superficial dermis and blister cavity in dogs with EBA, lamina densa proteolysis is likely to occur, thereby resulting in occasional collagen IV immunostaining below blister cavities.
We established this immunostain for collagen IV to take advantage of this unique blister formation characteristic of EBA among AISBDs. Indeed, our study confirmed that collagen IV could be seen above subepidermal clefts in 10 of 14 dogs with EBA (71%). This observation, however, was made in only 2 of 19 dogs (10%) with non-EBA AISBDs that exhibited a combined pattern (ie, immunostaining present above and below blister cavities).
At this time, an immunological test for the determination of collagen VII autoantibodies in dogs with EBA is not commercially available. The observation of collagen IV above any subepidermal cleft will therefore help improve the diagnosis of EBA because this parameter has an appreciable positive predictive value and accuracy (83%) for such diagnosis compared to that of the other canine AISBDs.
In conclusion, collagen IV immunostaining of paraffin-embedded lesional skin sections is a fairly inexpensive and easy immunohistochemical stain that can be recommended as an aid to improve the pathologic diagnosis of canine EBA.
Footnotes
Acknowledgements
We thank Drs Petra Bizikova and Keith Linder for their constructive review of this article.
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.