
Abstract
A 9-year-old female Golden Retriever was presented with an acute onset of progressive respiratory distress. Echocardiography revealed a left atrial mass that limited blood flow from the pulmonary veins. The pathological evaluation revealed a left atrial ossifying myxosarcoma, bilateral adrenocortical adenomas, multifocal pituitary hyperplasia with expression of adrenocorticotrophic hormone, and multiple pituitary Rathke's cleft cysts. These pathologic findings are similar to those described in Carney complex, a familial human syndrome characterized by cardiac myxoma and extracardiac tumors associated with mutations in the protein kinase A regulator gene PRKAR1A. Mutations were not detected in PRKAR1A exons in the present case.
Keywords
Cardiac myxoma is an endocardial neoplasm originating from multipotent mesenchymal cells in the subendocardial layer that can differentiate into various cell types. 9 Cardiac myxomas are rare primary heart tumors in dogs. 2,3,8,10,13,14 In humans, myxomas compose 50% of primary cardiac neoplasms and present as a single lesion or with other proliferative lesions as Carney complex (CNC). 7 CNC is a genetically heterogeneous, autosomal dominant syndrome resulting in multiple cardiac, endocrine, cutaneous, and neural tumors, as well as a variety of pigmented lesions of the skin and mucosae. 12,16 The diagnosis of CNC in humans requires two or more of the following: cardiac myxoma (usually affecting the left atrium), primary pigmented nodular adrenocortical disease (PPNAD) with or without Cushing' syndrome, growth hormone- or prolactin-producing pituitary adenomas, melanocytic nevi, thyroid nodular hyperplasia or carcinoma, testicular neoplasms, schwannoma, and certain other proliferative lesions. 12,16 In approximately 40% of the CNC kindreds, a variety of inactivating mutations of the protein kinase A R1 alpha regulatory subunit (PRKAR1A) and subsequent unregulated protein kinase A signaling have been described. 12 To our knowledge, the concomitant presence of primary cardiac myxosarcoma with extracardiac tumors, or a CNC-like condition, has not been described as a spontaneous condition in animals. Here we describe the morphologic and genetic findings of cardiac myxosarcoma with bilateral adrenocortical adenoma and hyperplastic pituitary lesions in a dog.
History
A 9-year-old spayed Golden Retriever was presented to the Ontario Veterinary College for an acute onset of progressive respiratory distress over the past 12 hours. Physical examination revealed severe tachypnea, dyspnea, cyanotic mucous membranes, harsh sounds in all lung fields, weak peripheral pulses, and mild hyperthermia (39.6°C). Thoracic radiographs demonstrated cardiomegaly and suggested pulmonary edema. Echocardiography revealed a mass that filled the left atrium, limited blood flow from the pulmonary veins, and caused a functional obstruction of flow through the left atrioventricular orifice. The dog was euthanized on the basis of poor prognosis.
Pathologic Findings
A cardiac mass originated from the interatrial septum and filled the left atrium; the mass was 5 cm in diameter, multinodular, pedunculated, and firm (Fig. 1 ). Projections of the mass extended 2.5 cm into the intrapulmonary branches of the pulmonary veins, where they loosely adhered to the intima. The mass had a smooth pink surface and was white, gelatinous, and gritty on cut section. The lungs were congested and edematous.
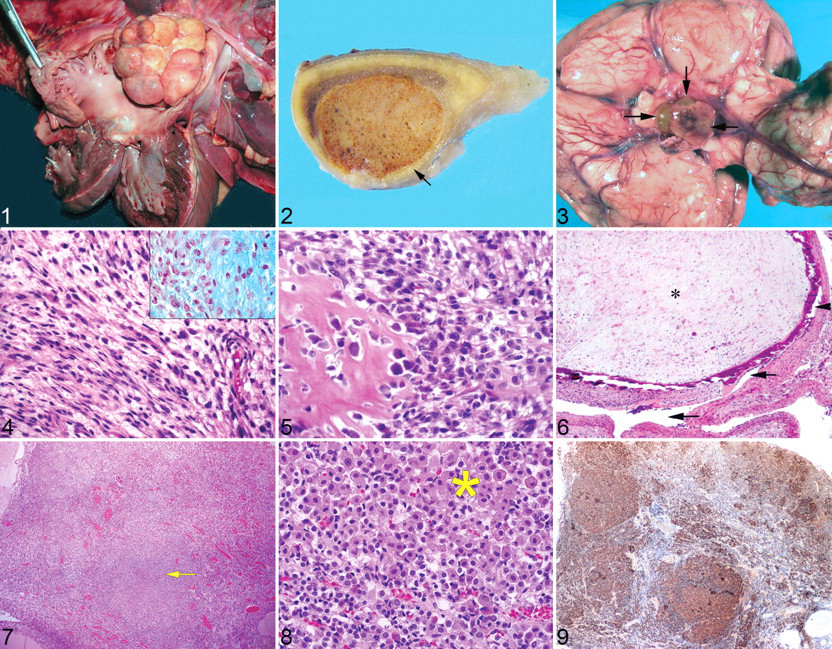
The left adrenal gland was enlarged (13.5 g), and it contained 2 soft variegated tan and red nodules of 1.5 and 1.0 cm diameter that compressed the cortex. The right adrenal gland weighed 3.5 g and contained a 0.75-cm-diameter mass that also compressed surrounding cortical tissue (Fig. 2 ). The pituitary gland was enlarged and had 3 brown cysts, 2 to 4 mm in diameter (Fig. 3).
Tissues were fixed in 10% neutral-buffered formalin and processed routinely. Histologically, the cardiac mass was composed of an abundant, lightly eosinophilic, myxoid matrix in which were scattered spindle-shaped to stellate cells that had scant eosinophilic fibrillar cytoplasm, round to spindle-shaped nuclei with granular to stippled chromatin, moderate anisokaryosis, and 4 mitotic figures per 400× field (Fig. 4). The center of the mass contained expanses of fibrous tissue and scattered foci of osteoid or cartilaginous matrix in close association with the neoplastic cells (Fig. 5). By immunohistochemistry, neoplastic cells throughout the mass expressed vimentin but not smooth muscle actin or S-100 protein. The matrix contained acidic mucopolysaccharides (Alcian Blue stain, pH 2.5) (Fig. 4, inset), abundant collagen (Masson’s trichrome stain), reticulin (Wilder’s reticulum stain), and scant amounts of elastic fibers (Verhoeff van Gieson stain). Extensions of the tumor into pulmonary veins were of lower cell density and were covered by endothelial cells that expressed CD31 (Fig. 6 ).
The nodules in both adrenal glands were well circumscribed and compressed the cortical and medullary structures. The nodules were composed of microvacuolated cortical epithelial cells with eccentric nuclei. Mitotic figures were not seen. Throughout the mass were small and large blood-filled cavities with numerous pigment-laden macrophages that were stained with Perl’s Prussian blue stain (hemosiderin) and were faintly periodic acid–Schiff reactive (lipofuscin) but did not stain with Nile blue (melanin).
Within the adenohypophyseal parenchyma were 4 well-demarcated 0.50- to 1.75-mm-diameter foci (Fig. 7) that contained large, round to polygonal cells with abundant pale hyaline cytoplasm, a central hyperchromatic round nucleus, and no mitotic figures (Fig. 8). Immunohistochemistry, performed by the University of Minnesota Veterinary Diagnostic Laboratory, revealed that nearly all the cells in these foci expressed adrenocorticotrophic hormone (ACTH) (Fig. 9). The expression of other hormones was not examined. The pituitary cysts contained homogeneous eosinophilic fibrillar material and were lined by a simple squamous to cuboidal ciliated epithelium. Smaller cysts were present within the parenchyma. At the margin of one of the cystic structures was a disorganized structure composed of small cysts lined by and admixed with large cells with karyomegaly, prominent nucleoli, and a single mitotic figure.
Genetic Analysis
For sequence analysis of the PRKAR1A gene, DNA was extracted from the formalin-fixed paraffin-embedded cardiac tumor, and the 10 predicted exons were separately amplified by PCR and sequenced. Primers were designed on the basis of the predicted coding sequence of the canine Prka1a gene (NCBI accession number = XM_537577). The forward (F) and reverse (R) primers and product size (PS) were as follows: exon 1 (PS = 310 base pairs; F 5′-AGCAGTCGCCTGATGAATTT; R 5′-TGACGCCATCTTGGATCG); exon 2 (PS = 300; F 5′-TGGAGATTGGTTCTCACTGG; R 5′-CGTGGGTCCTGAAAACATCT); exon 3 and 4 (PS = 405; F 5′-TCTGTTTTTCATTTATGGGATTG; R 5′-CGTGGGTCCTGAAAACATCT); exon 5 (PS = 269; F 5′-CACACTTTTCTCTCAGTACCTCT; R 5′-GGGTTATTAACAGCCCTTCAGA); exon 6 (PS = 316; F 5′-CATTAACTGTTTTGCTCTGCTG; R 5′-TAAAAACCTCGCCGTCTCAC); exon 7 (PS = 333; F 5′-CCCAGCCTGGTGTTACCTT; R 5′-GCAATCTTCCCAAACTCACC), exon 8 (PS = 420; F 5′-GGCACAGCTGTCTGATTCTCT, R 5′-AAAGCCCTTCTGACTCAAACC), exon 9 (PS = 295; F 5′-TGTCACCCTGGATTTGAAAG; R 5′-TCTGAGAGCCAGGAAGGAAA), exon 10 (PS = 500; F 5′-ACACACACACCCGATGCTC; R 5′-CGCTGCCTAGGTTGAACAC). The coding sequence of the PRKAR1A gene derived from the cardiac tumor was identical to the predicted coding sequence (NCBI XM_537577).
Discussion
The atrial tumor was diagnosed as a cardiac ossifying myxosarcoma based on the myxomatous features, including Alcian blue staining, and the scant presence of osteoid apparently produced by the neoplastic cells. The diagnosis of malignancy (myxosarcoma) was based on cellular pleomorphism and mitotic activity, 11 although the well-circumscribed, expansile, and nonmetastatic features were compatible with a benign neoplasm. The distinction between myxosarcoma and myxoma may be uncertain, 11 and many features of the present case resemble those in previous reports of cardiac myxoma in animals. 5,13 Diagnosis is further complicated by the multidirectional mesenchymal differentiation of cardiac myxomas, 15 consistent with the osteoid and chondroid matrix production in the present tumor. Furthermore, the histologic appearance of myxomas varies by site, clinical presentation, and patient age. 4 Although cardiac myxomas usually present as benign, features of malignancy—including recurrence, local invasion, extension from the heart, and distant metastasis—have been documented in humans. 1 Embolism of a myxoma to intrapulmonary vasculature has been documented in a dog, 13 and metastatic spread was reported in a canine myxosarcoma. 2,10 In the present case, the tumors within the pulmonary veins were direct extensions of the atrial mass and not of embolic or metastatic origin. Therefore, although CNC is classically associated with cardiac myxoma, we suggest that the diagnosis of myxosarcoma, instead of myxoma, based on histological features, would not disqualify this tumor from being a part of a CNC-like syndrome.
The diagnosis of adrenocortical adenoma in this case was based on size, partial fibrous encapsulation, compression of adjacent cortex, cytologic features, and presence of vascular spaces. 6 PPNAD, the adrenal lesion reported in human CNC, is characterized by lipofuscin pigment and multiple small adrenal nodules with internodular cortical atrophy. In contrast, the pigment within neoplastic adrenocortical cells in the present case was mainly hemosiderin, and the features are indicative of adrenocortical adenoma rather than PPNAD. 15 It is unlikely that the adrenal adenomas were caused by the ACTH-expressing pituitary hyperplasia, based on their multinodular appearance and the lack of evidence of hyperadrenocorticism.
Although we cannot exclude the possibility that the multiple lesions in this case were unrelated, the presence of cardiac myxosarcoma with proliferative endocrine lesions in this dog suggests a CNC-like condition. Mutations in the PRKAR1A coding sequence were not present. However, CNC is a genetically heterogeneous disease with only 40% of cases having mutations in the PRKAR1A gene 12 ; hence, the presence of other underlying genetic defects should not be ruled out. In summary, we describe a combination of cardiac myxosarcoma and extracardiac tumors in a dog, a spectrum of lesions with similarity to CNC in humans.
Footnotes
Acknowledgements
The assistance of Mary-Ellen Clark in DNA sequencing is highly appreciated. We thank Drs Rob Foster and Brian Wilcock for advice on histological interpretation and the University of Minnesota Veterinary Diagnostic Laboratory for performing the adrenocorticotrophic hormone immunohistochemistry.
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.