
Abstract
This report details a rare case of a frontal-ethmoid sinus mucocele with concurrent invasion of both anterior cranial fossa and orbital wall, manifesting primarily with ophthalmologic symptoms. A 64-year-old woman presented with right periorbital swelling accompanied with mild pain, photophobia, and epiphora. Endoscopic sinus surgery revealed extensive destruction of the skull base bone. Intraoperative findings included an intact dura mater without cerebrospinal fluid leakage. Histopathology identified a benign mucocele lined by respiratory epithelium. This case represents an exceptional presentation of a sinus mucocele with dual erosion into both anterior cranial fossa and orbital cavity. Endoscopic management achieved complete resolution without intracranial complications. This entity warrants consideration in patients with orbital symptoms and underlying sinus disease.
Introduction
A mucocele is a benign, slow-expanding lesion caused by the obstruction of the paranasal sinus ostia, most commonly occurring in the frontal and ethmoid sinuses. Although frequently asymptomatic initially, mucoceles may demonstrate progressive expansile growth, potentially compromising the adjacent orbital and intracranial structures when left untreated. Progressive bony erosion of the orbital walls or skull base can result in visual impairment, proptosis, and chronic pain. In advanced cases, intracranial extension may occur, which can compress the frontal lobe and induce neurological deficits.1,2 Herein, we report a rare case of a large frontal sinus mucocele that presented predominantly with ophthalmological manifestations.
Case report
A woman in her early 60s presented with a 2-day history of right periorbital swelling, accompanied with mild ocular pain, photophobia, epiphora, nausea, and nonprojectile vomiting of gastric contents. The patient denied headache or nasal symptoms such as congestion and rhinorrhea. She had undergone medical treatment at Liaocheng People’s Hospital in early 2025. Her medical history included a 9-year history of hypertension and type 2 diabetes mellitus, and an initial evaluation in the ophthalmology clinic revealed right eyelid edema, conjunctival injection, and impaired medial gaze. The right upper eyelid covered half of the cornea with elevated orbital tension (Figure 1). Visual acuity was 0.5 (right) and 0.6 (left), with intraocular pressures of 15 mmHg (right) and 17 mmHg (left). Her fundoscopic examination was unremarkable, and orbital computed tomography (CT) demonstrated outward and downward displacement of the right globe by a well-circumscribed, homogeneous cystic mass (5.6 × 3.5 × 6.9 cm) occupying the bilateral frontal and right ethmoid sinuses (Figure 2). The mass exhibited homogeneous density, eroded the medial orbital wall and frontal sinus floor, and displaced the posterior wall intracranially with anterior fossa bone destruction. Magnetic resonance imaging (MRI) revealed T2 hyperintensity, T1 hypointensity, and peripheral linear enhancement after contrast (Figure 3). The patient was diagnosed with a frontal sinus cyst invading the anterior cranial fossa and orbital wall. All routine preoperative examinations were completed preoperatively. Intraoperatively, nasal endoscopy revealed that the common nasal meatus of the right nasal cavity was occupied by a smooth-surfaced mass with a soft texture, and yellow cystic fluid was aspirated via puncture. During the procedure, the inferior wall of the mass was resected using biting forceps, and the cyst cavity was irrigated. Subsequent removal of the free inferior and lateral cyst walls revealed compression of the orbital wall and skull base, with evidence of partial bone resorption. The cephalad portion of the left leptomeningeal process was excised to expose and open the left frontal sinus, which communicated with the cystic cavity. Under nasal endoscopy, a resection and aspiration device was used to remove the cyst wall, ensuring adequate drainage and alleviating orbital pressure. Operative manipulation was performed gently to preserve the integrity of the dura mater without cerebrospinal fluid leakage. On postoperative day 3, nasal endoscopy was performed to clear the nasal secretions following thorough removal of the nasal packing. The ostia of all the paranasal sinuses were patent with unobstructed drainage. Postoperatively, the nasal cavity was irrigated with normal saline, and intranasal steroid sprays were administered to reduce nasal mucosal edema and inflammation. During the 3-month postoperative follow-up, nasal endoscopy revealed good paranasal sinus epithelialization, and the patient exhibited significant reduction in proptosis, normalization of the frontotemporal region, and restoration of ocular positioning, with no recurrence noted (Figure 4). We obtained signed consent for treatment and case publication from the patient.

Edema of the right eyelid and limited adduction of the right eye.

(a) Axial computed tomography (CT). (b) Coronal CT. The right eyeball is displaced outward and downward. Low-density shadows with clear boundaries and uniform density are observed in the bilateral frontal sinuses and the right ethmoid sinus cavities. Partial bone defects are observed on the floor of the frontal sinus, superior orbital rim, and anterior cranial fossa.
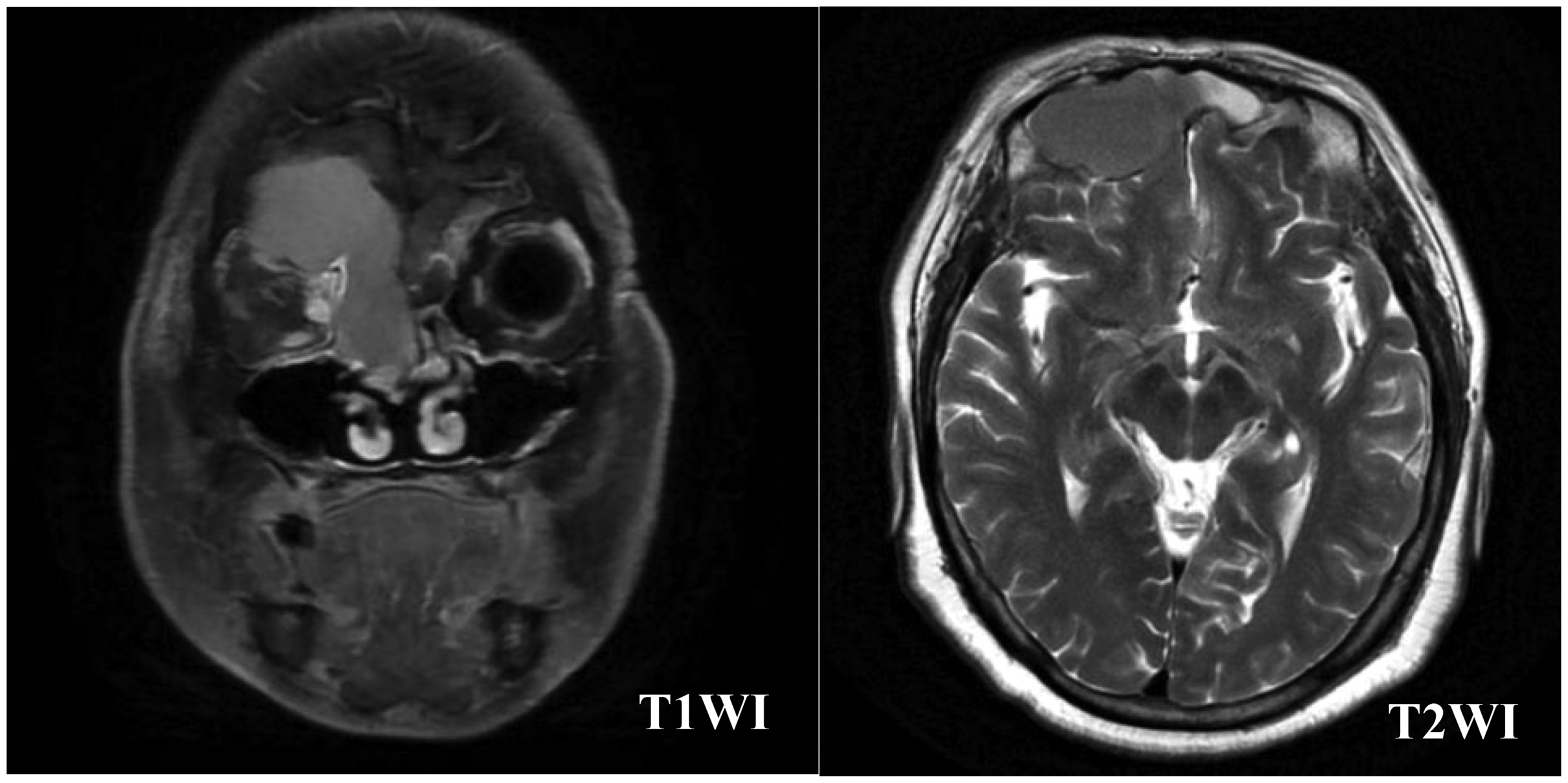
The coronal T1-weighted image demonstrates hypointensity, while the axial T2-weighted image shows hyperintensity. Compression of the frontal sinus floor and anterior cranial fossa is evident.
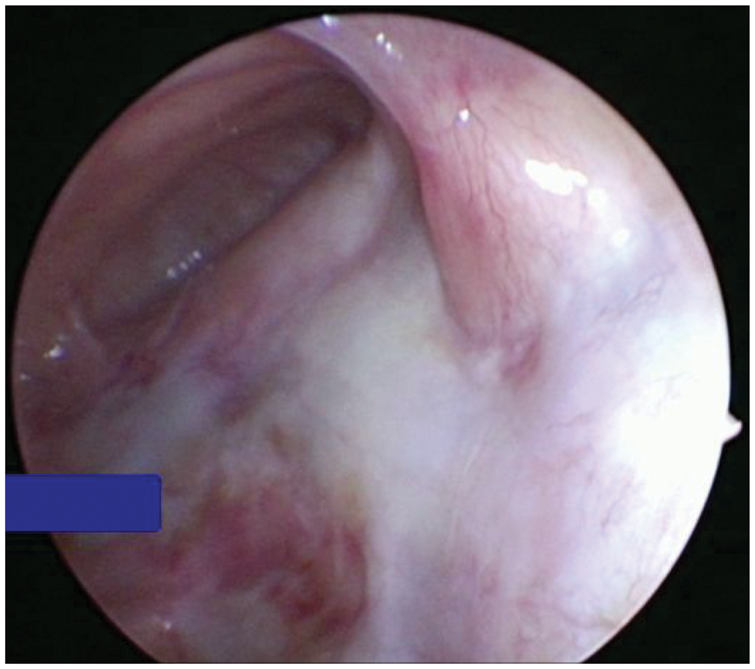
The nasofrontal canal was well opened postoperatively.
Discussion
Paranasal sinus mucoceles are benign, dilated, cystic lesions lined by a mucus-secreting respiratory epithelium. 1 In the presence of infection, these lesions may progress and form abscesses. 3 Mucous cysts most frequently arise in the frontal sinuses, likely due to the long, tortuous, and easily obstructed nature of the drainage pathways. The ethmoid sinuses are the second most common site of involvement. The primary etiology of frontal sinus mucoceles involves obstruction of the sinus ostia secondary to trauma or inflammatory changes, although in some cases, it may result from allergic reactions or postoperative complications.1,4 Although typically slow-growing, progressive mucus accumulation leads to expansion of the sinus walls and mass enlargement. Notably, cultured fibroblasts derived from frontal sinus mucosal cells demonstrate significantly elevated prostaglandin E2 and collagenase levels compared with normal frontal sinus mucosal fibroblasts. The increased prostaglandin E2 concentration appears to be particularly instrumental in promoting osteolysis, thereby explaining the invasive nature of mucoceles.2,4
The clinical manifestations of mucous cysts vary according to their anatomical location and typically present with an insidious onset. The signs and symptoms depend on cyst size, position, and degree of infiltration into adjacent structures. Patients with frontoethmoidal sinus mucous cysts may exhibit frontal headaches, facial asymmetry, localized swelling, or ocular manifestations, including visual impairment, restricted ocular motility, and proptosis secondary to orbital compression. Furthermore, the thin posterior wall of the frontal sinus is particularly prone to erosion, which may result in complications, such as meningitis and cerebrospinal fluid fistula, if breached. Large cysts compressing the frontal lobe can also induce neurological symptoms, including transient hemiparesis and seizures.1,4 In the present case, despite involvement of both anterior cranial fossa and orbital wall, the patient’s clinical presentation was dominated by ocular symptoms, primarily periorbital swelling, along with nausea and vomiting. These systemic symptoms may be attributable to compression of the frontal lobe.
If mucous cysts invade the orbital wall and base of the skull and cause bone destruction, they must be differentiated from malignant tumors of the paranasal sinuses, schwannomas, and other tumors. Squamous cell carcinoma is the most common malignant tumor of the nasal cavity and paranasal sinus mucosal epithelium. CT typically reveals an irregular unilateral soft tissue mass. The tumor is generally large, with heterogeneous density, ill-defined margins, and prominent bone destruction, leading to loss of the normal contours of the nasal cavity and paranasal sinuses. 5 Schwannoma is a predominantly benign tumor originating from the Schwann cells of peripheral nerves; the most common form is a unilateral tumor in the nasal cavity or paranasal sinuses. MRI typically shows isointensity or slight hypointensity on T1-weighted imaging (T1WI), whereas T2-weighted imaging (T2WI) shows heterogeneous hyperintensity, and the signal of the solid part is similar to that of the brainstem. Contrast-enhanced MRI shows moderate to marked homogeneous enhancement, and the cystic area shows no enhancement. 6
On CT, mucous cysts typically appear as homogeneous, isodense masses with well-demarcated margins and adjacent patchy osteolysis. Post-contrast imaging demonstrates no internal enhancement, although slight peripheral enhancement may be observed at the mucosal interface between the cyst and sinus wall. MRI characteristics vary depending on the protein concentration in the cystic fluid. On T1WI, the signal intensity ranges from hypointense (thin mucoid content) to hyperintense (protein-rich or concentrated fluid). T2WI typically shows hyperintensity, with even higher signal intensity observed in cases of thin, watery cystic fluid. The superior soft tissue resolution of MRI proves particularly valuable for excluding neoplastic processes in large mucous cysts. 7 In the present case, after the inferior border of the lesion was resected, an effusion of thin, yellow cystic fluid was observed. The fluid was watery in consistency and had a low protein concentration; consequently, it presented as hypointensity on T1WI and hyperintensity on T2WI. Despite the substantial lesion size and partial bone destruction, CT revealed a well-circumscribed, homogeneous cystic mass. The corresponding MRI demonstrated T2 hyperintensity and T1 hypointensity. Because of the patient’s personal preferences and clinical urgency, contrast-enhanced MRI was not performed. Based on the two imaging examinations, the possibility of squamous cell carcinoma or schwannoma was determined to be low. Our preliminary clinical diagnosis was a sinus mucous cyst, which was confirmed on postoperative pathological examination.
With advances in nasal endoscopic techniques, minimally invasive endoscopic sinus surgery (ESS) has emerged as the primary treatment. The surgical principle involves the removal of only pathological tissues or abnormal structures causing sinus obstruction while sufficiently enlarging the sinus ostium to ensure adequate cystic fluid drainage without complete excision of the residual cystic wall tissue. ESS offers significant advantages by minimizing sinus trauma, preserving the normal sinus anatomy, preventing external scarring, and facilitating postoperative endoscopic surveillance. However, open surgery remains the preferred approach for complex cases, including recurrent mucoceles, large mucoceles with intracranial extension, or lesions located in the far posterior–superior aspect of the sinuses.7,8 In the present case, ESS was successfully performed with adequate sinus drainage. Intraoperative exploration revealed anterior cranial fossa bone erosion with an intact dura mater without cerebrospinal fluid leakage. Postoperative follow-up demonstrated marked resolution of the right periorbital swelling and restoration of normal ocular motility.
Although sinus mucous cysts are generally regarded as benign lesions amenable to elective management, prompt intervention is warranted when inflammation or a symptomatic presentation exists. Frontal sinus mucous cysts frequently manifest with ocular rather than nasal symptoms in the early stages. This clinical pattern underscores the importance of considering rhinogenic pathology in the differential diagnosis of unexplained proptosis and visual disturbances. The absence of characteristic nasal symptoms may delay the diagnosis, emphasizing the need for a comprehensive evaluation that incorporates appropriate imaging modalities for cases with such ocular presentations. The reporting of this study conforms to the Case Report (CARE) guidelines. 9
Footnotes
Acknowledgments
I sincerely thank my tutor Li Lianqing for his valuable advice and careful guidance on the revision of the article, and thank all the authors for their selfless help in data collection.
Authors’ contributions
Siyu Liu: data collection and article preparation; Siyu Liu, Yu Feng, and Maocai Li: article preparation; Siyu Liu: picture collection; and Li Lianqing and Lili Gong: article preparation and review. All authors have read and approved the final manuscript.
Data availability statement
Not applicable.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, or publication of this article.