
Abstract
Primary squamous cell carcinoma of the liver is extremely rare, very difficult to diagnose, and carries an extremely poor prognosis. In this study, we discuss the imaging features of a patient with primary hepatic squamous cell carcinoma. The patient was admitted to hospital owing to discomfort in the right upper abdominal quadrant and a loss of appetite. He had no previous risk factors associated with hepatic squamous cell carcinoma and no history of systemic squamous cell carcinoma. We diagnosed primary hepatic squamous cell carcinoma by pathological analysis. Primary hepatic squamous cell carcinoma is rare, and its histological features are controversial, which makes the clinical and imaging diagnosis difficult. Therefore, it is urgent to improve the understanding of this disease in clinical practice to avoid misdiagnosis, and to identify the best treatment. This case provides a basis for the clinical diagnosis of primary hepatic squamous cell carcinoma.
Introduction
Squamous cell carcinoma occurs in areas of the body covered by squamous epithelium. Because there are no squamous epithelial cells in the liver, primary hepatic squamous cell carcinoma is rare in this location. Early diagnosis is difficult owing to a lack of specific clinical and imaging characteristics. 1 Furthermore, the histological source of primary liver squamous cell carcinoma is controversial. Squamous cell carcinoma antigens are elevated in some patients, but a correlation remains undetermined. 2 Patients with primary hepatic squamous cell carcinoma usually have a poor prognosis and are not sensitive to radiotherapy and chemotherapy. 3 Treatment options constitute surgical resection, liver transplantation, radiotherapy, interventional local chemotherapy, and radiofrequency ablation. 4 In this study, we analyzed the imaging data of a patient with primary hepatic squamous cell carcinoma.
Case report
The reporting of this study conforms to the CARE guidelines. 5 A 73-year-old male patient was admitted to the hospital with “abdominal right upper quadrant discomfort and loss of appetite for 15 days”. There was no fever. His sleep and diet were of poor quality, and were accompanied by a significant reduction in body weight of approximately 10 kg in 15 days. He had no history of hepatitis or cancer. Physical examination revealed no jaundice, palmar erythema, or spider naevi. Neither the liver nor spleen were palpable, and negative percussion tenderness was present over the liver, with no shifting dullness.
Laboratory tests revealed a markedly elevated squamous cell carcinoma antigen concentration of 17.44 µg/L (reference value: <1.5 µg/L). No abnormalities were found in the other indicators. There was a slightly-low-density mass in the right liver lobe, with a lobulated contour and blurred borders. The mass measured approximately 7.3 cm × 3.8 cm and had a mean density of 36 Hounsfield units (HU) during pre-contrast computed tomography (CT) (Figure 1a). Enhancement revealed shallow lobulation in the lesion, and during the arterial phase, the edge and the center of the lesion were mildly enhanced (Figure 1b). During the portal and delayed phases, the center of the lesion showed continuous enhancement (Figure 1c). The CT values in the arterial, portal, and delayed phases were 63.2 HU, 80.6 HU, and 87.9 HU, respectively. There were no stones and no dilatation of the intrahepatic bile ducts, and no filling defects were found in the portal vein. Both kidneys had a circular cystic lesion, and the larger one measured approximately 0.6 cm in diameter. No enhancement was observed during enhanced CT, and a small lymph node was observed next to the abdominal aorta. The CT diagnosis was: 1) space-occupying malignant lesion in the right liver lobe, and 2) cysts in both kidneys.
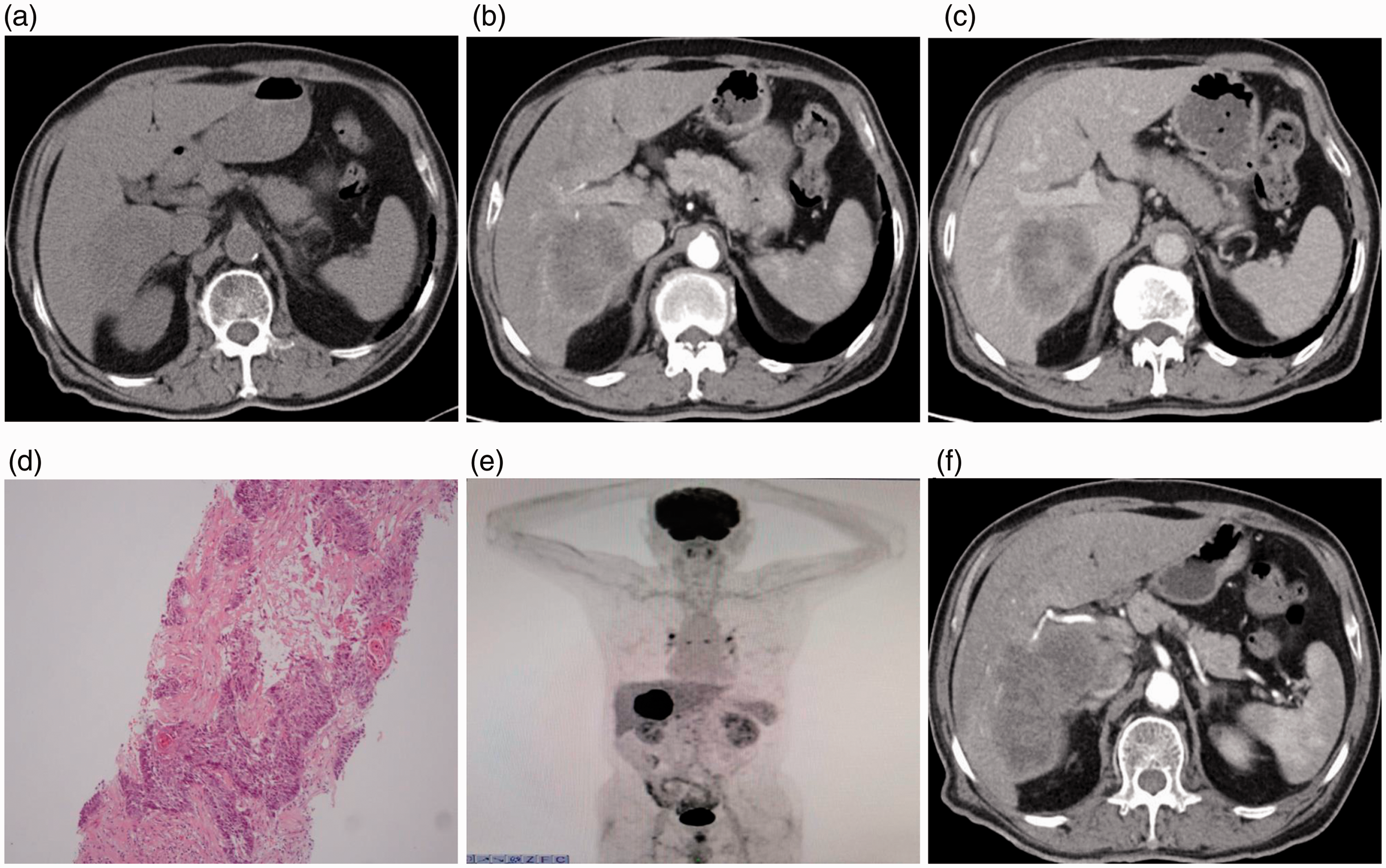
The imaging characteristics in the present case. (a) A slightly-low-density mass is seen in the right liver lobe, with unclear boundaries. (b) During the arterial phase of enhanced computed tomography (CT), mild enhancement at the edge and in the center of the lesion are seen. (c) Continuous enhancement of the center of the lesion during the delayed phase. (d) Microscopically (hematoxylin and eosin (HE) ×100), the tumor cells are nest-shaped and contain mitotic figures. Desmosomes (intercellular bridges) are present between the tumor cells, and keratin pearls are visible. (e) Positron emission tomography (PET) image showing that the metabolism of the right liver lobe mass is significantly increased. (f) Image 2 months later showing that the lesion has increased significantly in size.
Hematoxylin and eosin (HE) staining of liver biopsies showed that the tumor cells were nest-shaped and exhibited abnormal nuclear morphology. Desmosomes (intercellular bridges) were observed between tumor cells, accompanied by keratinization as keratin pearls (Figure 1d). Immunohistochemistry showed that the tumor cells were hepatocyte paraffin-1 (HepPar-1 (−), cytokeratin (CK)7 (−), P63 (+), and P40 (+). The pathological diagnosis was squamous cell carcinoma of the liver. Subsequent 18F-fluorodeoxyglucose positron emission tomography/CT (18F-FDG PET/CT) imaging showed significantly increased metabolism in the right liver lobe mass, with a maximum standardized uptake value for 18F-FDG of 20.1 (Figure 1e), while 18F-FDG uptake was slightly increased in the para-aortic, bilateral lung, and mediastinal lymph nodes. However, no abnormal uptake was observed in other regions; therefore, the possibility of metastasis from other systems was ruled out. The final diagnosis was squamous cell carcinoma of the liver. The patient refused surgery or interventional therapy, and requested to be discharged from the hospital and was treated with traditional Chinese medicine. During this treatment, his condition worsened, and he was admitted to the hospital 2 months later. CT revealed that the right liver lobe mass was significantly larger, measuring approximately 10.1 cm × 5.2 cm (Figure 1f). The patient declined treatment and was discharged from the hospital. One week after discharge, he underwent argon helium cryoablation of the right lobe malignant tumor in Beijing Eurasian Cancer Hospital (Beijing, China). He developed fatigue in the most recent month and lost consciousness 2 weeks later. He was re-admitted and received conventional liver protection treatment.
Discussion
Primary hepatic squamous cell carcinoma is very rare and is associated with high malignancy and a poor prognosis. The majority of patients are elderly men, and the average survival time is less than 1 year. 6 The clinical manifestations of primary squamous cell carcinoma of the liver lack specificity, and the disease often manifests as pain in the abdominal right upper quadrant, with jaundice, loss of appetite, and weight loss. Tumor marker expression in primary hepatic squamous cell carcinoma is generally negative; however, the diagnosis of squamous cell carcinoma can be indicated if the squamous cell carcinoma antigen concentration is elevated. The source of primary hepatic squamous cell carcinoma is controversial. Most studies suggest that primary hepatic squamous cell carcinoma is related to congenital benign non-parasitic hepatic cyst, 7 intrahepatic bile duct stones, 8 chronic cholangitis, congenital biliary cyst, 9 cirrhosis, and liver teratoma. 10
The development of most squamous cell carcinomas is thought to be related to squamous metaplasia and the progressive carcinogenesis of epithelial cells from the biliary tract or cyst wall under the stimulation of chronic inflammation.11,12 In this study, the patient had no risk factors associated with primary squamous cell carcinoma of the liver, such as cirrhosis and biliary system diseases. It has also been reported that liver pluripotent stem cells may transform into cancerous tissues containing squamous cells, hepatocytes, and biliary epithelial cells under the action of various carcinogenic factors, with the cells then developing into squamous cell carcinoma. 13 Therefore, we consider that the squamous cell carcinoma in this case may have derived from pluripotent stem cells. According to Carrim and Murchison, 14 patients with hepatic cysts have a greater probability of having a renal cyst compared with the baseline prevalence. Our patient had cysts in both kidneys. Thus, we speculated that a liver cyst was present before the formation of the liver tumor, and that the cyst underwent carcinogenesis after epithelial metaplasia.
Through a literature search,13,15,16 we summarized the CT imaging findings of primary squamous cell carcinoma of the liver. Most patients had a slightly-low-density mass, and a few cases were associated with cysts. Enhanced imaging showed uneven or mild enhancement or marginal enhancement in the lesion during the arterial phase. The portal and delayed phases were persistently enhanced, and patients sometimes also had intrahepatic bile duct stones, intrahepatic bile duct dilatation, and hepatic cysts. The patient in this study had no hepatic cyst, or intrahepatic bile duct stones or dilatation. However, the patient's right liver lobe contained a slightly dense mass, and hepatic capsular retraction syndrome was present. Enhanced imaging showed that the lesion was enhanced at the lesion edge during the arterial phase, with lobulation. The center of the lesion was slightly enhanced, and continuously enhanced in the delayed phase.
Primary hepatic squamous cell carcinoma must be distinguished from the following three diseases: 1) cholangiocarcinoma, which occurs adjacent to the capsular retraction of the liver, is surrounded by bile duct dilatation, and is accompanied by delayed phase enhancement. Squamous cell carcinoma antigen detection may facilitate the differential diagnosis. 2) Liver metastases. Affected patients usually have a history of primary tumors, and there is marginal enhancement of the tumor during enhanced imaging. The typical manifestation is “bull’s eye syndrome”. When the tumor is large, it often protrudes from the liver surface, and rarely, shows hepatic capsular retraction syndrome. 3) Liver abscess. CT imaging of liver abscesses generally shows round, low-density lesions. With enhancement, the wall of the abscess is enhanced, but the surrounding edema is not enhanced, and a ring sign is formed. The normal tissue around the abscess is transiently enhanced; liver abscess is accompanied by fever and elevated white blood cell counts.
In conclusion, primary hepatic squamous cell carcinoma is a refractory and rare hepatic heterogeneous malignant tumor, which is difficult to diagnose clinically and with imaging. Primary squamous cell carcinomas, such as in the respiratory tract, and digestive, gynecological, and urinary systems must be excluded, and pathological and immunohistochemical methods can be used to confirm the final diagnosis.
Footnotes
Ethics statement
This study was approved by the ethical review board of Yanbian University Affiliated Hospital. Written informed consent was obtained from this patient for publication of this case.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Natural Science Foundation of China (81860304).
Author contributions
Conceptualization: Guangyu Jin
Data curation: Yu Sun
Investigation: Yu Sun
Methodology: Yu Sun
Project administration: Guangyu Jin
Supervision: Guangyu Jin
Writing – Original Draft: Yu Sun
Writing – Review & Editing: Guangyu Jin