
Abstract
Objective
To examine the clinical effects of revision endoscopic frontal sinus surgery (RESS) through modified agger nasi (MAN)–middle turbinate resection on refractory chronic rhinosinusitis (CRS).
Methods
We reviewed 156 patients who were treated for refractory CRS from February 2012 to August 2014. These patients had been diagnosed with refractory CRS by computed tomography and endoscopy and had received several surgical and medical treatments in the past, but their condition had not been cured. They were divided into the observation group (RESS through MAN–middle turbinate resection, n = 78) and the control group (endoscopic sinus surgery, n = 78). Complete or partial control of the patient’s symptoms and signs suggested that the treatment was effective, and no improvement in the symptoms and signs indicated that the treatment was ineffective.
Results
The 6-month treatment efficacy rate was significantly higher in the observation group (91.03%) than in the control group (71.79%). The observation group had a significantly lower complication rate (7.69%) and recurrence rate (3.85%) than the control group (17.95% and 12.82%, respectively).
Conclusion
RESS through MAN–middle turbinate resection together with adequate perioperative preparation has a significant effect on the outcome of refractory CRS and is worthy of clinical promotion.
Keywords
Introduction
Refractory chronic rhinosinusitis (CRS) is characterized by persistent CRS, purulent sinuses, facial pain, and/or dysosmia. The main cause is the inflammatory response to colonizing bacteria. CRS in children has a great impact on public health in the United States, and reducing the bacterial load and mucosal inflammation plays an important role in controlling the disease. It is estimated that more than $2 billion in over-the-counter drugs are used annually for CRS treatment. 1 Refractory CRS affects nearly 31 million Americans each year, involving approximately 20 million clinic visits and 200,000 sinus surgeries per year. 2 New strategies that emphasize local treatment seem to be the most effective.3,4 Local sinus corticosteroid administration and high-volume saline flushing remain the cornerstones of drug therapy, and the use of systemic corticosteroids and antibiotics depends on the phenotype of the refractory CRS and whether its onset is acute. Anti-interleukin-4 receptor alpha antibodies and calcium channel blockers have achieved satisfactory initial results in the treatment of refractory CRS. Appropriateness criteria have been used to help clinicians determine which patients with refractory CRS can be candidates for endoscopic sinus surgery. 5 Revision endoscopic frontal sinus surgery (RESS) is an effective surgical approach for patients who have undergone failed drug therapy, and approximately 85% of patients can reportedly achieve reduced symptoms and improved quality of life both immediately and in the long term.6,7 RESS through modified agger nasi (MAN)–middle turbinate resection has been used to treat refractory CRS. However, RESS may destroy the normal anatomical structure of the nasal cavity and paranasal sinuses, and the most effective surgical landmarks remain unclear.
The results of RESS have been significantly improved with advances in technology, improved surgical training, and a better understanding of the pathophysiology of the disease. Complications of RESS include cerebrospinal fluid leakage, meningitis, bleeding, and eyelid damage. 8 In this study, we retrospectively analyzed the clinical data of 78 patients with refractory CRS who underwent RESS through MAN–middle turbinate resection and compared the efficacy of their treatment with that of 78 patients with refractory CRS who underwent endoscopic sinus surgery during the same period. The clinical effect of RESS through MAN–middle turbinate resection on refractory CRS was evaluated.
Materials and methods
Clinical data
The inclusion criteria for this study were a history of multiple surgical operations and medical treatments with no curative effect, the absence of other diseases, and the absence of factors affecting the curative effect. The exclusion criterion was no history of surgery during the first hospitalization.
In total, 156 patients with refractory CRS (89 men, 67 women) aged 21 to 72 years (mean, 42.2 ± 10.7) were included in this study. The disease course ranged from 3 to 36 years (mean, 12.3 ± 4.2 years). In accordance with the clinical classification standard, 9 all patients had type III and stage III CRS. The patients were randomly divided into the observation group (OB group) (n = 78) and the control group (n = 78). The OB group comprised 45 men and 33 women with a mean age of 41.2 ± 6.8 years and mean disease course of 11.7 ± 5.6 years. Ten patients had hypertension and coronary heart disease and three patients had diabetes in the OB group. The control group comprised 44 men and 34 women with a mean age of 43.1 ± 9.2 years and mean disease course of 13.6 ± 2.9 years. Eleven patients had hypertension and coronary heart disease and two patients had diabetes in the control group. All patients had a history of surgery for sinusitis. There were no significant differences in sex, age, disease duration, disease classification, complications, or surgical history between the two groups (Table 1). The Ethics Committee of the Affiliated Huai’an Hospital of Xuzhou Medical University approved the study protocol, and all patients provided written informed consent.
Demographic data.

Data are presented as n or mean ± standard deviation.
OB, observation; CRS, chronic rhinosinusitis.
Therapeutic method
One week before the surgery, all patients underwent nasal irrigation with ceftriaxone, nasal spraying with beclomethasone propionate, and oral administration of prednisone. The underlying diseases in patients with coronary heart disease and hypertension were controlled proactively. All patients received general anesthesia and were maintained in the reverse Trendelenburg position at 15° to 30°. Cotton fleece with anesthetic (12 mL of 10% lidocaine and 0.6 g of 5% oxymetazoline) was placed into the nasal cavity for 10 minutes, and then 0.01% adrenaline diluted by normal saline was injected into the local mucosa of the surgical site. The appropriate surgical method was selected based on the degree and location of sinusitis and nasal polyps. During the procedure, the remaining anatomical structures and lesions of the key anatomical sites, such as the anterior arch, posterior sinus arch, maxillary sinus ostium, and ridge below the eye socket, were carefully examined under nasal endoscopy.
In the OB group, RESS through MAN–middle turbinate resection was performed as follows. The polyps at the anterior arch or middle nasal concha were completely or partially resected according to the degree of hyalinosis and its impact on drainage of the nasal valve. The remaining uncinate process was then resected, or the maxillary sinus aperture was expanded to fully open the front and back naso-orbital-ethmoid regions. At the fornix position of the middle nasal meatus, the mucus and the agger nasi cell were removed in an upward direction with a 45° sphenoid sinus rongeur until the frontal bone could be touched; the resection height was about 1.0 cm. The agger nasi air cells, which are the most anterior ethmoidal air cells lying anterolateral and inferior to the frontal recess and anterior to and above the attachment of the middle turbinate, were thoroughly eliminated until the bottom of the frontal sinus was completely opened. An electric drill was used to open the frontal sinus, sphenoid sinus, and maxillary sinus to ensure that the mucosa of the aperture to the mastoid antrum was not closed after surgery. For patients with a deviated septum, three-line tension-reducing septorhinoplasty 10 or limited corrective resection was employed; for patients with allergic rhinitis, electrocoagulation was conducted toward the mucous membrane at the positions of the front end of the inferior nasal concha and the nasal septum of the middle nasal concha. The nerve of the pterygoid canal was cut off when necessary. For patients with a deviated nasal septum and adhesion of the nasal cavity, traditional (endoscopic sinus surgery) or circumscribed treatment of septal deviation and adhesion separation were employed.
In the control group, endoscopic sinus surgery was performed as follows. Paranasal sinus surgery was performed via the front-to-back approach. The nasal cavity fillings were removed 1 to 2 days postoperatively, and the nasal cavity was cleaned with normal saline and cleared under endoscopy 6 to 10 days postoperatively.
In accordance with the standard system we established, the follow-up data were collected by a designated person who was blinded to the patients’ information.
Efficacy evaluation criteria
The efficacy rate, complication rate, and recurrence rate after surgery were compared between the two groups in line with the 2012 Kunming CRS diagnosis and treatment guide. 11 Efficacy was classified as follows. (1) Full control of the condition: the symptoms disappeared completely, endoscopy showed that all visible epithelization of the sinus cavity mucosa and sinus mucosal edema had disappeared, the aperture to the mastoid antrum was adequately open, and no purulent secretion was present. (2) Partial control of the condition: the symptoms were obviously improved but had not completely disappeared; endoscopy showed that part of the sinus cavity mucosa had edema, tissue thickening, or granulation tissue; and a small amount of purulent secretion was present. (3) No control of the condition: the symptoms were not improved, and endoscopy showed cavity adhesion, sinus stenosis or atresia, polyps, or purulent secretion. The criteria of (1) and (2) indicated that the treatment was effective, and the criteria of (3) indicated that the treatment was not effective.
Statistical analysis
All measured data are presented as mean ± standard deviation and were analyzed with the Mann–Whitney U test. Enumeration data were analyzed with the chi-square test using PASW Statistics for Windows, Version 18.0 (SPSS Inc., Chicago, IL, USA), and a P value of <0.05 was considered statistically significant.
Results
Comparison of therapeutic effects between the two groups
Six months after surgery, the total efficacy rate was 91.03% in the OB group and 71.79% in the control group, with a significant difference between the two groups (P < 0.05) (Table 2, Figures 1 and 2).
Comparison of therapeutic effects between the two groups.

OB, observation.

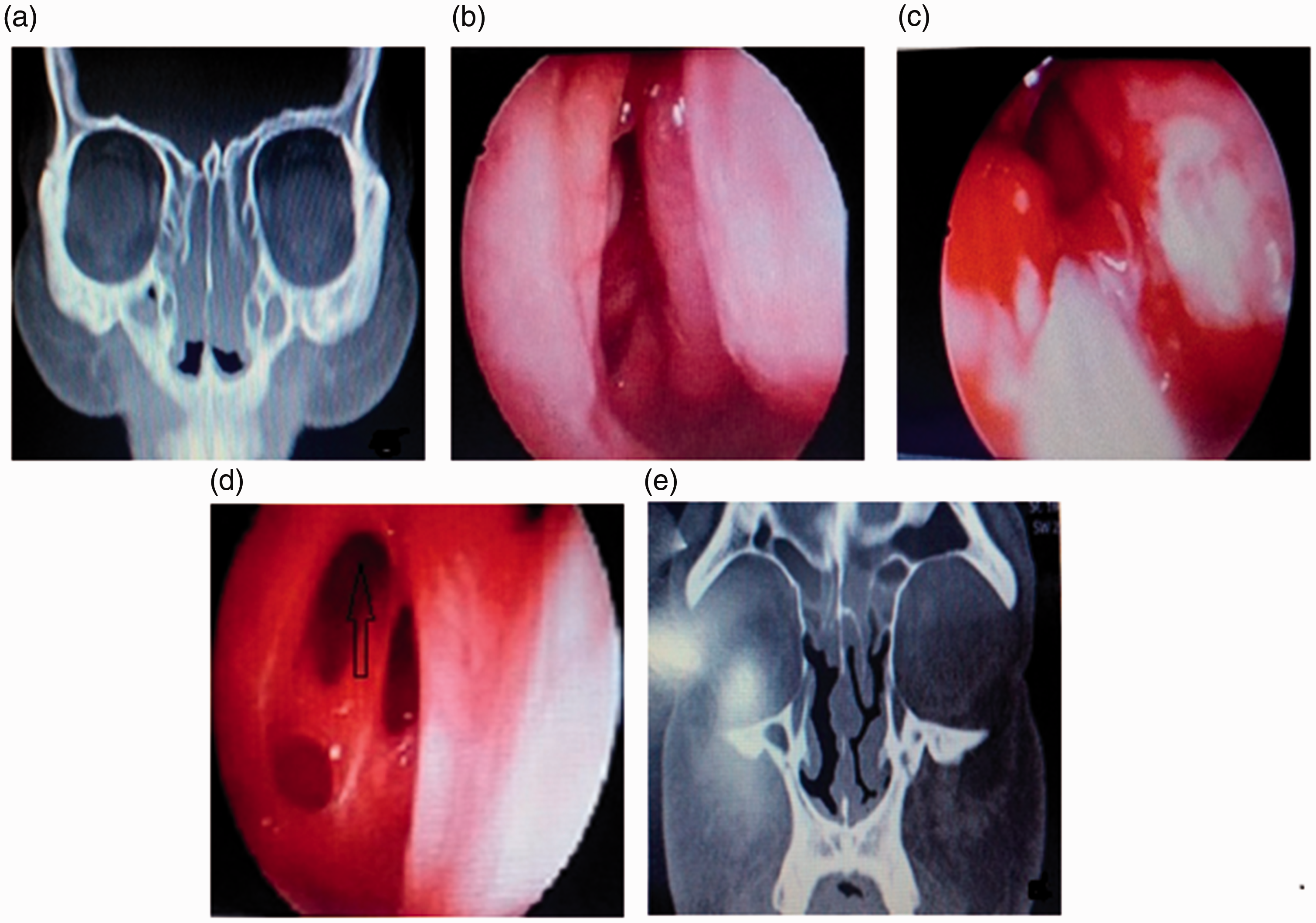
Images of a 52-year-old female patient. RESS through MAN–middle turbinate resection was performed to treat recurrent obliterating inflammation of the maxillary sinus, ethmoidal cells, and frontal sinuses of both sides. (a) The preoperative coronal computed tomography scan indicated obliterating inflammation of the maxillary sinus, ethmoidal cells, and frontal sinuses of both sides. (b) The preoperative nasal endoscopic examination indicated synechia of the right nasal cavity and polypoid change of the middle turbinate. (c) During surgery, the synechia was separated, the partial middle turbinate was resected, and the right frontal sinus was opened via the MAN approach. (d) At the 6-month postoperative follow-up visit, the right frontal sinus was adequately open, and the wound cavity showed good epithelization. (e) The right frontal sinus and maxillary sinus were adequately open.
Images of a 46-year-old female patient. Endoscopic sinus surgery was performed to treat obliterating inflammation of the maxillary sinus, ethmoidal cells, and frontal sinuses of both sides as well as deviation of the nasal septum. (a) The preoperative coronal computed tomography scan indicated obliterating inflammation of the maxillary sinus, ethmoidal cells, and frontal sinuses of both sides as well as deviation of the nasal septum. (b) The preoperative nasal endoscopic examination indicated recurrence of a polyp in the right middle nasal meatus and deviation of the nasal septum. (c) After opening the right maxillary sinus, ethmoidal cells, and frontal sinus, purulent secretion was noted. (d) Six months postoperatively, endoscopic examination showed that the right middle nasal meatus synechia was still present and that the frontal sinus was still closed. (e) The postoperative follow-up computed tomography scan revealed inflammation of the ethmoidal cells, maxillary sinus, and frontal sinus and showed that the deviation of nasal septum had not been corrected.
Comparison of complication and recurrence rates between the two groups
The complication and recurrence rates were significantly lower in the OB group than in the control group. In the OB group, there was one case of nasal cavity adhesion, two cases of periorbital cyanosis, one case of sinus atresia, two cases of nasal dryness, and three cases of recurrence. In the control group, there were three cases of nasal cavity adhesion, four cases of periorbital cyanosis, two cases of sinus atresia, one case of rectus muscle injury, four cases of nasal dryness, and 10 cases of recurrence. The differences between the two groups were considerable (P < 0.05) (Table 3).
Comparison of complications and recurrence of refractory CRS between the two groups.

CRS, chronic rhinosinusitis; OB, observation.
Discussion
Surgical treatment for refractory CRS is designed to eliminate local edema and hyperplasia or inflammatory polyps in the nasal cavity and paranasal sinuses, thus improving ventilation and drainage.12,13
General treatment
Special attention to perioperative treatment is needed for patients with refractory CRS. Nasal irrigation, nasal spraying with budesonide, and oral administration of prednisone should be continued for at least 1 week in addition to controlling any underlying systemic diseases. For patients with underlying diseases such as asthma, a group consultation should be carried out to determine how to adjust the patient’s medications. Patients must be thoroughly instructed in self-care after nasal endoscopic surgery and should strive for a good understanding of their disease; in particular, clinicians should ensure that patients comply with regular follow-up re-examinations after surgery. Before the surgery, the extent of disease and the surgical procedures must be assessed according to the endoscopic examination and paranasal sinus CT findings. Anatomic landmarks such as the anterior arch, ostium of the maxillary sinus, and others must be clearly identified. In cases of severe bleeding or indistinct structures, the surgeon should perform all procedures very carefully and suspend the surgery if necessary. The surgeon should also communicate with the anesthesiologist if needed and carefully study the sinus CT findings to avoid serious complications. In the present study, patients in both groups continued receiving preoperative medication and other treatments for 1 week. The first cavity clearing was performed 1 to 2 weeks before surgery, mainly to clear old hematomas and secretions.
Follow-up treatment
The treatment interval after discharge is generally not less than 2 weeks, and the total treatment time is 3 to 6 months. Dressing changes should be performed through endoscopy at each follow-up visit, and any necessary interventions should be performed for sinus edema or other problems. For patients with allergic rhinitis, the duration of treatment with oral mucolytic agent and prednisone should be extended. An antihistamine and leukotriene receptor antagonist should be added when necessary, and the duration of anti-inflammatory treatment should be no less than 12 weeks. Some patients achieve epithelization of the cavity during postoperative follow-up. However, when allergic rhinitis develops, patients are likely to develop increased mucous membrane edema, vesical hyperplasia, and delayed cavity epithelization. After local treatment and drug treatment, the epithelium can be restored. Therefore, regular follow-ups and specific drug treatments are essential to ensure a good outcome.
Comprehensive treatment
RESS through MAN–middle turbinate resection for refractory CRS conducted by Huai et al. 12 and Schaefer and Close 14 achieved quite good effects. After 6 months of follow-up visits in the present study, the total efficacy rate was higher in the OB group than in the control group, and the ineffective rate was lower than in the control group. This sufficiently proves that the curative effect of RESS through MAN–middle turbinate resection for refractory CRS is reliable. This is consistent with the findings of Huai et al. 12
Complication and recurrence rates
Both the complication and recurrence rates were much lower in the OB group than in the control group (P < 0.05). Treatment improved the quality of life of patients with refractory CRS, consistent with the report by Zhao and Qin. 13 Frontal sinus lesions in patients with refractory CRS are quite severe, and the recurrence rate of sinus atresia is high after endoscopic sinus surgery. The frontal recess is the most difficult location for endoscopic sinus surgery and is the most common cause of surgical failure. The frontal recess of Chinese patients is relatively narrow, increasing the risk of postoperative mucosal edema. If the treatment is improperly performed or not performed in a timely manner, sinus atresia is more likely to recur.
RESS through MAN–middle turbinate resection
The theoretical foundation of RESS through MAN–middle turbinate resection is that the superior wall of the agger nasi cell is the bottom of the frontal sinus, and the anterior wall is the frontal recess. We performed the frontal sinus surgery through the MAN approach: under visualization with a 0° endoscope, we used a 45° sphenoid sinus rongeur to remove the tissue in an upward direction from the front fornix of the middle nasal meatus, thus opening the agger nasi. Our procedure facilitates quick entry into the frontal sinus for resection of the upper foundation of the middle nasal concha and complete opening of the bottom of the frontal sinus. Compared with frontal sinus surgery through the approach of centering the uncinate process of the ethmoid bone, the agger nasi approach uses nasal endoscopy with a smaller angle. In addition, it is easier to expose the inside wall of the frontal sinus by resecting the upper adhesion from the middle nasal concha and bottom wall of the inner frontal sinus. According to CT assessment, endoscopic frontal sinusotomy has a better curative effect than uncinate process sinusotomy, which requires a 30° or 70° endoscope. It is simpler and more feasible to conduct endoscopic frontal sinusotomy with a 0° endoscope in primary hospitals, and the curative effect is better.
RESS through MAN–middle turbinate resection has a higher efficacy rate for refractory CRS for several reasons. First, the sufficient perioperative preparation and use of the self-compiled nasal endoscope health care manual used in the hospital promote patient compliance during the perioperative period and follow-up. Second, partial or full resection of the middle nasal concha markedly reduces the recurrence rate of adhesions and polyps, and the reduction in polyp recurrence is not accompanied by an increase in postoperative adverse effects. 15 Third, in patients with a deviated nasal septum, the application of endoscopic sinus surgery or limited revision resection plus inferior nasal concha fracture and relocation can expand the operative space and facilitate better drainage from the paranasal sinus to the nasal cavity. Finally, endoscopic frontal sinusotomy can be more easily performed using a 0° endoscope, which is simple and intuitive and avoids the recurrence of frontal sinus atresia.
Conclusion
RESS through MAN–middle turbinate resection in combination with comprehensive perioperative treatment and follow-up can improve the efficacy rate for refractory CRS and effectively prevent recurrence of rhinosinusitis and polyps. The operation is easy to master, the field of vision is clear, mucous patches are not required, and the operation is relatively short. Therefore, RESS through MAN–middle turbinate resection is promising in terms of clinical application and promotion. The main limitation of this surgical technique is the high level of surgical trauma; thus, the surgical indications should be strictly controlled.
Footnotes
Acknowledgment
We thank all patients who participated in this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Huai’an Science and Research Foundation of Jiangsu Province (HA2013032).